Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction Treatment?
Tam metin
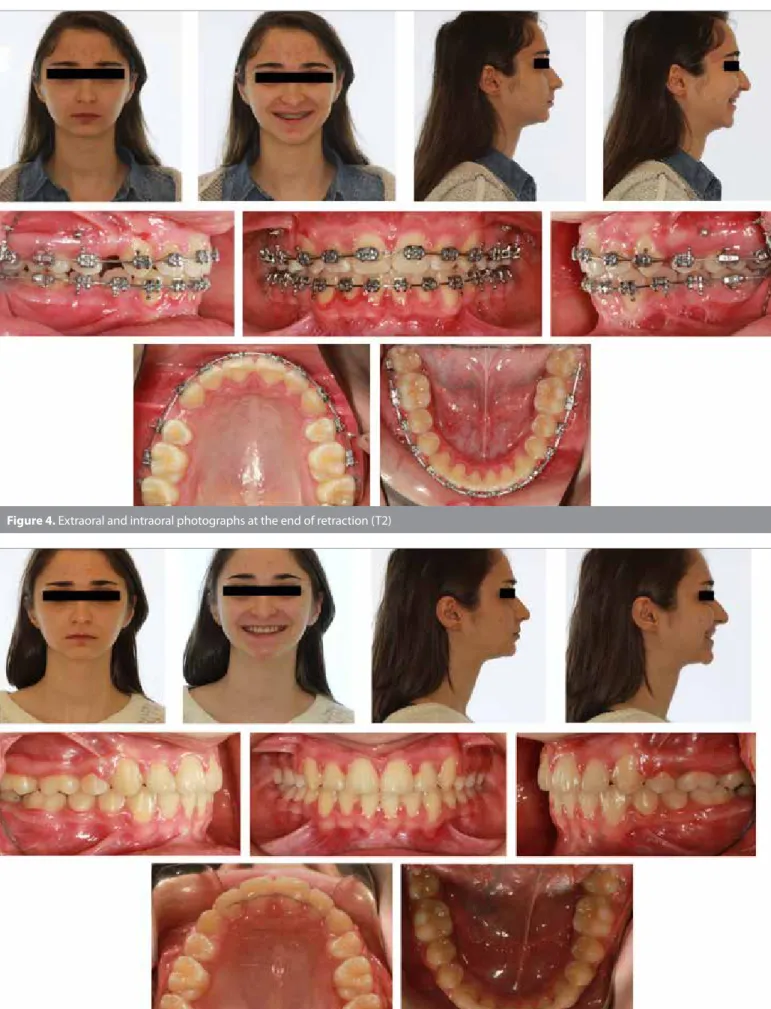
Şekil


Benzer Belgeler
25 geleneksel multiloop edgewise me- kaniği ile mini vida destekli multiloop edgewise mekaniğini kıyasladıkları çalışmalarında, Sınıf III elastikleri birinci grupta üst
Mannchen (32), üst molar distalizasyonu için pala- tal implantları ankraj olarak kullanarak Sınıf II dişsel ilişkiyi düzelttiği iki vakasını sunmuştur.. Çalışmada
Therefore, the GALATA (GALvus safety and efficacy Assessment in Turkish populAtion) study, a 6 month prospective, single-arm cohort study in patients with T2DM, was the
This study was conducted on white collar workers working in private and public organizations and it was determined that there are positive and significant relationships
Proposal of new expanded selection criteria using total tumor size and (18)F-fluorodeoxyglucose - positron emission tomography/computed tomography for living donor
The main reason for failure in inlays luted with dual-polymerized composite or con- ventional glass ionomers were partial fracture or total loss of the inlays.[ 25 ] In one study,
İçbükey kemerlerden oluşan bir tepelikle sonlanan 153x40-44x12 cm ölçülerindeki baş taşının sülüs 10 satırlık metin bölümü, zemin oyma tekniğinde hazırlanmış
Contractions in the setting of soft compact metric spaces which generalizes the results of Sayyed
