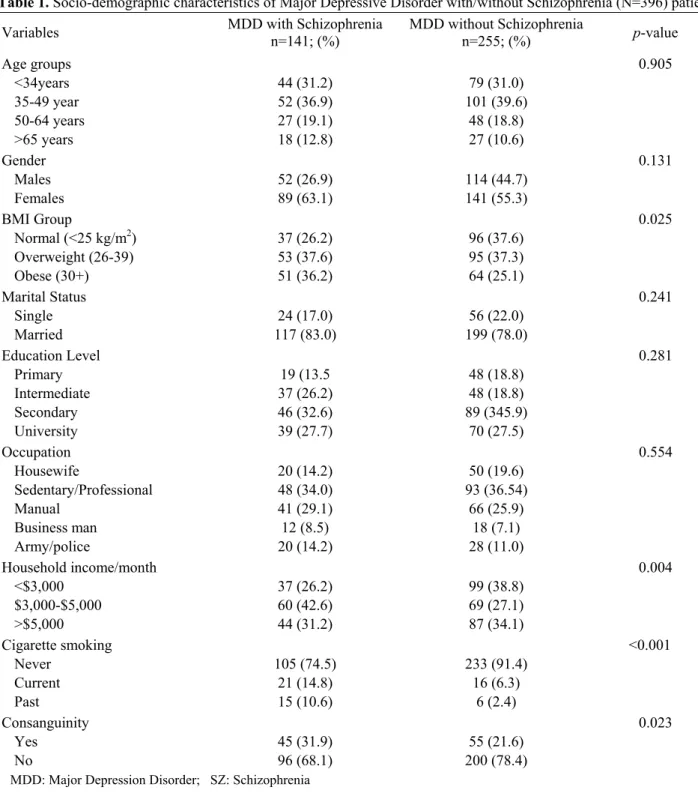
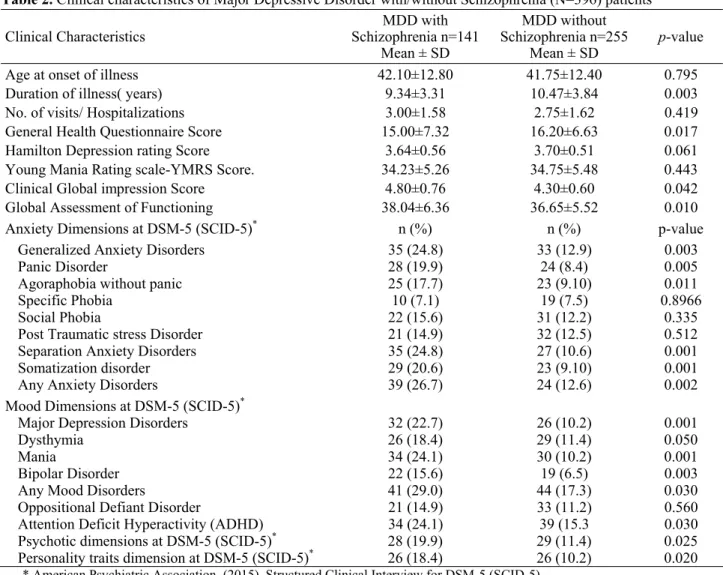
Co-Morbidity between major depression and schizophrenia: Prevalence and clinical characteristics
Tam metin
Şekil
Benzer Belgeler
Kraliçe Kral Kuğu Çalgı Yunus Andromeda Balıklar Büyük Kare Balina Pompa Güneybalığı Kova Kanatlı At Kertenkele Kalkan Kartal Yılancı Yılan Yay Kuzey Tacı Vega
Fevzi Paşa’ya ismet Paşa’nın bana Musul’u almayı teklif ettiği ni, bunun daha önce de Gazi ta rafından yapıldığını anlattım.. Hayret etti ve bana
W n O'nu bıraktığımız yerde, yalnız servilerin değil, denizin de getirdiği serinlik vardı. Bu yerj iıki gün önce seçmişti. Bir parça güneş duruyordu
SETI, "Sabırsız" Yardımcılardan Dertli Test kütlesi Test kütlesi Lazer Demet ayırıcı Fotodedektör Test kütlesi Test kütlesi Işık depolama kolu Işık depolama
on ların yaptıkları, ha bunlar doğrudur, bu suretle vaniış Türk m otifidir diye çalışıp eser verenlerin de bu suretle artık tutul madıkları ve bunu
Birinci basamak vizyonunu ortaya koyan politika dokümanlarının yayımlanması (örneğin Aile Hekimliği Türkiye Modeli), kanun ve yönetmeliklerle birinci basa-
Despite its importance and the many modern educational trends and the emphasis of many educators on it, the actual reality of its teaching is still characterized by
It is customary to tease by keeping a dress & Origin in the community and looking at Vadivelu, who comes with love and teasing him like a Ghost, discriminating as red and
