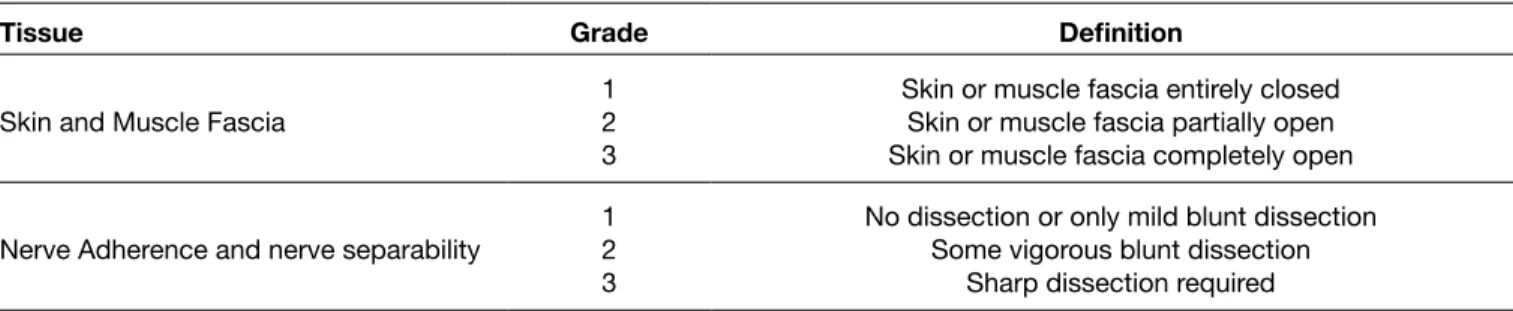
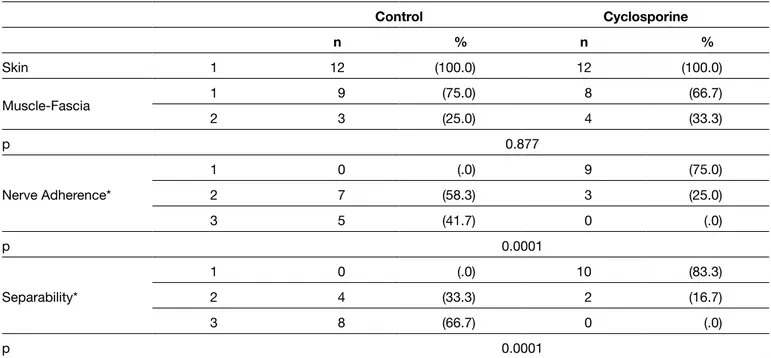
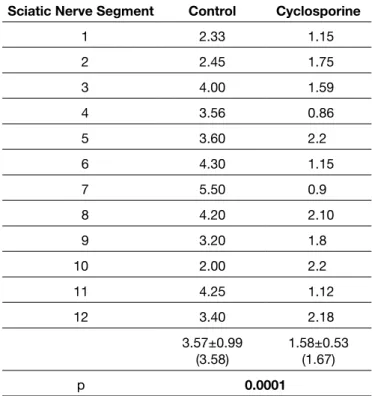
Topical application of cyclosporine reduces epineurial fibrosis: Gross post-surgical, histopathological and ultrastructural analysis in a rat sciatic nerve model
Tam metin
Şekil
Benzer Belgeler
The behavior of the critical capital stock with respect to these parameters is important in explaining the persistent differences in per capita capital stocks among countries
Therefore Theorem 1 makes Grodal’s results on closedness of the set of Pareto optimal allocations, and the core, and continuity of the core of pure exchange economies (Grodal,
Turkish FP in the new era, according to a hawkish realist and anti-government camp that includes Hu¨rriyet, Cumhuriyet, Yenic¸ag˘ and Milliyet newspapers, is: ima- ginative
The main extrinsic invariant is the squared mean curvature and the main intrinsic invariants include the classical curvature invariants namely the scalar curvature and the
Tepeardı Mevkii’nde yaklaşık 48 parça değerlendirmeye alındı.Neolitik ve Kalkolitik dönem seramikleri çanaklar, “S” profilli çömlekler, düz ve hafif içe dönük
Bu nedenle de tek bir dinin, ideolojinin, sınıfın hâkim olduğu veya tek bir devletin diğerlerini egemenliği altına aldığı Roma İmparatorluğu, Orta Çağ Kilisesi,
Türk düşünürleri ve sosyologları yaygın olan kültür ve medeniyet tanımlarını kullanmışlar, genel olarak kültür tartışmalarındaki kültürün maddi
