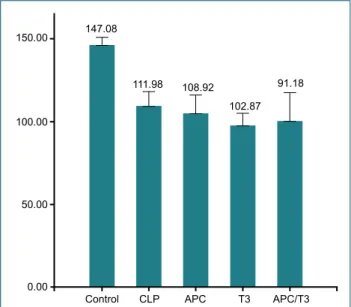
Is tri-iodothyronine a better choice than activated protein C in sepsis treatment?
Tam metin
Şekil
Benzer Belgeler
Es ki ener jik, gü ler yüz lü k›z git mifl, ye ri ne asa bi ve so murt kan bi ri gel
Antithrom- bin III deficiency concomitant with atrial fibrillation causes thrombi in all chambers: 2-D and 3-D echocardiographic evaluation.. Inherited antithrombin deficiency:
Antithrom- bin III deficiency concomitant with atrial fibrillation causes thrombi in all chambers: 2-D and 3-D echocardiographic evaluation.. Inherited antithrombin deficiency:
Bu sonuca varmak için koroner arter hastal›¤›n›n ba¤›ml› de¤iflken olarak al›nmas›, CRP düzeyleri ile di¤er risk faktörlerinin de ba¤›ms›z de¤iflken olmas›
A huge intracardiac thrombus developed in the presence of antithrombin III deficiency in a patient with end-stage renal failure.. Son dönem böbrek yetersizliği olan hastada
Dönen ve ucunda kütle bulunan visko-elastik bir Bernoulli-Euler çubuğunun, düzlem dışı titreşimlerinin incelenmesi temeline dayanan bu çalışmanın ikinci kısmında,
The aim of the present study was to investigate biodegradation of high concentrations of 2.4-DCP with adaptation of mixed culture in an activated sludge bioreactor and to
Objective: The primary aim of our study was to investigate the usefulness of serum C-reactive protein (CRP) and procalcitonin (PCT) levels in the differential diagnosis of
