www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Olfactory
rehabilitation
and
olfactory
bulb
volume
changes
in
patients
after
total
laryngectomy:
a
prospective
randomized
study
Defne
Gürbüz
a,
Mustafa
Caner
Kesimli
b,
Ahmet
Mert
Bilgili
c,∗,
Hacı
Ömer
Durmaz
daUniversityofHealthSciences,Prof.Dr.CemilTas¸c¸ıo˘gluCityHospital,DepartmentofRadiology, ˙Istanbul,Turkey bIstinyeUniversity,SchoolofMedicine,DepartmentofOtolaryngology,HeadandNeckSurgery, ˙Istanbul,Turkey
cCyprusInternationalUniversity,MedicalFaculty,DepartmentofOtolaryngology,HeadandNeckSurgery,Lefkos¸e,Cyprus dAvicennaPrivateHospital,OtorhinolaryngologyDepartment, ˙Istanbul,Turkey
Received16September2020;accepted28February2021
KEYWORDS Olfactory; Laryngectomy; Orthonasal; Rehabilitation; Training Abstract
Introduction:Aftertotallaryngectomy,decreasedolfactoryfunctionandolfactorybulbvolume shrinkagehavebeenreportedtooccurduetoolfactorydeprivationcausedbynasalairflow inter-ruption.Thereisevidencethattheolfactorysystemcanbemodulatedbyrepeatedexposureto odorsinaprocedurecalledolfactorytraining.However,itisnotknownwhetheranyrecovery ofthelostolfactorybulbvolumeispossiblebyeliminatingolfactorydeprivationviaolfactory rehabilitationlongafterlaryngectomy.
Objective:Thisstudyexaminedtherecoveryofolfactoryfunctionandthechangeinolfactory bulbvolumevialong-termolfactoryrehabilitationaftertotallaryngectomy.
Methods:Possiblecausesofolfactorydysfunctioninthestudyparticipantswereevaluatedby collectingdetailedanamnesis.Asolfactorytests,orthonasalbutanolthresholdandodor dis-criminationtestswereperformed.Three-dimensionalolfactorybulbvolumeswerecalculated usingmanual segmentationonT2-weightedcoronalmagneticresonanceimages.Inolfactory rehabilitation,four differentodorswere appliedto allpatients orthonasally,using alarynx bypasstechniquefor30minperdayfor6months.Olfactorytestswereperformedbeforethe rehabilitationandafter6monthsofrehabilitation,andolfactorybulbvolumemeasurements wereperformedusingmagneticresonanceimages.
Results:Elevenpatientsdiagnosedwithadvancedlaryngealcancerwhounderwenttotal laryn-gectomyandpostoperativeradiotherapywithafollow-upof5---10yearswereincludedinthe study.All patients weremale,andthemean agewas 58.18±4.17years.In total laryngec-tomizedpatients,theolfactorybulbvolumesmeasuredonmagneticresonanceimageswere 42.25±12.8mm3beforeand55.5±11.22mm3afterrehabilitation,andthisincreasewashighly
∗Correspondingauthor.
E-mail:[email protected](A.M.Bilgili).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
https://doi.org/10.1016/j.bjorl.2021.02.013
1808-8694/©2021Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
Introduction
Olfactorylossnotonlynegativelyaffectsqualityoflifebut mayevenjeopardizethepatient’spersonalsafetybecause oftheinabilitytodetectsmokeorotherdangerousolfactory signals.1
Theolfactorynerveisanervepertainingtosensory func-tionofsmell(olfaction)alone.Theolfactorysystemconsists oftheepithelium,bulb,andtractsassociatedwiththe cor-ticalolfactoryarea,alsoknownastherhinencephalon.The olfactorybulb(OB)consistsofthesensoryafferentsofthe olfactory receptor cells located in theolfactory neuroep-ithelium.TheOBisthoughttobethemostimportantstation of the olfactory pathways connecting the peripheral and corticalstructures.TheOBreflectsthelevelofafferent neu-ralactivityandmaintainsadegreeofplasticitythroughout adultlife.2
After total laryngectomy, air flow does not reach the olfactory mucosa due to interrupted nasal airflow; as a result,theolfactorycenterisdeprivedofolfactorystimuli. Frequently,thisdeprivationsoonleadstoseverehyposmia and anosmia. Despite being reported in laryngectomized patients,thisolfactoryloss hasbeen widelyoverlooked in previousstudies.1---3 Asaresultofolfactorystimulus depri-vation, the OB volume diminishes due to decreased cell numbersovertime.4Interruptednasalbreathingasaresult of tracheostomy after laryngectomy leads to significant olfactory loss in patients. Significantly impaired olfactory abilityhasbeenobservedinlaryngectomizedpatients.5,6
Magneticresonanceimaging(MRI)isareliableandideal technique for OB volume measurements. The OB volume also reflects the functionalstatus of this structure in the humanolfactorysystem duetoitsplasticity.RegardingOB volume measurements, post-traumatic olfactory dysfunc-tionandneurodegenerativediseaseshavebeenevaluatedin totallaryngectomizedpatientsandindividualswithnormal olfaction.7---9 Veyseller et al. demonstrated in both cross-sectionalandlongitudinalstudiesthatolfactorydysfunction andOBvolumeshrinkageoccurinlaryngectomypatients.5,6 As yet,noeffective methodisuniversallyacceptedfor thetreatmentofolfactorydysfunction.Olfactory rehabili-tationthrougholfactorytrainingconsistsofmodulatingthe systemicregeneration process byrepeatedly exposing the olfactorysystemtoparticularodors.10
Significant improvements inolfactory test results after olfactory training in patients with post-traumatic and
post-infectiousolfactorydysfunctionhavebeenreported.11 The training is performed once a day using four odors: phenylethyl alcohol (rose), eucalyptol (eucalyptus), cit-ronellal (lemon), and eugenol (clove).12,13 There are also studiesontheimprovementofolfactoryfunctionin laryn-gectomypatientsviaolfactoryrehabilitation.1,14,15
This study was conducted prospectively and longitu-dinally in patients after laryngectomy to demonstrate improvementsinolfactoryfunctionandchangesinOB vol-umesviaolfactoryrehabilitationachievedbyrestorationof nasalairflow.
Methods
This prospective study wasconducted on patients admit-tedtothe Ear,NoseandThroat(ENT)andHeadandNeck SurgeryClinicwiththe assistanceof theRadiology Clinic. Thestudywascarriedoutinaccordancewiththe Declara-tionofHelsinki(WMA1997).Approvalwasobtainedfromthe ethicscommittee,andtheparticipantsgavewrittenconsent afterbeinginformedaboutthestudy.(Approvalnumberof theethicscommittee:(2017-KAEK-120)/2/2020.G-068).
Patientswith ahistory of nasal polyposis,neurological orpsychiatricdiseases, headtraumaor nasalsurgerythat maycauseolfactoryimpairmentbeforelaryngectomywere excluded.RoutineENTexaminations,paranasalsinus com-putedtomography, orthonasal olfactory tests,and cranial MRI were performed for OB volume measurements in all patients. CranialMRI and orthonasal olfactory tests were conductedbeforeand6-monthsafterlaryngectomy.In addi-tion,acompleteneurologicalexaminationandMini-Mental evaluationtests,aswellascranialMRI,wereperformedto excludepossible cognitivedisorders or neurodegenerative diseases.
The orthonasal olfactory test devisedby the Connecti-cut Chemosensory Clinical Research Center (CCCRC) was used.16,17 The possible score ranges obtained from the CCCRCorthonasaltestsareshowninTable1.
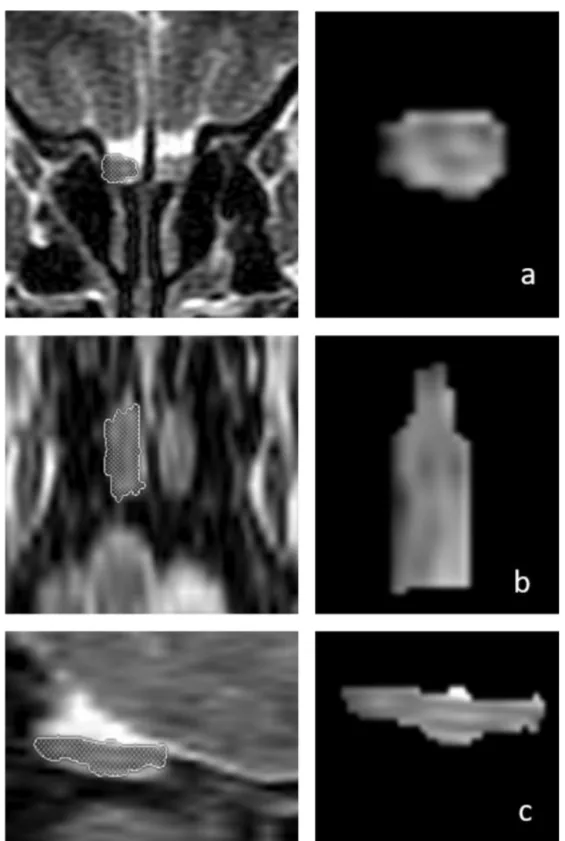
OBvolumemeasurementswereperformedbyMRIimages (Fig. 1) using the 1.5T General Electric Signa Excite MRI device by three-dimensional evaluation on coronal T2-weighted Turbo Spin Echo (TSE) sections using a manual segmentationmethod.Thesectionshadaslicethicknessof 2mmwithoutintersectiongaps(gap=0).Allmeasurements wereperformedbythesameexperiencedradiologist, sep-2
Figure1 Three-dimensionalmeasurementsoftherightolfactorybulb(OB)volumeina66-year-oldmalepatientonT2-weighted coronal(a,firstrow),axial(b,middlerow),andsagittal(c,bottomrow)magneticresonanceimages.Thepatient’srightOBvolume was76mm3afterolfactoryrehabilitation.
aratelyfrombothsides,withoutknowledgeofwhetherthe imageswereobtainedbeforeoraftertreatment.OBvolume measurementswerecalculatedinmm3(Figs.1and2).11,12
Patientswithpost-traumaticparenchymalor meningeal hemosiderinaccumulationin braintissues onT2-weighted GradientEchoSequence(GRE)MRIsectionswereexcluded from the study. In addition, conventional cranial MRI
sequenceswerescreenedforotherorganicdisordersofthe brain, and individuals with any pathology were excluded fromthestudy.
For olfactory rehabilitation, air flow was provided to the nasal olfactory mucosa, and access of odor particles totheolfactoryregionwasachievedusingalarynxbypass technique.Duringolfactoryrehabilitation,thetrainingwas
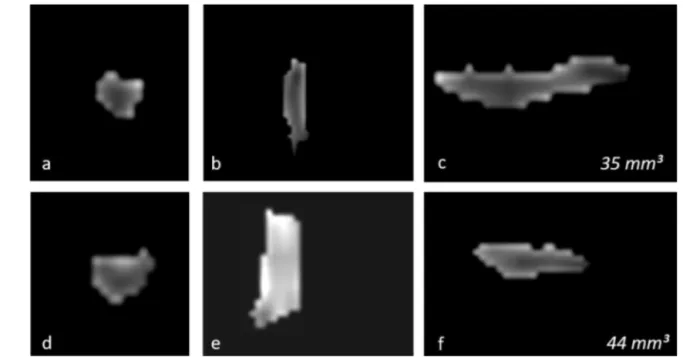
Figure2 Changesinthethree-dimensionalvolumemeasurementoftheleftOBinatotallaryngectomizedpatientonmagnetic resonanceimages,beforeolfactoryrehabilitation(a---c,upperrow)andafterolfactoryrehabilitation(d---f,lowerrow),ascoronal (a,d),axial(b,e),andsagittal(c,f)images,respectively.TheleftOBvolumewas35mm3and44mm3beforeandafterolfactory
rehabilitation.
Table1 CCCRCscoreranges.
Scoreranges Anosmia 0---1.75 Severehyposmia 2---3.75 Moderatehyposmia 4---4.75 Mildhyposmia 5---5.75 Normosmia 6---7
performed for30min adayfor6monthsusingfourodors: phenylethyl alcohol (rose), eucalyptol (eucalyptus), cit-ronellal(lemon),andeugenol(clove).
Inthissection,weperformstatisticalanalysisto inves-tigateiftherehabilitation helpscounteract thereduction inCCCRCscoresandOBvolumesduetolaryngectomy(i.e., aretheCCCRCscoresandOBvolumeshigherafter6months ofpostoperativerehabilitationcomparedtorightafterthe laryngectomy?).Weconsiderthattheresultswithap-value lessthan0.05arestatisticallysignificant.
Descriptive statisticsarepresentedin theTable2.The majority of the patients aremiddle-aged (range: 52---66), andtheANCOVAanalysisrevealsthat‘‘age’’doesnothave
astatisticallysignificanteffectonthedifferenceinCCCRC scoresandOBvolumespre/postrehabilitation,andthuscan besafelyeliminatedfromfurtheranalysis.
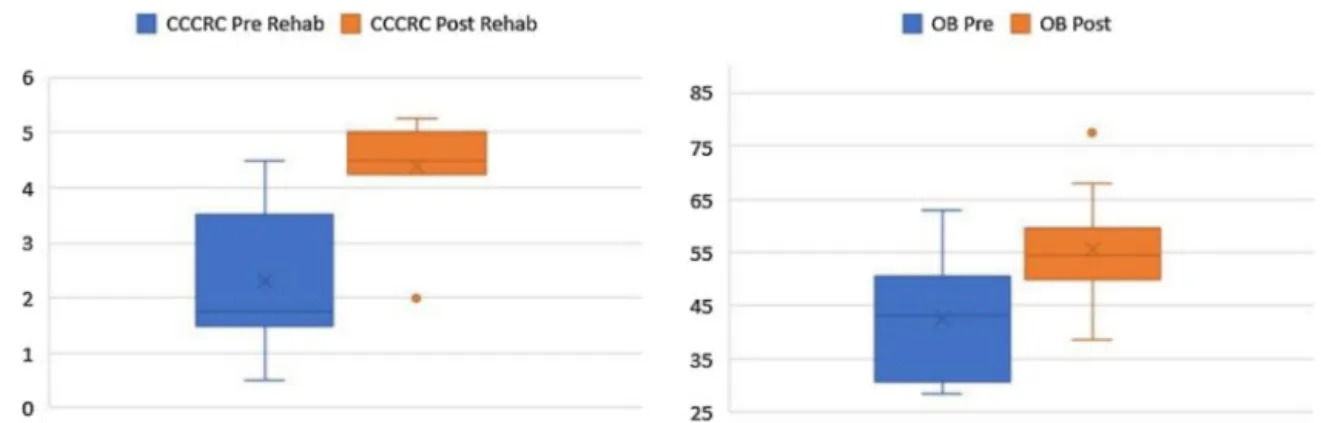
According tothebox plots in Fig.1,the CCCRCscores and OB volumes are noticeably higher as a result of the rehabilitation, in line with our prior belief that the rehabilitation helps increase CCCRC scores and OB vol-umes.The Wilcoxon test for paired samplesalsoconfirms thatthepost-rehabilitationCCCRCscoresandOBvolumes arehigherthan thepre-rehabilitation valuesmeasured 6-monthsapart (highlystatistically significant withp-values
of0.001)(Fig.3).
Results
A totalof 11 patients diagnosed withadvanced laryngeal cancerwereincluded.Allpatientsweremale.Theyoungest andoldestpatientswere52and66yearsold,withamean ageof58.18±4.17years.Allpatientshadahistoryof smok-ing----mean25(range10---40)cigarettes/day.
Inall11laryngectomizedpatients,themeanOBvolume beforerehabilitationwas42.5(withastandarddeviationof 12.8andrange28.5---62.5)mm3 (Table2),while themean
Table2 Descriptivestatistics.
Group1(prerehab,n=11) Group2(postrehab,n=11)
Variables Mean SD Median Range Mean SD Median Range
Age(yr) 58.18 4.17 58 (52---66) 58.18 4.17 58 (52---66)
CCCRC 2.3 1.27 1.75 (0.5---4.5) 4.39 0.86 4.5 (2---5.25)
OB 42.5 12.8 43 (28.5---63) 55.5 11.22 54.5 (38.5---77.5)
Figure3 BoxplotsforCCCRCscoresandOBvolumespre/postrehabilitation.
Table 3 Patient distribution among the CCCRC score categories. Category Before rehabilitation 6-monthsafter rehabilitation Normal 0 0 Mildhyposmia 0 3 Moderatehyposmia 1 5 Severehyposmia 3 2 Anosmia 6 0 Total 10 10
OBvolume measured after6 months of olfactory rehabil-itation was 55.5 (with a standard deviation of 11.22 and range 39.5---77.5)mm3. The OB volume was significantly
largerafterthanbeforeolfactoryrehabilitation(p<0.001) (Fig.1).
CCCRC mean scores (butanol threshold and odor iden-tification scores) were 2.3±1.27 (range 0.50---3.25) and 4.39±0.86(range2.50---5.25)(outof7)beforeandafterthe 6-montholfactoryrehabilitation,respectively.Theincrease inthescoreaftertherehabilitation(attheendof6-months) was statistically significant (p<0.001) (Fig. 1). According totheCCCRC scoring system,the scoreof 2.3in patients beforerehabilitationindicatedseverehyposmia,whilethe score of 4.39 afterrehabilitation demonstrated moderate hyposmia.
According to the CCCRC scores before rehabilitation, onepatientwasmoderatelyhyposmic,threewereseverely hyposmic,andsixwereanosmic.Afterrehabilitation,three patientsweremildlyhyposmic,fiveweremoderately hypos-mic,andtwowereseverelyhyposmic(Table3).
Discussion
Due totracheostomy performed after totallaryngectomy, the nasal airway is interrupted, and the neuroepithelium specializedforolfactionisdeprivedofodorparticles.6Two mechanismspotentiallyexplainingolfactorylossafter laryn-gectomyareinterruptionofnasalairflowafterlaryngectomy and impairment of neurosensory feedback mechanisms after multiple peripheral nerve injuries during surgery.5 The OB displays plasticity throughout adult life, based
ontwomajor neurobiological mechanisms; oneis related to the continuity of neurogenesis from the subventricu-lar zone, and the other is related to the continuity of synaptogenesis.18
A reduction in OB volumes resulting in hypoplasiahas been shown tobe the most important effectof olfactory stimuli deprivation in animals.4 The continuity in the OB neuroblastflow fromthe subventricularzoneinhumansis describedintheCNS(CentralNervousSystem).18
Bulbarneuroplasticityisassociatedwithinputfrom olfac-tory receptor neurons.19 The continuity of neurogenesis, which is sensitive to environmental factors and stimuli, resultsin neural recruitment,andsensitivity improves OB volume.19
Shehataetal.demonstratedthatinpatientswithchronic rhinosinusitiswithnasal polyposis,postoperative improve-mentin olfactoryfunction andan increase inOBvolumes occurred6monthsafterremovalofthenasalblockade.20
Althoughpulmonaryandvocalproblemsaftertotal laryn-gectomyhavebeenwidelycoveredintheliterature,there arefewstudiesonthedeteriorationofolfactoryfunction.1 OBvolumes measured postoperativelyin laryngectomized patientswerereportedtobelowerthanthoseinasimilar agecontrolgroup.5,6Atrophyoftheolfactory neuroepithe-liumortheOBmayplayaroleintheemergenceofolfactory problemsinpatientsafterlaryngectomy.6,18,19,21
The pathophysiology of olfactory reduction in laryn-gectomized patients is not fully understood, and several theorieshavebeenproposed.Theinterruptionof nasopul-monaryairflow inlaryngectomizedpatientsautomatically interruptsthepassivesniffingmechanism.Mianietal. sug-gestedthatdegenerationof theolfactory epitheliummay result from atrophy, inflammation, or disuse. Laryngec-tomy patients show severe degeneration of the olfactory epithelium.22
Inourstudy,althoughmorethan5yearshadpassedsince laryngectomyandolfactoryloss,thepatientsrespondedto olfactoryrehabilitation, andbothodor perceptionand OB volumesincreased.Thissupportsthefactthat,afterits acti-vation,theolfactorysystemcanregainitsformerfunctions andstructureduetoitsplasticity.
Ourstudyisimportantinthatitshowedincreasesinboth CCCRCscoresandOBvolumesasaresultofolfactory reha-bilitationafterlaryngectomy.
EthicsapprovalwasobtainedfromthelocalResearchEthics Committeepriortothestudy.
Everyparticipantpatientwasinformedcomprehensively about the studyand informedconsentwasobtained from eachofthem.
Thisstudywasconductedinaccordancewiththetenets oftheDeclarationofHelsinki.
Allauthorshavesubstantialcontributionstoconception anddesign,acquisitionofdata,oranalysisand interpreta-tionofdata.
All authors have taken part by drafting the article or revisingitcriticallyforimportantintellectualcontent.
Allauthorshavefinalapprovaloftheversiontobe pub-lished.
All authorsagreed tobe accountablefor allaspects of thework.
References
1.GoektasO,FleinerF,FrielerK,SchererH,PaschenC.The scent-diffusingventilatorforrehabilitationofolfactoryfunctionafter laryngectomy.AmJRhinology.2008;22:487---90.
2.Ackerstaf AH, HilgersFJM,Aarson NK,Balm AJM. Communi-cation,functionaldisorders,and lifestylechangesaftertotal laryngectomy.ClinOtolaryngol.1994;19:295---300.
3.FujiiM,FukazawaK,HattaC,YasunoH,SakagamiM.Olfactory acuityaftertotallaryngectomy.ChemSenses.2002;27:117---21.
4.Cummings DM, Knab BR, Brunjes PC. Effects of unilateral olfactorydeprivationinthedevelopingopossum,Monodelphis domestica.JNeurobiol.1997;33:429---38.
5.VeysellerB,OzucerB,AksoyF,YıldırımYS,GürbüzD,Balıkc¸ıHH, etal.Reducedolfactorybulbvolumeanddiminishedolfactory functionintotallaryngectomypatients:aprospective longitu-dinalstudy.AmJRhinolAllergy.2012;26:191---3.
6.Veyseller B, Aksoy F, Yildirim YS, Bayraktar FGI, Gurbuz D, SavasD,etal.Reducedolfactorybulbvolumeintotal
laryngec-HuttenbrinkKB.Effects ofolfactory traininginpatientswith olfactoryloss.Laryngoscope.2009;119:496---9.
11.Konstantinidis I, Tsakiropoulou E, Bekiaridou P, Kazantzi-dou C, Constantinidis J. Use of olfactory training in post-traumaticandpostinfectiousolfactorydysfunction. Laryn-goscope.2013;123:E85---90.
12.KonstantinidisI,TsakiropoulouE,Constantinidis J.Longterm effects ofolfactory trainingin patients with post-infectious olfactoryloss.Rhinology.2016;54:170---5.
13.PellegrinoR,HanP,ReitherN,HummelT.Effectivenessof olfac-tory trainingondifferent severities ofposttraumatic lossof smell.Laryngoscope.2019;129:1737---43.
14.GöktasO,FleinerF,PaschenC,LammertI,SchromT. Rehabili-tationoftheolfactorysenseafterlaryngectomy:long-termuse ofthelarynxbypass.EarNoseThroatJ.2008;87:528---30.
15.MoorJW,RaffertyA,SoodS.Canlaryngectomeessmell? Con-siderations regarding olfactory rehabilitation following total laryngectomy.JLaryngolOtol.2010;124:361---5.
16.Cain WS, Gent JF, Goodspeed RB, Leonard G. Evaluation of olfactorydysfunctionintheConnecticutChemosensoryClinical ResearchCenter.Laryngoscope.1988;98:83---8.
17.LeonEA,CatalanottoFA,WerningJW.Retronasalandorthonasal olfactory ability after laryngectomy. Arch Otolaryngol Head NeckSurg.2007;133:32---6.
18.CurtisMA,KamM,NannmarkU,AndersonMF,AxellMZ,Wikkelso C,etal.Humanneuroblastsmigratetotheolfactorybulbviaa lateralventricularextension.Science.2007;315:1243---9.
19.LledoPM,GheusiG.Olfactoryprocessinginachangingbrain. Neuroreport.2003;14:1655---63.
20.ShehataEM, TomoumMO, AmerMA, AlarabawyRA, Eltomey MA.Olfactorybulbneuroplasticity:aprospectivecohortstudy inpatientswithchronicrhinosinusitiswithnasalpolyps. Clin Otolaryngol.2018;43:1528---34.
21.MaruniakJA.Deprivationandolfactorysystem.In:DotyRL, edi-tor.Handbookofolfactionandgustation.NewYork,NY:Marcel DekkerInc.;1995.p.455---69.
22.MianiC,OrtolaniF,BracaleAM,PetrelliL,StaffieriA,Marchini M.Olfactorymucosahistologicalfindingsinlaryngectomees.Eur ArchOtorhinolaryngol.2003;260:529---35.