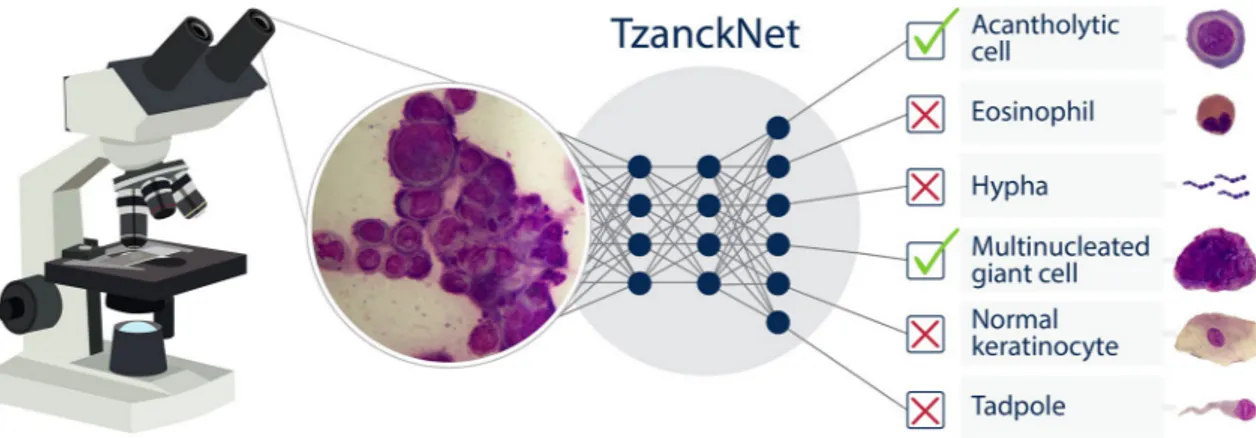
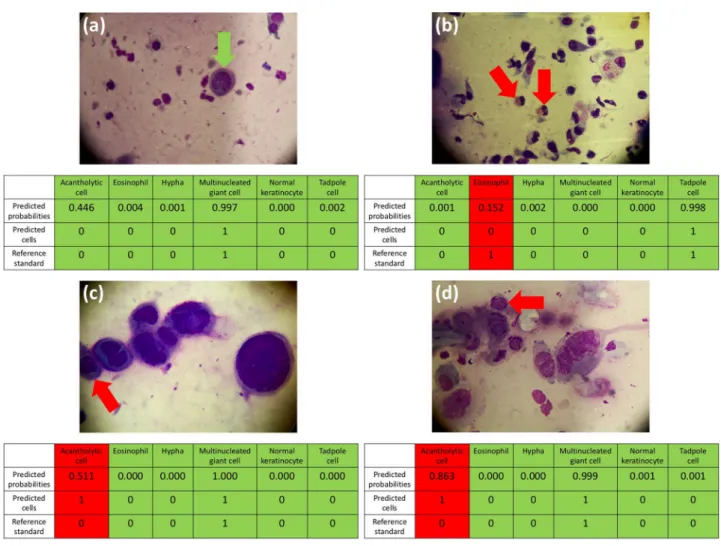
TzanckNet: a convolutional neural network to identify cells in the cytology of erosive-vesiculobullous diseases
Tam metin
Şekil
Benzer Belgeler
Kırk çeşme mahallesinde üç değirmen Hızır Bey Çelebi mahallesinde değirmen Üskûbi mescidi mahallesinde iki değirmen Küçük Mustafa Paşa hamamı yanında
Okuyucunun bu kitapta de ğişik bir kalıp değil, yeni bir ruh aramasını isterim. ZAMAN
Kronolojik ve bilimsel bir sınıflandırmayla yazılmadığı için tam değil sözünü kullanıyorum, bu anılar, da ha çok meslek hayatımda gördüğüm, ak
Türkiye’deki Hıristiyanların di ni eğitimlerini sürdürebilmeleri için yapılan ayinlere İstanbul’ da yaşayan azınlıkların dışında Müslüman Türkler de
Şu halde millî karakteri gelı> - tirmek için, onu kendi kudretleri ve geleneği içinde yaratıcı kılmak lâ zımdır : Bir milletin sanatta, ilimde,
Nadir Nadi, Gide misalini verdikten son ra, Nazım Hikm et’in aksine davranışların dan söz ediyor: “ Nazım ilk gidişinde Stalin’i öylesine göklere çıkardı ki, bu
This research was carried out in order to evaluate the quality practices of Ondokuz Mayıs University Health Application and Research Center (Turkey) within the framework of
In our study, by measuring the plasma AOPP and serum AGE levels as oxidative stress markers, we aimed to determine whether there is a relationship between oxidative stress markers
