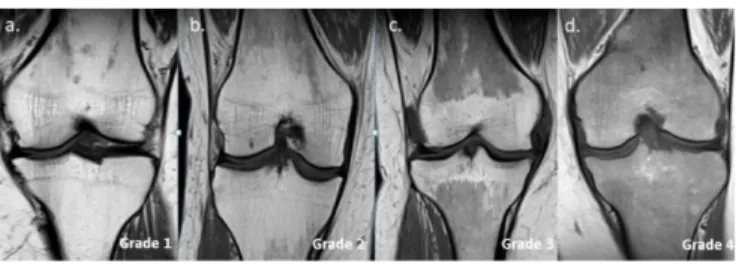
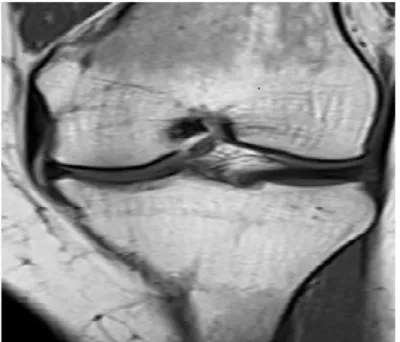
Evaluation of bone marrow reconversion in healthy adults with knee MRI
Tam metin
Şekil
Benzer Belgeler
Observed mucocutaneous signs were classified as infectious dermatosis (mucocutaneous candidiasis, paronychia, tinea versicolor), inflammatory dermatoses (asteatotic eczema,
We obtained the clinical characteristics of patients as well as their age, date of diagnosis of prostate cancer and BoMI, Gleason score, sites of metastases, complete blood
Astar Kumaşında Kullanılan Renkler: Ceket bedeni siyah, kol astar kumaşı beyaz üzerine. kahverengi
Mastitisin teĢhisi için oluĢturulan lojistik regresyon modelindeki bağımsız test değiĢkenleri üç aĢamada (birinci aĢama: sadece süt verim özellikleri (süt
Sonuç olarak; ikiz gebeliğin yaygın olduğu bir koyun işletmesinde karşılaşılan anomali olguları, düşük ve gebe kalamamaya bağlı olarak %25 oranında ciddi
alternative procedures to get an initial feasible solution: l j we randomly generate 100 feasible solutions and run the heuristic starting from each, recording the best
Tokat ilinde kentsel alanda yapılan bu araştırmada kişi başına tüketilen tavuk eti miktarı 8,15 kg/yıl olarak hesaplanmıştır.. Aylık kişi başı kanatlı eti
İlk olarak BBC, yeni medya piyasasına uyumlanma sürecinde öncü bir konumda yer almıştır ve ikili yayın stratejisi, kamu değer testi gibi uygulamaları ortaya çıkararak, birlik
