ORIGINAL ARTICLE
Histologic and Biomechanical Evaluation of the Effects of Social
Stress and the Antidepressant Fluoxetine on Tendon
Healing in Rats
Muhammed Besir Ozturk1&Onur Egemen2&Salih Onur Basat3&Ergün Bozdağ4&
Damlanur Sakız5
&Mithat Akan6
Received: 2 June 2015 / Accepted: 8 October 2015 / Published online: 15 October 2015 # Society of the Hand & Microsurgeons of India 2015
Abstract Impaired wound healing in humans under psycho-logical stress and the positive effects of antidepressant drugs on wound healing were also shown in the literature. However, there are currently no studies regarding the effects of antide-pressant drugs on tendon healing. The aim of this study was to compare tendon healing under normal conditions versus so-cial stress. We also aimed to perform a histological and bio-mechanical analysis of the effects of the antidepressant drug fluoxetine on tendon healing. Sixty Sprague Dawley rats were divided into six groups. A social stress regimen was used to stress the rats. The use of fluoxetine in the social stress group yielded significantly better biomechanical results and the col-lagen organizations of the fluoxetine group were more similar to the normal tendon collagen organization. Fluoxetine seems
to inhibit the negative effects of stress on tendon healing and seems to improve tendon healing.
Levels of Evidence: Level 5
Keywords Social stress . Fluoxetine . Tendon healing . Social stress and tendon healing . SSRI and tendon healing
Introduction
Hand injuries are among the most common injuries seen in daily life, and they constitute 6–28 % of trauma cases present-ing to the emergency departments [1].
Previous studies have shown that patients who have sustained hand injuries due to glass fisting are under high psychologic stress [2]. Inability to use the extremity during and after the operation, along with a long recovery period that requires phys-ical therapy create a significant psychologic stress on the patients. It has been shown that psychologic stress negatively affects wound healing [3]. Tendon healing is in fact a process of wound healing, consisting of the inflammation, proliferation/ repair, and remodeling phases [4].
Antidepressants were shown to have positive effects on wound healing [5]. However the effects of antidepressants on tendon healing have not been investigated.
The aim of this study was to analyze the effects of social stress and antidepressant fluoxetine on tendon healing, evalu-ate the differences between normal tendon healing and healing under antidepressant treatment, and assess the endurance, ten-sile strength, and histologic healing patterns of the tendon during the healing process in rats.
* Muhammed Besir Ozturk [email protected]
1
Department of Plastic Reconstructive and Aesthetic Surgery,
Tekirdağ Government Hospital, Tekirdağ, Turkey
2 Department of Plastic Reconstructive and Aesthetic Surgery, Liv
Hospital,İstanbul, Turkey
3
Department of Plastic Reconstructive and Aesthetic Surgery, Bağcılar Training and Research Hospital, İstanbul, Turkey 4
Faculty of Mechanical Engineering, Labaratory of Strength of Materials and Biomechanics, Istanbul Technical University, İstanbul, Turkey
5 Department of Pathology,Şişli Etfal Training and Research Hospital,
İstanbul, Turkey 6
Department of Plastic Reconstructive and Aesthetic Surgery,
Material and Method
The study was approved by the Bezmi Alem Vakıf University Animal Studies Local Ethics Committee (Ethics Committee Approval Date: 21.02.2012/Number: 2012–95).
The rat Achilles tendon healing model, which is used fre-quently as an animal model, was used also in this study [6,7]. Sixty rats weighing between 300 and 350 g were used for the study.
Groups
Sixty rats were separated into six groups: control 1 and 2, study 1 and 2, sham 1 and 2. There were ten rats each group, seven for biomechanical and three for histologic evaluations. Rats in the control group were operated without application of stress, the right Achilles tendons were cut and repaired surgically. The rats were sacrificed three or six weeks after the operation, and the repaired Achilles tendons were evalu-ated biomechanically and histologically.
Rats in the study group were operated after a 15 day long stress regimen. The right Achilles tendons were cut and repaired. Following the operation, they received intraperitone-al injection of Fluoxetine 1 mg/kg/day until they were sacrificed on either the third or sixth weeks. The Achilles tendons on the legs of animals sacrificed on the sixth week were evaluated biomechanically and histologically.
Rats in the sham group underwent transaction and repair of the Achilles tendon following a 15 day stress regimen. Animals in this group received 1 mgkg/day intraperitoneal injection of saline, and this treatment continued until they were sacrificed on the third and sixth weeks. The Achilles tendons of the animals sacrificed on the sixth week were eval-uated biomechanically and histologically.
Social Stress Regimen
A social stress regimen was applied to the animals as de-scribed previously [8]. The rats were kept in isolation for 24 h and in a crowded environment for 24 h. Isolation was applied by keeping the rat alone in a single cage, and crowded environment was applied by putting ten rats into each single animal cage.
Surgical Procedure
All the rats were operated by the same surgeon. A 1.5 cm long longitudinal incision was made on the posterior aspect of the right leg. The Achilles and plantaris tendons were exposed, the Achilles tendon was cut transversely with a scalpel, 0.5 cm proximal to its insertion point on the calcaneal bone. The plantaris tendon was also transected to prevent an internal splint effect.
The Achilles tendon was repaired with a 5–0 monofilament polypropylene suture (Propilen®, Doğsan, Turkey) on a round body needle, using the modified Kessler method. The skin was repaired with the same suture after tendon repair. No surgery was applied on the left Achilles tendons.
Sections including the Achilles tendon repair sites were prepared from all animals, three sections in each group were used for histologic evaluations and seven for biomechanical examination.
Histologic Evaluation
The sections were stained with hematoxylin and eosin stain, and evaluated under light microscope and polarized light.
Sections were blinded and the evaluation was performed by the same pathologist for the level of cellularity (fibroblast proliferation), the level of vascular proliferation, the level of inflammatory response (lymphocyte infiltration), the level of fibroblast organization and the amount of collagen matrix density between the cells. These were graded as (+: mild, ++ : moderate, +++: advanced).
Extracellular matrix-collagen density and the collagen alignments were evaluated under the polarized light micros-copy, and grading was performed based on the classification of Yuan et al. [9]. (Table1).
Biomechanical Evaluation
The cross sectional area examinations were done before the sectioning of the tendon from the widest and narrowest point of the tendon healing site using a micrometer (Series 523, Mitutoyo, Japan). Cross section areas were calculated by mul-tiplication of these values and expressed as mm2.
Achilles tendons were tested on the tension machine (MTS 858 Mini Bionix II, Eden Prairie, MN, U.S.A.) and the max-imum tension before rupture was measured in Newtons (N).
The maximum resistance at the time of rupture was divided by the cross section area of the tendon and Rupture Stress Values that showed the structural power of the tendon were found in N/mm2.
Statistical Evaluation
Mean and standard deviation were used in the complementary statistics of the data. The tests used during assessment were Kruskal Wallis Test which is used to compare the groups, Dunn’s Multiple Comparison Test which is used to compare the subgroups and Mann-Whitney-U test which is used to compare the differences between two independent groups. The level of significance was accepted asp < 0.05.
Results
Histologic Evaluation
Light microscopy evaluation revealed that the groups were similar with respect to cellularity, vascular proliferations, and inflammatory response. (Table2.)
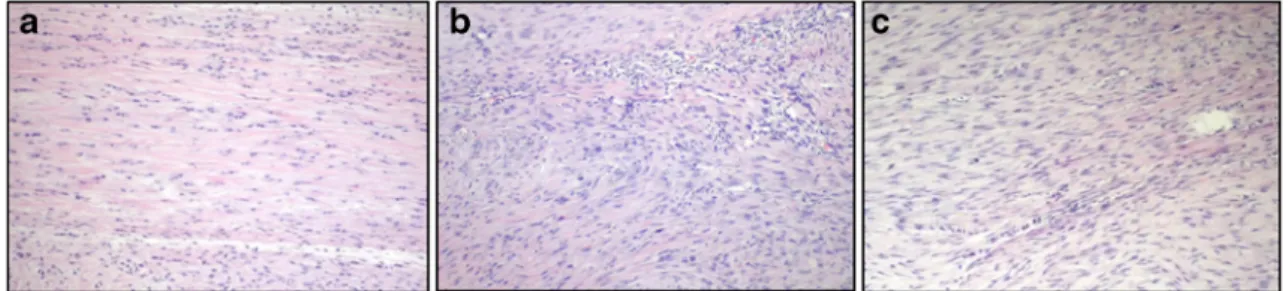
Evaluation of the three week groups (study 2, control 2, sham 2) showed that the sham group had less colla-gen density compared to control and study groups. In the study group collagen density was increased com-pared to other groups at the same weeks, in addition fibroblast alignment was more organized and parallel to the long axis of the tendon, similar to normal tenocytes. (Fig.1).
Evaluation of the sixth week groups (study 1, control 1, sham 1) revealed an increased collagen density in all groups compared to the third week. However when the study group was compared with the control and sham groups, collagen was more dense in the study group. Fibroblasts in the study group had flatter nuclei and more organized alignment. (Figs.2and3).
Polarized light microscopy examination showed that compared to the control and sham groups, collagen ac-cumulation in the study group was more organized and the ratio of collagen bundles (double refraction of po-larized light) was higher (Fig. 3.) Collagen alignment in the study groups was parallel to the long axis of the tendons, whereas it had a nodular style in other groups. (Table 2.)
Biomechanical Evaluation
The results of biomechanical evaluation are given on Table 3.
Prerupture maximum resistance in the third and sixth week study groups were significantly higher than the values in the control and sham groups (p < 0.05). Prerupture maximum resistance in the control group was significantly (p < 0.05) higher than the sham group on the sixth week, this difference was not significant (p > 0.05) on the third week. (Table3.)
Cross section area was significantly (p < 0.05) lower in the study group on both the third and sixth weeks when compared to the control and sham groups. Cross section area in the control group was significantly (p < 0.05) lower than the sham group on sixth week, this difference was not significant (p > 0.05) on the third week. (Table3.)
Rupture stress in the study group was significantly higher than the control and sham groups on both the third and sixth weeks (p < 0.05). Rupture stress was significantly (p < 0.05) higher in the control group than the sham group both on the third and sixth weeks. (Table3.)
Discussion
There are wide series in the literature showing that psychologic stress negatively affects wound healing [10–12]. A metaanalysis investigating various wound healing models showed that psy-chologic stress slowed wound healing by 42 % [13].
Table 2 Assessment of the groups under light microscopy and collagen alignment in polarized light examination
Fibroblast proliferation Vascular proliferation Inflammatory response Collagen density Fibroblast alignment Collagen Alignment
Ratio of Collagen bundles (double refraction of light)
Mean score
Study 1 +++ + + +++ +++ Fairly parallel Near Complete 4
Study 2 +++ + + ++ ++ Fairly parallel 40 % 3
Control 1 +++ + + ++ ++ Nodular 40 % 3
Control 2 +++ + + + + Nodular 20 % 2
Sham 1 +++ + + ++ + Nodular 10 % 2
Sham 2 +++ + + + + Nodular 20 % 2
Table 1 Assessment of collagen fibril organization with the polarized light microscope
Score 1 No bire-fringence of collagen fibre bundles, collagen fibres show no unique orientation.
Score 2 Collagen fibrils formed bundles. Collagen bundle ratio in cross section is <50 %, with loose network structure.
Score 3 Less than 50 % of collagen fiber bundles formed but with tight network structure.
Score 4 Over 50 % of collagen bundles formed in the healing site. These bands are aligned along the long axis of the tendon.
Poor wound healing will increase the surgery related wound complications. Tendon healing is basically a wound healing process, therefore such disorders will result in unde-sired results such as adhesions or ruptures in healing where the principal goal is functional recovery.
Previous studies showed that social isolation in rats is re-lated to anxiety and depressive behaviour, and fluoxetine ap-plication is protective against these effects [14].
In our study, we found a decreased collagen density on the third and sixth weeks in the sham groups compared to the study and control groups. This may be explained by suppres-sion of collagen synthesis by cortisone which is one of the factors responsible for the effects of stress on wound healing [15].
On the other hand, in the presence of chronic stress high glucocorticoid levels persist in the blood for a long time, resulting in the development of tolerance against glucocorti-coids at the cellular level. This effect results in an extreme inflammation in wound healing [16,17]. Other negative ef-fects of the glucocorticoids on wound healing include preven-tion of angiogenesis by suppression of VEGF, decreased pro-duction of factors necessary for wound healing such as IGF and TGF, suppression of collagen production, and increased production of proinflammatory cytokines by activation of macrophages through alternative routes [15,18–20]. In bio-mechanical tests, cross sectional areas in the sham group on the third week were significantly greater in the control and study groups. This may be explained by the proinflammatory
effect described above, the irregularity of collagen in a nodular and irregular way, and an irregular distribution of the fibro-blasts under the polarized light microscope.
A study on the effects of fluoxetine on wound healing in rats under stress similarly showed that collagen alignment and fibroblast distribution were irregular in the stressed groups [21].
Prerupture maximum resistance and rupture stress mea-surements on the sixth week sham group were significantly lower in the control and study groups on the same time period. When it is considered that tendon healing is basically a wound healing process, this finding may be considered to be consis-tent with other reports negative effects of stress on wound healing [22].
On the third week, prerupture maximum resistance values were similar between the sham and control groups but on the sixth week the measurements of the sham group was signifi-cantly lower. These results show that stress affects tendon healing especially during the late phase. However because the late three week period has a critical significance in the development of complications such as ruptures and adhesions after tendon repair, the prevention of negative effects during especially this phase is important.
Study of the collagen density in animals on the third and sixth week study groups revealed an increased density com-pared to sham and control groups on the same weeks. This effect may be explained by the fact that fluoxetine inhibits the
Fig. 2 a H/E evaluation of sixth week Study group tendon cross sections. There is an increased collagen density compared to the third week. Fi-broblasts have an organized alignment similar to normal tenocytes (X200). b H/E evaluation of sixth week Control group tendon cross
sections. Collagen density has increased compared to the third week. Fibroblast orientation is less organized compared to the Study group (X200)
Fig. 1 a H/E evaluation of third week Study group cross sections. Relatively increased collagen accumulation (red color in the background) and more organized fibroblasts are observed (×200). b H/E evaluation of third week Control group tendon cross sections. Collagen density is
relatively less. Fibroblast orientation is not organized (X200). c H/E evaluation of third week Sham group tendon cross sections. Collagen density is relatively less. The fibroblasts are organized. (X200)
glucocorticoids' suppression on collagen synthesis seen in chronic stress.
The study group had significantly smaller cross sectional areas on the third and sixth weeks compared to the control and sham groups. This difference may be explained by the antiinflammatory effects of fluoxetine during the early period and as well as to the regular alignment of collagen which is parallel to the long axis of the tendon under the polarized light microscope. Better rupture stress and prerupture maximum resistance values on the third and sixth weeks in the study group despite having smaller cross sectional areas than the control and sham groups support this explanation.
In addition to its known antidepressive effects, fluoxetine has anxiolytic and antinociceptive effects. The combination of all these effects contribute to the positive contribution of flu-oxetine on wound healing [23–25].
Wound healing consists of a balance between the inflam-mation period and healing. The disruption of this balance to-wards inflammation will delay healing.
Fluoxetine shows an antiinflammatory effect by signifi-cantly decreasing the levels of proinflammatory cytokines in-cluding IL-1β, IL-2, TNFα, and also by significantly increas-ing the levels of an antiinflammatory cytokine IL-10 [26,27]. Matrix metalloproteinases (MMP) are involved in wound healing by degradation of the extracellular matrix and remod-eling phases. A study performed on rats showed that fluoxe-tine inhibited the MMPs, suppressed inflammation by pre-serving intercellular links, and prevented neural injury by this route [28].
In addition to shifting the wound healing process toward healing by suppressing the inflammation, fluoxetine also im-proves microvascular circulation by affecting the thrombo-cytes, and increase NO synthesis and angiogenesis [29,30]. These may explain its positive effects on tendon healing.
One of the limitations of this study is that we did not per-form any tests to show the exact mechanism of the fluoxetine blocking the negative effects of the stress on tendon healing. Additional studies may overcome this limitation. Although the rat is not a human hand, and that these results are not evidence for an effect in humans, but do seem to justify further work in this area.
Conclusion
In our study the social stress in rats seems to have negative effects on tendon healing and the fluoxetine use seems to prevent these negative effects. In addition, the results of his-tological and biomechanical evaluations were found to be bet-ter in the fluoxetine group compared to the control group that was not exposed to stress and expected to have normal tendon
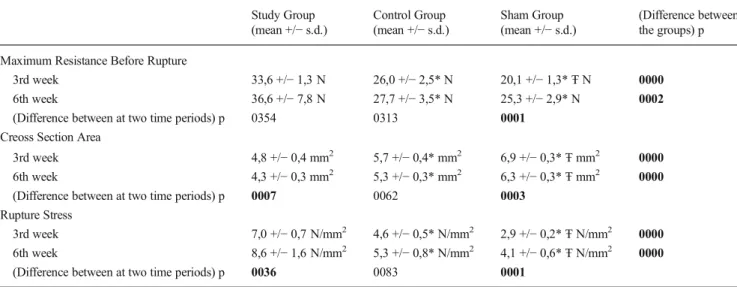
Table 3 Maximum resistance before rupture, cross section area and rupture stress measurements. Comparison of the values between groups
Study Group
(mean +/− s.d.) Control Group(mean +/− s.d.) Sham Group(mean +/− s.d.) (Difference betweenthe groups) p
Maximum Resistance Before Rupture
3rd week 33,6 +/− 1,3 N 26,0 +/− 2,5* N 20,1 +/− 1,3* Ŧ N 0000
6th week 36,6 +/− 7,8 N 27,7 +/− 3,5* N 25,3 +/− 2,9* N 0002
(Difference between at two time periods) p 0354 0313 0001
Creoss Section Area
3rd week 4,8 +/− 0,4 mm2 5,7 +/− 0,4* mm2 6,9 +/− 0,3* Ŧ mm2 0000
6th week 4,3 +/− 0,3 mm2 5,3 +/− 0,3* mm2 6,3 +/− 0,3* Ŧ mm2 0000
(Difference between at two time periods) p 0007 0062 0003
Rupture Stress
3rd week 7,0 +/− 0,7 N/mm2 4,6 +/− 0,5* N/mm2 2,9 +/− 0,2* Ŧ N/mm2 0000
6th week 8,6 +/− 1,6 N/mm2 5,3 +/− 0,8* N/mm2 4,1 +/− 0,6* Ŧ N/mm2 0000
(Difference between at two time periods) p 0036 0083 0001
*p < 0.05 difference with the study group/Ŧ p < 0.05 difference with the study group
ANOVA (Tukey test)/Independent Sample t test
Fig. 3 In polarized light microscopy of the sixth week study group, collagen fibers have double refraction of the light in wide field (white areas) and organized appearance are observed (×200)
healing. We believe that the use of fluoxetine may have pos-itive effects on tendon healing which should be supported with additional studies.
Acknowledgments The study was approved by the Bezmi Alem Vakıf
University Animal Studies Local Ethics Committee (Ethics Committee Approval Date: 21.02.2012 / Number: 2012-95). The study complied with the Europian standarts as described by European Council (2010/63/EU).
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
I would like to thank to Mr. Onur Egemen and Mr. Mithat Akan for the planning and the design of the study, to Mr. Salih Onur Basat for the
English translation and editing of the text, to Mr. Ergün Bozdağ for the
technical help of the biomechanical evaluation and to Ms. Damlanur Sakız for pathological examinations.
Compliance with Ethical Standards
Conflict of interest All named authors hereby declare that they have no
conflicts of interest to disclose.
References
1. Clark DP, Scott RN, Anderson IW (1985) Hand problems in an
accident and emergency department. J Hand Surg (Br) 10:297–299
2. Keskin D, Seçkin Ü, Bodur H, Sevil A, Erdoğan B, Akyüz M
(2005) Tendon yaralanmalı hastalarımızın klinik özellikleri. Türk
Fiz Tıp Rehab Derg 51:94–97
3. Altan L, Bingöl Ü, Selçuk A, Özkan N (2002) El yaralanmalı
hastaların sosyodemografik özellikleri ve yaralanmanın karakteristik özelliklerinin rehabilitasyon sonuçlarına etkisi. Romatol. Tıp Rehab 13:236–242
4. James R, Kesturu G, Balian G, Chhabra AB (2008) Tendon:
biol-ogy, biomechanics, repair, growth factors, and evolving treatment
options. J Hand Surg [Am] 33:102–112
5. Muppayyanavarmath SS, Patil PA (1999) The influence of tricyclic
antidepressants on resutured incision and dead space wound healing in albino rats. Indian J Pharm 31:290
6. Forslund C (2003) BMP treatment for improving tendon repair. Studies
on rat and rabbit Achilles tendons. Acta Orthop Scand Suppl 74:1–30
7. Kaux JF, Drion P, Libertiaux V, Colige A, Hoffmann A, Nusgens B,
Besançon B, Forthomme B, Le Goff C, Franzen R, Defraigne JO, Cescotto S, Rickert M, Crielaard JM, Croisier JL (2013) Eccentric training improves tendon biomechanical properties: a rat model. J
Orthop Res 31:119–124
8. Rygula R, Abumaria N, Havemann-Reinecke U, Rüther E, Hiemke
C, Zernig G, Fuchs E, Behav FG (2008) Pharmacological valida-tion of a chronic social stress model of depression in rats: effects of
reboxetine, haloperidol and diazepam. Pharmacol 19:183–196
9. Yuan J, Murrell GA, Wei AQ, Appleyard RC, Del Soldato P, Wang
MX (2003) Addition of nitric oxide via nitroflurbiprofen enhances the material properties of early healing of young rat Achilles
ten-dons. Inflamm Res 52:230–237
10. Grose R, Werner S, Kessler D, Tuckermann J, Durka S, Huggel K,
Reichardth H, Werner S (2002) A role for endogenous
glucocorti-coids in wound repair. EMBO Rep 16:575–582
11. Gouin JP, Kiecolt-Glaser JK (2012) The impact of psychological
stress on wound healing: methods and mechanisms. Crit Care Nurs
Clin North Am 24:201–213
12. Marucha PT, Kiecolt-Glaser JK, Favagehi M (1998) Mucosal
wound healing is impaired by examination stress. Psychosom
Med 60:362–365
13. Walbur NJ, Vedhara K, Hankins M, et al (2009) Psychological
stress and wound healing in humans: a systematic review and
me-ta-analysis. J Psychosom Res 67:253–271
14. Berton O, Durand M, Aguerre S, Mormede P, Chaouloff F (1999)
Behavioral, neuroendocrine and serotonergic consequences of sin-gle social defeat and repeated fluoxetine pretreatment in the Lewis rat strain. Neuroscience 92:327–341
15. Wicke C, Halliday B, Allen D, Roche NS, Scheuenstuhl H, Spencer
MM, Hunt TK (2000) Effects of steroids and retinoids on wound healing. Arch Surg 135:1265
16. Miller GE, Cohen S, Ritchey AK (2002) Chronic psychological
stress and the regulation of pro-inflammatory cytokines: a glucocorticoid-resistance model. Health Psychol 21:531–534
17. Avitsur R, Stark JL, Sheridan JF (2001) Social stress induces
glucocor-ticoid resistance in subordinate animals. Horm Behav 39:247–257
18. Bitar MS (2000) Insulin and glucocorticoid-dependent suppression
of the IGF-I system in diabetic wounds. Surgery 127:687–695
19. Rook G, Baker R, Walker B, et al (2000) Local regulation of
glu-cocorticoid activity in sites of inflammation. Insights from the study of tuberculosis. Ann N Y Acad Sci 917:913–922
20. Song E, Ouyang N, Horbelt M, et al (2000) Influence of
alterna-tively and classically activated macrophages on fibrogenic activities of human fibroblasts. Cell Immunol 204:19–28
21. Farahani RM, Sadr K, Rad JS, et al (2007) Fluoxetine enhances
cutaneous wound heal-ing in chronically stressed wistar rats. Adv Skin Wound Care 20:157–165
22. Christian LM, Graham JE, Padgett DA, Glaser R, Kiecolt-Glaser
JK (2006) Stress and wound healing. Neuroimmunomodulation 13: 337–346
23. Rossi A, Barraco A, Donda P (2004) Fluoxetine: a review on
evi-dence based medicine. Ann Gen Hosp Psychiatry 3:2
24. Nowakowska E, Chodera A, Kus K (1996) Anxiolytic and memory
improving activity of fluoxetine. Pol J Pharmacol 48:255–260
25. Bianchi M, Sacerdote P, Panerai AE (1994) Fluoxetine reduces
inflammatory edema in the rat: involvement of the
pituitary-adrenal axis. Eur J Pharmacol 263:81–84
26. Xia Z, DePierre J, Nassberger L (1996) Tricyclic antidepressants
inhibit IL-6, IL-1 beta, and TNF-alpha release in human blood monocytes and IL-2 and interferon-gamma in T cells.
Immunopharmacology 34:27–30
27. Kubera M, Simbirtsev A, Mathison R, Maes M (2000) Effects of
repeated fluoxetine and citalopram administration on cytokine
re-lease in C57BL/6 mice. Psychiatry Res 20(96):255–266
28. Lee JY, Kim HS, Choi HY, Oh TH, Yune TY (2012) Fluoxetine
inhibits matrix metalloprotease activation and prevents disruption of blood-spinal cord barrier after spinal cord injury. Brain 135:
2375–2389
29. Martinez-de Jesus FR, Morales-Guzman M, Castaneda M, et al (1997)
Randomized single-blind trial of topical ketanserin for healing
acceler-ation of diabetic foot ulcers. Arch Med Res 28:95–99
30. Witte MB, Efron DT, Kiyama T (1998) Wound fluid regulates nitric