The article states that 32.25% of the studied patients were in stage IIb and 67.75% patients in stage III. Computed tomography (CT) scan (thoracic region) and ultrasonography of the abdomen were done for determining the stage of disease. CT is not considered a reliable modality for the staging of esophageal carcinoma.[2] Even PET CT and
high‑resolution magnetic resonance imaging (MRI) have not been regarded as accurate for this purpose. Endoscopic ultrasonography (EUS) has been regarded the best modality, but even this cannot replace the accuracy of histopathologic staging in excluding higher stage disease. We would like to emphasize the importance of nodal status in this case. The number of involved lymph nodes has been proven to impact the prognosis.[3] The recent AJCC staging has also taken this
into account classifying nodal status on the basis of number of involved lymph nodes. CT has been a good investigation for evaluation of nodal metastasis. Periesophageal, mediastinal, and abdominal lymph nodes with short axis greater than 1 cm have widely been considered to be involved.[4] Here it would
be pertinent to raise the point that when CT alone has been used for staging in esophageal carcinoma, the nodal status would better correlate with prognosis rather than the overall stage on CT.
In addition, the role of endoscopic ultrasound (EUS) also needs to be emphasized. It visualizes all the layers of esophagus and gives good results in knowing not only the local tumor (T) stage but also the nodal (N) status of disease. The accuracy for T stage by EUS is 85% and N stage being 75%.[5] The use of
this investigation needs to be encouraged so that exact stage of malignant esophageal disease is recorded.
Definitive chemoradiation has the inherent drawback of lacking histopathological staging details provided by surgical treatment. Coupled with the selection bias, the inaccuracies in clinical staging tend to favor the surgical series whenever treatment results of chemoradiotherapy and surgery in carcinoma esophagus are compared. Thus, all efforts to minimize these flaws are needed in published studies so that the correct picture can be ascertained.
Mukesh Sharma, Anjna Sharma1 Departments of Radiotherapy and 1Radiodiagnosis, Indira Gandhi Medical
College, Shimla, Himachal Pradesh, India
For correspondence:
Dr. Mukesh Sharma, Department of Radiotherapy, Indira Gandhi Medical College, Shimla, Himachal Pradesh ‑ 171 001, India. E‑mail: [email protected] REFERENCES
1. Bhandari V. Role of concurrent chemoradiation in inoperable carcinoma esophagus: A prospective study. J Cancer Res Ther 2014;10:11‑4. 2. Quint LE, Glazer GM, Orringer MB. Esophageal imaging by MR and CT:
Study of normal anatomy and neoplasms. Radiology 1985;156:727‑31. 3. Rizk N, Venkatraman E, Park B, Flores R, Bains MS, Rusch V. American
Joint Committee on Cancer staging system. The prognostic importance of the number of involved lymph nodes in esophageal cancer: Implications for revisions of the American Joint Committee on Cancer staging system. J Thorac Cardiovasc Surg 2006;132:1374‑81. 4. Wolfman NT, Scharling ES, Chen MY. Esophageal squamous
carcinoma. Radiol Clin North Am 1994;32:1183‑201.
5. Rosch T. Endosonographic staging of esophageal cancer: A review of literature results. Gastrointest Endosc Clin N Am 1995;5:537‑47.
Re: Lambda light chain myeloma presenting as
nodular hepatic lesion: A clinical rarity
Access this article online
Website: www.cancerjournal.net Quick Response Code:
DOI: 10.4103/0973-1482.144555
PMID: ***
Sir,
I read an interesting article by Pal S et al.,[1] entitled “Lambda
light chain myeloma presenting as nodular hepatic lesion: A clinical rarity” in your Journal published on 2014 Jan‑Mar; 10 (1) 191‑3. The patient in this report had a successful outcome. Nevertheless, we want to share supportive information about
this rare disease. We treated a patient with a multiple liver extramedullary plasmositomas.
A 64‑year‑old female was incidentally found to have a multiple masses in the liver. She has slightly right upper quadrant pain. Her routine physical examination was unremarkable. Her blood count and routine biochemical parameters were within normal limits.
Abdominal ultrasonography (US) showed a hepatic mass on segment 8. This lesion displayed an isoechoic pattern with a surrounding hypoechoic halo [Figure 1]. Computed tomography (CT) and magnetic resonance imaging (MRI) showed multiple masses on the right liver lobe. Pre‑contrast CT showed multiple nodular hypodense lesions on the right
1335 Journal of Cancer Research and Therapeutics - October-December 2015 - Volume 11 - Issue 4
Letters to the Editor
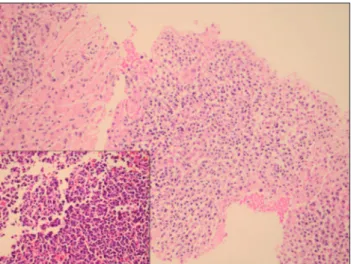
liver lobe. Post‑contrast CT scans (portal phase) revealed hypovascular and hypodense lesions compared with normal liver parenchyma [Figure 2]. Similarly, MRI showed multiple right liver lobe lesions. These masses showed low signal intensity on T1‑weighted imaging and high signal intensity on T2‑weighted imaging [Figure 3a and b]. The initial impression of the contrast‑enhanced CT suggested the possibility of hypovascular hepatic metastases. Hematological indexes, liver function tests, and renal function tests were within the normal limits. A needle biopsy of the largest liver mass was performed. Histological examination of the liver biopsy showed diffuse solid proliferation of monotonous small round cells. These cells had eccentric cytoplasm and round nuclei with peripheral condensed chromatin. The diagnosis after immunohistochemical staining was plasmacytoma of the kappa type. Leukocyte common antigen, cytokeratin, CD34, S100, synaptophysin, and desmin staining was negative [Figure 4]. Extramedullary plasmacytomas (EMPs) are uncommon, and most are found in the lungs, oronasopharynx, or paranasal
Figure 1: Abdominal ultrasonography showed a hepatic mass
on segment 8. This lesion displayed an isoechoic pattern with a surrounding hypoechoic halo (arrows)
Figure 2: Post-contrast computed tomography at the level of the portal
hilus scan (portal phase) demonstrated multiple hypovascular and hypodense lesions compared with normal liver parenchyma (arrows)
Figure 4: Photomicrograph showing atypical infiltrating plasma cells and
effacing normal liver tissue [main frame: (H and E) staining, ×100; inset frame: H and E ×400]
Figures 3: (a and b). Axial magnetic resonance imaging showed
multiple right liver lobe lesions. These masses showed low signal intensity on T1-weighted imaging (a) and high signal intensity on T2-weighted imaging (b)
b a
sinuses.[2,3] These lesions represent a rare form of plasma
cell proliferation in which the tumor arises outside the bone marrow. The diagnosis of EMP requires the absence of bone marrow plasmacytosis, a normal skeletal survey, and plasma cell infiltration only at the site of EMP.[4]
Hepatic plasmacytomas are rare, and images of these lesions on US, CT, and MRI are variable, providing insufficient knowledge. US may be the first choice, but it must be supported by other radiological modalities because it is unable to detect all lesions.
Generally, including in our case, these lesions are defined as having a hypovascular pattern. Matheiu et al.,[4] described
a case where the dynamic CT finding of peripheral enhancement with gradual filling‑in toward the center of the lesion is very similar to those encountered in
1336 Journal of Cancer Research and Therapeutics - October-December 2015 - Volume 11 - Issue 4
Letters to the Editor
For correspondence:
Dr. Serife Ulusan, Department of Radiology, Faculty of Medicine, Baskent University, Yuregir, Adana 01250, Turkey. E‑mail: [email protected] REFERENC ES
1. Pal S, Chattopadhyay B, Chatterjee A, Bhattacharya B. Lambda light chain myeloma presenting as nodular hepatic lesion: A clinical rarity. J Cancer Res Ther 2014;10:191‑3.
2. Oshima K, Kanda Y, Nannya Y, Kaneko M, Hamaki T, Suguro M, et al. Clinical and pathologic findings in 52 consecutively autopsied cases with multiple myeloma. Am J Hematol 2001;67:1‑5
3. Kapadia SB. Multiple myeloma: A clinicopathologic study of 62 consecutively autopsied cases. Medicine (Baltimore) 1980;59:380‑92. 4. Mathieu D, Elouaer‑Blanc L, Diviné M, René E, Vasile N. Hepatic
plasmacytomas: Sonographic and CT findings. J Comput Assist Tomogr 1986;10:144‑5.
5. Monill J, Pernas J, Montserrat E, Pérez C, Clavero J, Martinez‑Noguera A, et al. CT features of abdominal plasma cell neoplasms. Eur Radiol 2005;15:1705‑12.
cavernous hemangiomas. However, in all cases of hepatic plasmacytomas described, including ours, the lesions were more conspicuous on US, which was also the preferred method of biopsy in most cases.
The MRI images of hepatic plasmacytomas are also variable and limited. In the English‑language literature, these lesions are described as showing low signal intensity on T1‑weighted imaging and high signal intensity on T2‑weighted imaging.[5]
It is important to differentiate plasmacytomas from other hepatic metastases by biopsy because they may be resectable, are radiosensitive, and show a better prognosis.
Serife Ulusan, Nazım Emrah Koçer1 Departments of Radiology and 1Pathology, Faculty of Medicine,
Baskent University, Yuregir, Adana, Turkey
Primary neuroendocrine mediastinal tumor presenting
with carcinoid syndrome and left supraclavicular
lymphadenopathy. Clinico-radiological and
pathological features
Access this article online
Website: www.cancerjournal.net Quick Response Code:
DOI: 10.4103/0973-1482.140775
PMID: ***
Sir,
With respect to the letter to editor, I would like to submit that the manuscript is dedicated to the clinicoradiological features of neuroendocrine tumors. The authors wanted to stress the point that the tumor presented with supraclavicular adenopathy and carcinoid syndrome. The imaging findings showed a normal scan of abdomen. The diagnosis of an atypical low‑grade neuroendocrine tumor was reported arising from the mediastinum. The controversy regarding the nomenclature and origin of neuroendocrine tumors has been mentioned in the beginning of the discussion.
Moreover, the suggestion to include a pathologist as an author depends upon the contribution to the manuscript. The mere confirmation of pathology by tissue diagnosis does not merit authorship by any standard international guidelines.
The manuscript was an assiduous clinical and radiological work up to arrive at a correct diagnosis in a young patient who presented with left supraclavicular adenopathy and carcinoid syndrome. Tissue diagnosis was routine and necessary, which is usual in any case study or report. The contribution of a pathologist was minimal and did not warrant authorship.
Amit Nandan D. Dwivedi, Kanika Goel, Suchi Tripathi1, Sunny Garg1, Madhukar Rai1 Departments of Radiodiagnosis and Imaging, and 1Internal Medicine,
Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India
For correspondence:
Dr. Amit Nandan D. Dwivedi, Department of Radiodiagnosis and Imaging, Institute of Medical Sciences, Banaras Hindu University, Varanasi ‑ 221 005, Uttar Pradesh, India. E‑mail: [email protected]
1337 Journal of Cancer Research and Therapeutics - October-December 2015 - Volume 11 - Issue 4
Letters to the Editor