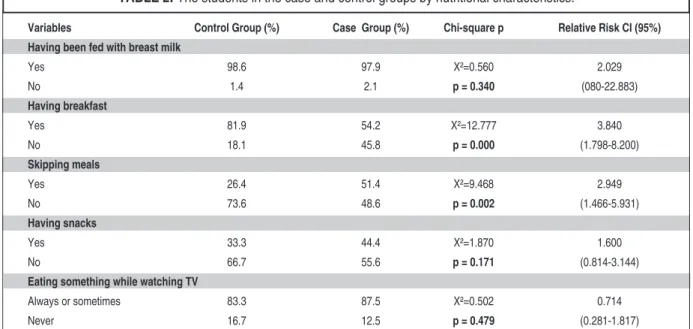
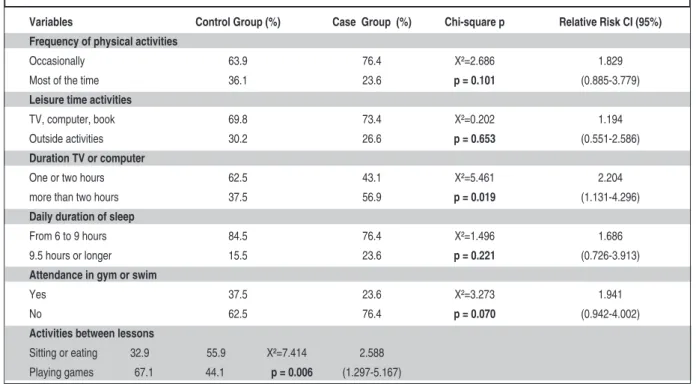
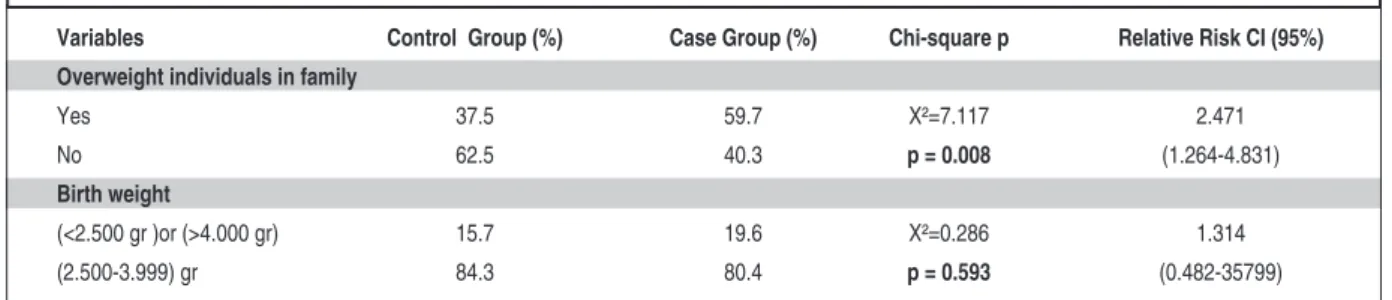
Determining the risk factors related with obesity and overweight in junior high school students: a case-control study
Tam metin
Şekil

Benzer Belgeler
We generate the random potential using an optical speckle pattern, whose induced forces act strongly on one species of particles (strong particles) and weakly on the other
Eğer etken viral ise hastalarda ek olarak üst solunum yolu enfeksiyonunun diğer bulguları olan; nazal konjesyon, burun akıntısı, ses kısıklığı, orbital
Sonuç olarak bu boyutta daha çok yenilenen öğretim programlarının ön plana çıktığı ve programlarla ilgili olarak okul müdürlerinin ve öğretmenlerin gerekli bilgi
Bu bölümde yönetim ve okul yönetiminin tanımı, okul yöneticilerinin sahip olması gereken özellikler ve yeterlikler, okul yöneticilerinin görev ve sorumlulukları,
caret ve Nafıa Nazırı Zihni Pa şaya tevdi olunmuştu. Paşa, ay nanın yanındaki sandalyeye o- turup II. Abdülhamide arzolu- nacak Vükelâ -Heyeti kararını
[r]
Hassas bir ka dın olan şairin yazılarında daima bir hüzün sezilmesi, bu aile saa- detsizliğinin izi olacaktır Nişâr Hanım 14 yaşlarında iken şiir
