Introduction
Acute coronary syndrome is correlated with high morbidity and mortality rates [1]. Guidelines recommend clinical risk score calcu-lations for the planning of treatment [2, 3]. Aortic stiffness is related to mechanical aortic wall tension and elasticity [4]. Increased arteri-al stiffness by impairing especiarteri-ally large arteriarteri-al dilatation capacity, decreases cardiac perfor-mance and adversely affects organ perfusion [5]. Increased pulse pressure due to large arte-rial stiffness also affects the coronary out-comes by increasing systolic blood pressure and after load [6]. Aortic stiffness can be evalu-ated by simple and noninvasive methods. Aortic
strain is one of the aortic elasticity indexes. Aortic stiffness index represents aortic stiff-ness [7, 8]. In order to determine the treatment and follow up strategies of the patients with acute coronary syndromes, clinical risk scoring systems were generated according to the results of comprehensive clinical studies [9]. Global Registry of Acute Coronary Events (GRACE) risk score is one of the most important scoring system and it is found to be related to prognosis [9].
GRACE risk score includes laboratory parame-ters such as ECG changes, increase in cardiac markers and creatine value in addition to clini-cal characteristics of the patients such as age,
Original Article
Relation of the aortic stiffness with the GRACE risk
score in patients with the non ST-segment
elevation myocardial infarction
Gedikli Omer1, Aksan Gokhan2, Uzun Adem1, Demircan Sabri3, Soylu Korhan4
1Departmant of Cardiology, Artvin State Hospital, Artvin, Turkey; 2Departmant of Cardiology, Gazi State Hospital,
Samsun, Turkey; 3Department of Cardiology, Faculty of Medicine, İstanbul Bilim University, İstanbul, Turkey; 4Department of Cardiology, Faculty of Medicine, Ondokuz Mayis University, Samsun, Turkey
Received July 8, 2014; Accepted August 16, 2014; Epub September 15, 2014; Published September 30, 2014 Abstract: Background: Current guidelines recommend clinical risk scoring systems for the patients diagnosed and determinated treatment strategy with in Non-ST-elevation elevation myocardial infarction (NSTEMI). Previous stud-ies demonstrated association between aortic elasticity propertstud-ies, stiffness and severity CAD. However, the as-sociations between Aortic stiffness, elasticity properties and clinical risk scores have not been investigated. In the present study we have evaluated the relation between the Global Registry of Acute Coronary Events (GRACE) risk score and aortic stiffness in patients with NSTEMI. Method: We prospectively analyzed 87 consecutive patients with NSTEMI. Aortic elastic parameter and stiffness parameter were calculated from the echocardiographically derived thoracic aortic diameters (mm/m2), and the measurement of pulse pressure obtained by cuff sphygmomanometry.
We have categorized the patients in to two groups as low ((n = 45) (GRACE risk score ≤ 140)) and high ((n = 42) (GRACE risk score > 140)) risk group according to GRACE risk score and compare the both groups. Results: Table 1 shows baseline characteristics of patients. Our study showed that Aortic strain was significantly low (3.5 ± 1.4, 7.9 ± 2.3 respectively, p < 0.001) and aortic stiffness index was significantly high (3.9 ± 0.38; 3 ± 0.35, respectively, p < 0.001) in the high risk group values compared to those with low risk group. The aortic stiffness index was the only independent predictor of GRACE risk score (OR: 119.390; 95% CI: 2.925-4872.8; p = 0.011) in multivariate analysis. Conclusion: We found a significant correlation between aortic stiffness, impaired elasticity and GRACE risk score. Aortic stiffness index was the only independent variable of the high GRACE risk score. The inclusion of aortic stiffness into the GRACE risk score could allow improved risk classification of patients with ACS at admission and this may be important in the diagnosis, follow up and treatment of the patients.
heart rate, systolic blood pressure, and degree of heart failure [9]. Echocardiography is used in all of the fields of cardiology; however there is no echocardiography parameter in these clini-cal scoring systems. Previous studies have demonstrated the relation between arterial stiffness and stroke [10], heart failure [11] and coronary artery disease [12]. Relation between the presence and the extention of coronary artery disease and aortic elastic properties were investigated in previous studies [12, 13]. However there is no study in the literature searching the relation between the aortic elas-tic parameters and stiffness measured by echocardiography parameters and clinical risk scores in acute coronary syndromes.
In the present study we have evaluated the relation between the GRACE risk score and Aortic stiffness measured by echocardiography in patients who were admitted to our hospital with the diagnosis of non ST elevation myocar-dial infarction (NSTEMI).
Materials and methods Study population
Study population consisted of 107 patients who were referred to Ondokuz Mayıs University emergency department with chest pain and had the diagnosis of non ST elevation acute coronary syndrome (NSTEMI) according to the results clinical, electrocardiographic and labo-ratory evaluation and admitted to coronary care unit between March 2012 and December 2012. Among 107 patients, 7 had no athero-sclerosis on coronary angiography, 6 declined to have coronary angiography and 7 had poor quality of echocardiography images and subse-quently excluded from study. Echocardiographic examinations were performed and parameters were recorded at the time of the diagnosis of acute coronary syndrome and after the recov-ery of acute ischemia, ECG and clinical complaints.
Transthoracic echocardiography was per-formed within 24 hours and coronary angiogra-phy was performed within 3-1.5 days. Evaluation of clinical risk in patients with NSTEMI was done according to GRACE risk score.
Exclusion criteria were severe ventricular arrhythmia, myocarditis, pericarditis,
pulmo-nary emboli, severe heart failure or cardiogenic shock, presence of prosthetic valve, acute or chronic renal failure, musculoskeletal disease, presence of malignity, previous history of PCI or CABS, patients under regular medical treat-ment, severe hypertension, apparent DM, severe aortic valve disease, and dilatation of ascendant aorta. In addition patients who had cardioversion or exposed to trauma and patients who were followed medically and not undergone coronary angiography were also excluded from study.
Diagnosis of acute NSTE-ACS
NSTE-ACS was considered as presence of T-wave inversion or ST-segment depression and/or positive Troponin I in the absence of electrocardiographic (ECG) ST elevation in patients presenting with angina or equivalent [2].
Calculation of GRACE risk score
The main principle of the GRACE risk score has been described elsewhere [14]. The variables required for calculation of the score include age, heart rate, systolic blood pressure, base-line creatine level, history of congestive heart failure, in hospital percutaneous coronary inter-vention, history of MI, ST segment depression on admission electrocardiography (ECG) and elevated cardiac enzyme or marker levels. This study, we used single serum levels in this study, we used single serum levels of cTnI 0.1 ng/ml as the elevated cardiac marker. ST-segment depression was defined as decreased ST seg-ment: 0.5 mV below the isoelectric line in any ECG lead. As is known patients who had GRACE risk score 140 over have bad clinical progres-sion and poor prognosis that is why early inva-sive treatment strategies are recommended for these patients. For this reason we have catego-rized the patients in to two groups as low ((n = 45) (GRACE risk score ≤ 140)) and high ((n = 42) (GRACE risk score > 140)) risk group according to GRACE risk score and compare the both groups.
Measurements of aortic elasticity and stiff-ness parameters
In the present study, we used echocardiograph-ically derived method for the evaluation of aor-tic elasaor-tic properties and stiffness. This
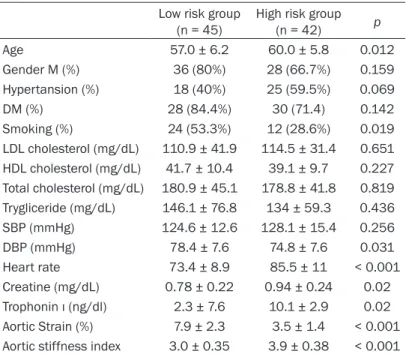
meth-Table 1. The demographic, laboratory characteristics, aortic strain and aortic stiffness index values of patients
Low risk group
(n = 45) High risk group (n = 42) p Age 57.0 ± 6.2 60.0 ± 5.8 0.012 Gender M (%) 36 (80%) 28 (66.7%) 0.159 Hypertansion (%) 18 (40%) 25 (59.5%) 0.069 DM (%) 28 (84.4%) 30 (71.4) 0.142 Smoking (%) 24 (53.3%) 12 (28.6%) 0.019 LDL cholesterol (mg/dL) 110.9 ± 41.9 114.5 ± 31.4 0.651 HDL cholesterol (mg/dL) 41.7 ± 10.4 39.1 ± 9.7 0.227 Total cholesterol (mg/dL) 180.9 ± 45.1 178.8 ± 41.8 0.819 Trygliceride (mg/dL) 146.1 ± 76.8 134 ± 59.3 0.436 SBP (mmHg) 124.6 ± 12.6 128.1 ± 15.4 0.256 DBP (mmHg) 78.4 ± 7.6 74.8 ± 7.6 0.031 Heart rate 73.4 ± 8.9 85.5 ± 11 < 0.001 Creatine (mg/dL) 0.78 ± 0.22 0.94 ± 0.24 0.02 Trophonin ı (ng/dl) 2.3 ± 7.6 10.1 ± 2.9 0.02 Aortic Strain (%) 7.9 ± 2.3 3.5 ± 1.4 < 0.001 Aortic stiffness index 3.0 ± 0.35 3.9 ± 0.38 < 0.001
LDL, Low-density lipoprotein; HDL, High-density lipoprotein; DBP, Diastolic blood pressure; SBP, sistolic blood pressure.
od is readily available, relatively less expensive, and noninvasive compared with other tech-niques. The echocardiographic examinations were obtained by using GE VingMed vivid 7 pro (Horten, Norway). Thoracic aortic diameters (mm/m2) were measured 3 cm above the aortic
valve by two-dimensional guided M-mode transthoracic echocardiography of the aortic root at left parasternal long-axis view. Aortic systolic diameter (AoS) was measured at the time of full opening of the aortic valve, and dia-stolic diameter (AoD) at the peak of the QRS complex at the simultaneous electrocardio-gram recording. After echocardiographic exami-nation, blood pressure was measured from right arm with a standard sphygmomanometer. The first sound of Korotkoff was accepted as systolic, and the fifth sound was accepted as diastolic blood pressure. Pulse pressure (PP) was calculated as systolic minus diastolic blood pressure. The elasticity of the aorta was assessed by the following parameters [15, 16]. Aortic strain (%) = (AoS - AoD) × 100/AoD Aortic stiffness index = ln (systolic pressure/ diastolic pressure)/[(AoS − AoD)/AoD]
Stiffness index is a marker for aortic stiffness, whilst strain is marker for aortic elasticity.
variables were analyzed by Chi-square test and Fischer-exact test. Multivariable logistic regres-sion analysis was used to assess the relation-ship between increased GRACE score and other variables. A p value < 0.05 was considered sta-tistically significant. SPSS 15.0 statistical pro-gram (SPSS Inc, Chicago, IL USA) was used to statistical analysis.
Results
The study population consisted of 87 patients with NSTEMİ. There were 64 (74%) men and 23 (26%) women in the study population. Mean age of patients were 58.4±4. In all, 58 (66.6%) patients were diabetic, 43 (49%) patients were hypertensive and 36 (41.3%) patients were smokers. According to the GRACE risk score, 42 (48.2%) patients were in the high risk score group and 45 (51.8%) patients were in the low risk score group. The demographic, laboratory characteristics, the aortic elasticity properties and aortic stiffness of patients in GRACE risk score groups are presented in Table 1. High risk group was older (60.0 ± 5.8, 57.0 ± 6.2, respectively, p = 0.012) heart rate (85.5 ± 11, 73.4 ± 8.9, respectively, p < 0.001) creatine (0.94 ± 0.24, 0.78 ± 0.22, respectively, p = 0.02), and trophonin ı (ng/dl) (10.1 ± 2.92, 3.0
We have used the aortic strain as aortic elasticity parameter. Impai-red aortic elasticity properties are association with aortic stiff-ness [15, 16].
These parameters give informa-tion on structure of aorta [17]. Abnormality in these parameters means structural alteration of arterial wall [17]. Elastic proper-ties of aorta are useful not only in representing basic mechanical behavior of the arterial system but also in predicting outcome [17].
Statistical analyses
All continuous variables were given as mean ± standard devia-tion. Normal distribution was assessed by Kolmogorov–Smir- nov test. Then, student t-test and Mann Whitney U-test were used when appropriate. Categorical
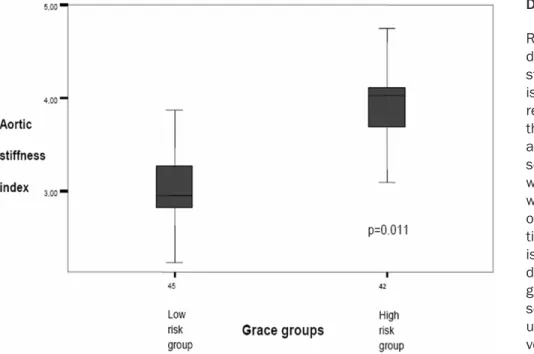
Figure 1. Aortic stiffness index in the study groups.
± 7.6, respectively, p = 0.02) level was higher, Diastolic blood pressure (74.8 ± 7.6, 78.4 ± 7.6, respectively, p = 0.031) and smoking (12 (28.6%), 24 (53.3%), respectively, p = 0.019) was lower than low risk group. Aortic strain (3.5 ± 1.47, 9.0 ± 2.3, respectively, p < 0.001) and aortic stiffness index (3.9 ± 0.38, 3.0 ± 0.35, respectively, p < 0.001) showed a significant difference between two groups. The aortic stiff-ness index showed a proportional increase cor-related with GRACE risk score (Figure 1). Univariate and multivariate relationships of GRACE risk score
GRACE risk score was associatedwith age (OR: 1.1000, p = 016), smoking (OR: 0.350, p =
0.021), lower diastolic blood pressure (OR: 0.937, p = 0.036) higher aortic stiffness index (OR: 230.460, p < 0.001) and lower Aortic strain (OR: 0.493, p < 0.001) on Univariate logistic regression analysis (Table 2). Multivariate analysis was performed in order to evaluate the independent determinants of GRACE risk score (Table 2). The aortic stiffness index was the only independent predictor of GRACE risk score (OR: 119.390; 95% CI: 2.925-4872.8; p = 0.011) in multivariate analysis (Table 2).
coronary artery disease and also the cardiovas-cular events [4, 12, 18]. There are several stud-ies that have demonstrated the increased car-diovascular morbidity and mortality with the increased in arterial stiffness [19, 20]. Willum-Hansen et al. have investigated the arterial stiffness in general population and put forth the relation between the aortic stiffness and cardiovascular events and mortality [21]. Study of Akinori et al. has demonstrated that there is a marked increase in CAVI (cardio-ankle vascu-lar index) in patients with acute coronary syn-drome [22]. However there is no study evaluat-ing the relation between the Grace risk score which is used in the routine clinical practice for the diagnosis and treatment of the patients with acute coronary syndrome and aortic elas-ticity parameters (aortic strain) and aortic stiff-ness index which can easily be measured with echocardiographic examination. GRACE scoring system is an important scoring system which is composed of specific parameters and advised by the current guidelines for the diagnosis and the determination of treatment strategies in patients with acute coronary syndrome [2]. Among the GRACE risk scoring parameters, there is no echocardiographic parameter. Previous studies have demonstrated the rela-tion between GRACE risk score and cardiovas-cular events and prognosis in patients with ACS
Discussion
Results of our stu- dy have demon-strated that there is a significant relation between the aortic stiffness and clinical risk score in patients with NSTEMI and we have also dem-onstrated that aor-tic stiffness index is the independent determinant of hi- gh GRACE risk score. Previous st- udies have re- vealed that there is a relation bet- ween aortic stiff-ness and extend and the severity of
Table 2. Relationship between increased GRACE score and other variables
Univariate analysis Multivariate analysis
OR P OR P 95% CI Lower Upper Age 1.100 0.016 1.064 0.439 0.910 1.243 DBP 0.937 0.036 0.924 0.192 0.821 1.040 HT 2.206 0.071 0.551 0.494 0.100 3.038 Smoking 0.350 0.021 3.822 0.109 0.743 19.657 Aortic Strain 0.493 < 0.001 0.930 0.832 0.462 1.870 Aortic Stiffness index 230.460 < 0.001 119.390 0.011 2.925 4872.801
DBP, Diastolic blood pressure; HT, Hypertension.
[23]. For this reason there may be a relation between the GRACE risk score and aortic stiffness.
Aortic stiffness has an adverse effect on arte-rial wall integrity, coronary perfusion and left ventricular function in patients with cardiovas-cular disease. Arterial stiffness is related to large arterial mechanical tension [4, 24]. As a result, increased arterial stiffness or decreased elasticity increase the left ventricular burden and myocardial oxygen demand and impair left ventricular function and coronary blood flow [22, 24, 25]. Besides, it was reported that, in patients with moderate coronary artery dis-ease, large arterial stiffness is the major deter-minant of exercise myocardial ischemia [26]. Fukuda et al. have searched the relation between Ao-bracial PWV index which is related to aortic stiffness. FFR and found that coronary flow is decreased in patients with aortic stiffen-ing [5]. Deterioration in aortic elasticity and stiffness parameters may increase the myocar-dial ischemia by decreasing coronary blood flow and increasing myocardial oxygen demand in addition to atherosclerotic lesions.
As a result, poor clinical condition results in high Grace score. In addition to this, previous studies have revealed the relation between the deterioration in aortic elasticity and stiffness parameters and complicated atherothrombotic lesion [27]. Selwaness et al have demonstrat-ed the relation between arterial stiffness and carotid plaque hemorrhage and vulnerability [28]. There may be a correlation between ves-sels that have impaired elasticity, increased stiffness and unstable atherosclerotic plaques and extent of ischemia, high risk scores and bad prognosis. In our study, there was a strong correlation between aortic stiffness and
clini-and stiffness clini-and GRACE risk score. Aortic stiff-ness index was the only independent variable of the high GRACE risk score. Based on our knowledge, this is the first study to correlate aortic stiffness with GRACE risk score.
Limitations of study
Major limitation of our study is the low number of the patients. Besides, aortic elasticity and stiffness calculations done with the echocar-diography by measuring the diameter changes in ascendant aorta is not a gold standard [17]. However it gives information about local stiff-ness and can be done with echocardiography machine which can easily be reached even in intensive care units and it is practical and cheap. In addition we have planned our study to find a method which can be used in routine clinical practice. As is known that social securi-ty systems in many countries do not pay the price of the gold standard systems that mea-sures the aortic stiffness, however echocar-diography is practical and easily reachable. In conclusion, the determination of aortic stiff-ness may be useful parameter for risk stratifi-cation of patients with NSTEMI during the hos-pitalization period. The inclusion of aortic stiff-ness parameters into the GRACE risk score could allow improved risk classification of patients with ACS at admission and this may be important in the diagnosis, follow up and treat-ment of the patients. Large, prospective, multi-center registries are necessary to confirm our results.
Disclosure of conflict of interest None.
cal risk score. There was a significant corre-lation between the aortic strain and stiff-ness index and GRACE risk score at Univariate logistic regression an- alysis, however aortic stiffness was the only independent variable in multivariate analy-sis. We found a signifi-cant correlation be- tween aortic elasticity
Address correspondence to: Dr. Gedikli Omer, Departmant of Cardiology, Artvin State Hospital, Artvin 08000, Turkey. Tel: + 90 466 212 10 40; Fax: + 90 0466 212 34 23; E-mail: drgedikli@hotmail. com
References
[1] Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet 1997; 349: 1269-1276. [2] Hamm CW, Bassand JP, Agewall S, Bax J,
Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, Uva MS, Storey RF, Wijns W, Zahger D; ESC Committee for Practice Guidelines. ESC Guide-lines for the management of acute coronary syndromes in patients presenting without per-sistent ST-segment elevation: The Task Force for the management of acute coronary syn-dromes (ACS) in patients presenting without persistent ST-segment elevation of the Euro-pean Society of Cardiology (ESC). Eur Heart J 2011 Dec; 32: 2999-3054.
[3] Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000; 36: 959-69. [4] Hope SA, Antonis P, Adam D, Cameron JD, Mer-edith IT. Arterial pulse wave velocity but not augmentation index is associated with coro-nary artery disease extent and severity: impli-cations for arterial transfer function applicabil-ity. J Hypertens 2007; 25: 2105-2109. [5] Fukuda D, Yoshiyama M, Shimada K,
Yamashi-ta H, Ehara S, Nakamura Y, Kamimori K, Tana-ka A, Kawarabayashi T, YoshiTana-kawa J. Relation between aortic stiffness and coronary flow re-serve in patients with coronary artery disease. Heart 2006; 92: 759-62.
[6] Mitchell GF, DeStefano AL, Larson MG, Benja-min EJ, Chen MH, Vasan RS, Vita JA, Levy D. Heritability and a genomewide linkage scan for arterial stiffness, wave reflection, and mean arterial pressure: the Framingham Heart Study. Ciculation 2005; 112: 194-199.
[7] Eren M, Gorgulu Ş, Uslu N, Celik S, Dağdeviren B, Tezel T. Relation between aortic stiffness and left ventricular diastolic function in pa-tients with hypertension,diabetes, or both. Heart 2004; 90: 37-43.
[8] Ikonomidis I, Lekakis J, Stamatelopoulos K. Aortic elastic properties and left ventricular di-astolic function in patients with Adamantiades-Behcet’s Disease. J Am Coll Cardiol 2004; 43: 1075-1081.
[9] de Araújo Gonçalves P, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE
risk scores: sustained prognostic value and in-teraction with revascularization in NSTE-ACS. Eur Heart J 2005; 26: 865-872.
[10] Biteker M, Ozden T, Dayan A, Tekkeşin AI, Mısırlı CH. Aortic stiffness and plasma brain natriuretic peptide predicts mortality in acute ischemic stroke. Int J Stroke 2013; [Epub ahead of print].
[11] Desai AS, Mitchell GF, Fang JC, Creager MA. Central aortic stiffness is increased in patients with heart failure and preserved ejection frac-tion. J Card Fail 2009; 15: 658-64.
[12] Yıldız A, Gur M, Yılmaz R, Demirbağ R. The as-sociation of elasticity indexes of ascending aorta and the presence and the severity of coronary artery disease. Coronary Artery Dis-ease 2008; 19: 311-317.
[13] Giannattasio C, Capra A, Facchetti R, Viscardi L, Bianchi F, Failla M, Colombo V, Grieco A, Mancia G. Relationship between arterial dis-tensibility and coronary atherosclerosis in an-gina patients. J Hypertens 2007; 25: 593-598. [14] Eagle KA, Lim MJ, Dabbous OH, Pieper KS,
Goldberg RJ, Van de Werf F, Goodman SG, Granger CB, Steg PG, Gore JM, Budaj A, Avezum A, Flather MD, Fox KA; GRACE Investigators. A validated prediction model for all forms of acute coronary syndrome: estimat-ing the risk of 6-month postdischarge death in an international registry. JAMA 2004; 291: 2727-2733.
[15] Lacombe F, Dart A, Dewar E, Jennings G, Cameron J, Laufer E. Arterial elastic properties in man: a comparison of echo-Doppler indices of aortic stiffness. Eur Heart J 1992; 13: 1040-1045.
[16] Stefanadis C, Stratos C, Boudoulas H, Kourouklis C, Toutouzas P. Distensibility of the ascending aorta: Comparison of invasive and non-invasive techniques in healthy men and in men with coronary artery disease. Eur Heart J 1990; 11: 990-996.
[17] Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H; European Network for Non-invasive Investigation of Large Arteries. Expert consen-sus document on arterial stiffness: method-ological issues and clinical applications. Eur Heart J 2006; 27: 2588-605.
[18] Gary F Mitchell, ShihJen Hwang, Ram- achandran S Vasan, Martin G Larson, Michael J Pencina, Naomi M Hamburg, Joseph A Vita, Daniel Levy and Emelia J Benjamin. Arterial stiffness and cardiovascular events: the Framingham Heart Study Circulation 2010 February 2; 121: 505-511.
[19] Van Sloten TT, Schram MT, van den Hurk K, Dekker JM, Nijpels G, Henry RM. Stehouwer
CD Local stiffness of the carotid and femoral artery is associated with incident cardiovascu-larevents and all-cause mortality: the hoorn study. J Am Coll Cardiol 2014; 63: 1739-47. [20] Papaioannou TG, Protogerou AD, Stergiopulos
N, Vardoulis O, Stefanadis C, Safar M, Blacher J. Total arterial compliance estimated by a nov-el method and all-cause mortality in the nov- elder-ly: the PROTEGER study. Age (Dordr) 2014; 36: 9661.
[21] Willum-Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H, Jeppesen J. Prognostic value ofaortic pulse wave velocity as index of arterial stiffness in the generalpop-ulation. Circulation 2006; 113: 664-7080. [22] Sairaku A, Eno S, Hondo T, Teragawa H, Nakano
Y, Matsuda K, Kisaka T, Kihara Y. Head-to-head comparison of the cardio-ankle vascular index between patients with acute coronary syn-drome and stable angina pectoris. Hypertens Res 2010; 33: 1162-6.
[23] de Araújo Gonçalves P, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and in-teraction with revascularization in NSTE-ACS. Eur Heart J 2005; 26: 865-872.
[24] Bogren HG, Mohiaddin RH, Klipstein RK, Firmin DN, Underwood RS, Rees SR, Longmore DB. The function of the aorta in ischemic heart disease: A magnetic resonance and angio-graphic study of aortic compliance and blood flow patterns. Am Heart J 1989; 118: 234-247.
[25] Ohtsuka S, Kakihana M, Watanabe H, Sugishita Y. Chronically decreased aortic dis-tensibility causes deterioration of coronary perfusion during increased left ventricular contraction. J Am Coll Cardiol 1994; 24: 1406-1414.
[26] Kingwell BA, Waddell TK, Medley TL, Cameron JD, Dart AM. Large artery stiffness predicts ischemic threshold in patients with coronary artery disease. J Am Coll Cardiol 2002; 40: 773-779.
[27] Taglieri N, Dall’Ara G, Rapezzi C, Saia F, Cinti L, Rosmini S, Alessi L, Vagnarelli F, Moretti C, Palmerini T, Marrozzini C, Montefiori M, Branzi A, Marzocchi A. Predictors of complicated athero-thrombotic lesions in non-ST segment acute coronary syndrome. J Cardiovasc Med (Hagerstown) 2013; 14: 430-7.
[28] Selwaness M, van den Bouwhuijsen Q, Mattace-Raso FU, Verwoert GC, Hofman A, Franco OH, Witteman JC, van der Lugt A, Vernooij MW, Wentzel JJ. Arterial stiffness is associated with carotid intraplaque hemor-rhage in the general population: the Rotterdam study. Arterioscler Thromb Vasc Biol 2014; 34: 927-32.