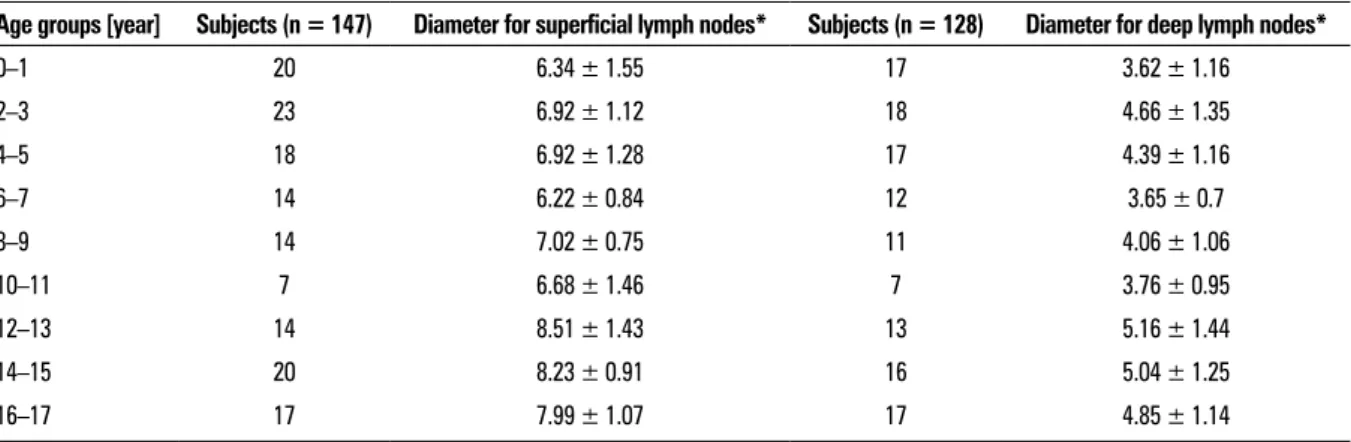
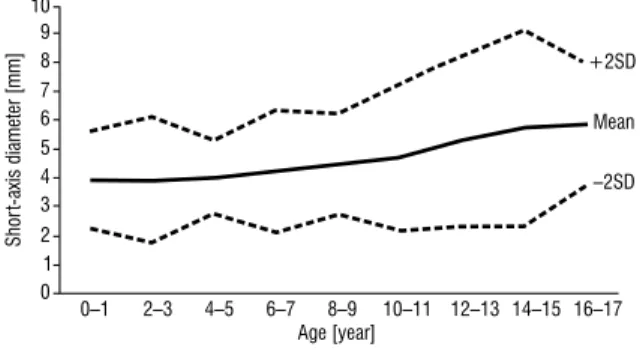
Computed tomography depiction of normal inguinal lymph nodes in children
Tam metin
Şekil
Benzer Belgeler
Among the first to do so was Sayyid ‘Ali Hariri’s Book of the Splendid Stories of the Crusades (Cairo: 1899), the first Arabic-language study of the Crusades, to Syed Qutb’s use
Zira 6545 sayılı Kanun ile yapılan değişiklikten önce, cinsel saldırı suçunun basit şekli için öngörülen ceza iki yıldan yedi yıla ka- darken, bugün suçun hafif
Figure 1: Triangular opacity in the right, mid-lower zone of the paracar- diac area can be seen obscuring the cardiac border on the right side with an obvious
Postoperative survival and the number of lymph nodes sampled during resection of node-negative non-small cell
and diagnostic accuracy of integrated positron emission tomography- computed tomography (PET-CT) and endobronchial ultrasound-guided transbronchial needle aspiration
dığı gazel bir Divana muadildir; Pa şa olan şairler içinde, keza her mıs raı, bir vecize, bir daılbımesel kudre tinde olan meşhur Ziya Paşa, isminin
Mart 1917'de 'National Society for the Promotion of Occupational Therapy' ilk toplantýsýný yapmýþ ve 1921'de 'American Occupational Therapy Associa- tion' adýný almýþtýr ve
Çalışanlar tarafından haber uçurma (whistleblowing) iki şekilde yapılmaktadır; içsel whistleblowing (internal whistleblowing), haber uçuranın örgüt içindeki ahlaki
