Hereditary hemorrhagic telangiectasia with multiple fusiform
retinal aneurysms
Nagihan Uğurlu&Selma Emre&Fatma Yülek&
Emine Kalkan Akcay&Ahmet Sengun
Received: 9 December 2012 / Accepted: 17 January 2013 / Published online: 29 January 2013 # Springer Science+Business Media New York 2013
Introduction
Hereditary hemorrhagic telangiectasia (HHT) is a rare genetic disorder characterized by abnormalities of vascular structures involving skin, mucosal membranes, and other organs. A wide variety of clinical manifestations have been associated with HHT ranging from small telangiectasia on face causing only cosmetic problems to life-threatening visceral arteriovenous malformations leading to systemic emboli, hepatic dysfunc-tion, and high output cardiac failure. These diverse clinical manifestations develop according to the localization and the severity of the vascular abnormalities.
Ocular involvement is common in HHT and conjunctival telangiectasia is the most common ocular lesion. Retinal tel-angiectasia, retinal arteriovenous malformations, and choroi-dal telangiectasia are other relatively rare ocular findings [1–3]. We herein present a case of HHT with bilateral multiple retinal fusiform aneurysms and conjunctival telangiectasia.
Case report
A 38-year-old woman with the diagnosis of HHT was exam-ined from the dermatology clinic for investigation of ocular involvement. She had a history of recurrent epistaxis and there were several spots of telangiectasia distributed on her arm, back, thigh, and buccal mucosa especially apparent for the last 3 years (Figs.1and2). Her family history was negative for HHT and she was not taking any anticoagulant medication.
The best corrected visual acuity was 10/10 in both eyes. Numerous conjunctival telangiectasias on nasal bulbar con-junctiva and spider-like angiomatous malformations on the caruncula and the forniceal conjunctiva in the neighborhood of the caruncula were noted during biomicroscopic exami-nation (Fig.3). Fundus examination revealed tortuosity and multiple fusiform dilatations in all of the branches of the retinal vein and fine telangiectatic capillaries in both eyes (Fig.4). The macula and the optic disc were normal. Neither hemorrhage nor exudate was observed. The fundus fluores-cein angiogram did not show any leakage or capillary non-perfusion while the walls of retinal veins were stained (Fig. 5). The OCT examination of the macula was normal. The investigations done for the patient included: kidney and liver function tests including HbA1c and spot glucose level, ACE level, chest radiography, erythrocyte sedimentation rate, HLA B51, rheumatic factor, antinuclear antibodies,
double-stranded DNA, antineutrophil cytoplasmic antibod-ies, C-reactive protein, complement level (C3 and C4), Brucella, toxoplasmosis, and Borrelia titers, HBsAg, VDRL level, prothrombin time, partial thromboplastin time, and hemoglobin electrophoresis. Of these, only HLA B51 was
positive and all other results were normal. Pathological
N. Uğurlu
:
F. Yülek:
E. K. AkcayAtatürk Research and Training Hospital, Department of Ophthalmology, Yıldırım Beyazıt University, Ankara, Turkey S. Emre
Atatürk Research and Training Hospital, Department of
Dermatology, Yıldırım Beyazıt University, Ankara, Turkey
A. Sengun
Department of Ophthalmology, Ufuk University School of Medicine, Ankara, Turkey
N. Uğurlu (*)
48.cadde 1474. Sokak 3/10 Çukurambar, Ankara, Turkey e-mail: [email protected]
j ocul biol dis inform (2012) 5:48–50 DOI 10.1007/s12177-013-9100-y
examination of biopsy material taken from lesions in the back region showed ectatic proliferating small vascular structures in the papillary dermis. Since only one minor criterion, HLA B51 positivity, was present and any other
major findings were absent, the diagnosis of Behçet’s dis-ease was not being considered.
Discussion
The ophthalmological findings observed in this patient were conjunctival and retinal vascular abnormalities. The clinical and the angiographic appearances of retinal lesions were characterized by increased tortuosity and multiple aneurys-mal dilatations along retinal veins without associated find-ings such as exudate, hemorrhage, leakage, or capillary non-perfusion. As extraocular findings, she had multiple muco-cutaneous telangiectasia involving her back, extremities, inguinal area, and buccal mucosa. The patient was com-plaining of frequent epistaxis also.
Generalized mucocutaneous telangiectasia with ocular involvement is seen in very few conditions. Mainly, gener-alized essential telangiectasia (GET), ataxia telangiectasia (AT) and HHT are the diseases where concomitant ocular and cutaneous telangiectasias were reported.
Generalized essential telangiectasia is a rare disease affect-ing young healthy women. The condition is characterized by spontaneous development and progressive spreading of telan-giectasia. Although the age and the clinical course of skin lesions of our patient may resemble to GET, the presence of epistaxis, which is not the component of GET, excluded the diagnosis. Moreover, although conjunctival involvement was reported, retinal involvement also has not been reported with GET.
Ataxia telangiectasia is another disease in which accom-panying cutaneous and ocular telangiectasias are seen. In this disease, the age of onset is the first 2 years of life with progressive neurological dysfunction, immunodeficiency, and recurrent sinopulmonary infections. The age and gener-al hegener-alth status of our patient can easily exclude the diag-nosis of AT. Retinal telangiectasia also is not a reported finding of AT.
Idiopathic retinitis, vasculitis, aneurysms, and neuroretini-tis (IRVAN) syndrome is a rare characterized by the presence of multiple aneurysmal dilatations along the arteriolar tree. Three major criteria of IRVAN are retinal vasculitis, aneurys-mal dilatations at arterial bifurcations, and neuroretinitis which do not conform to the findings of our patient [4]. Moreover, IRVAN is limited to eye and extraocular findings
Fig. 2 Telangiectasia on her buccal mucosa
Fig. 3 Multiple telangiectatic vessels and spider-like angiomatous malformations on the caruncula
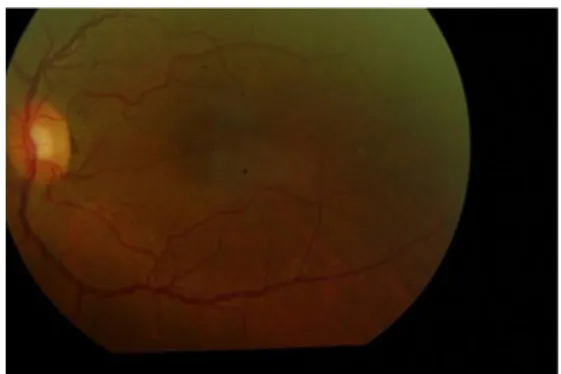
Fig. 4 Increased tortuosity and multiple fusiform aneurysms along the inferior and superior temporal retinal veins and fine telangiectatic capillaries temporal to macula
Fig. 1 Widespread telangiectatic lesions on her back
of our patient such as epistaxis and mucocutaneous telangiec-tasia are not found in IRVAN.
Hereditary hemorrhagic telangiectasia is also another disorder in which both retinal and conjunctival telangiecta-sia with mucocutaneous telangiectatelangiecta-sia is seen. HHT is a rare vascular disease characterized by vascular abnormalities. The hallmark of vascular lesions in HHT is the thinning and the dilatation of the vessel walls which make the vessels friable and increase the risk of bleeding. Whole vasculature throughout the body may be affected and may lead to the manifestations such as epistaxis, gastrointestinal bleedings, mucocutaneous telangiectasia, and pulmonary embolism.
Ocular involvement is common (45–65 %) in HHT and the most frequent ocular location is conjunctival telangiec-tasia. It has been reported in 35–38 % of HHT cases and it is harmless being not accepted as an indicator of visceral involvement [1–3].
In contrast to conjunctiva, intraocular involvement of HHT is a rare finding and includes abnormalities in the retinal and the choroidal vascular beds. Retinal vascular abnormalities, which had been reported in 10 % of cases, are the tortuosity and the dilatation of the retinal vessels, retinal telangiectasia, new optic disc vessels, and retinal arteriovenous malformations [1, 3, 5] while
the only reported choroidal lesion which may lead to surgical complications is telangiectasia [6].
Landau et al. reported a family of HHT with both conjunctival and retinal telangiectasia and described the retinal lesions as tortuous veins resembling twisted cords and suggested varices [5]. Brand observed retinal involvement in 2 of 20 HHT patients. One of them had numerous telangiectatic vessels on papillomacular bun-dle and other had multiple foci of fine telangiectasia throughout the retina [1]. Ocular lesions in HHT are generally stable and rarely cause symptoms. Only in one case with symptomatic parafoveal telangiectasia photodynamic therapy had been reported [7]. To our knowledge, multiple fusiform aneurysms had never been reported before as a finding of HHT.
Conflict of interest None of the authors has conflict of interest with
the submission.
References
1. Brant AM, Schachat AP, White RI. Ocular manifestations in hered-itary hemorrhagic telangiectasia (Rendu-Osler-Weber disease). Am
J Ophthalmol. 1989;107:642–6.
2. Geisthoff UW, Hille K, Ruprecht KW, et al. Prevalence of ocular manifestations in hereditary hemorrhagic telangiectasia. Graefes
Arch Clin Exp Ophthalmol. 2007;245:1141–4.
3. Vase I, Vase P. Ocular lesions in hereditary haemorrhagic
telangiec-tasia. Acta Ophthalmol (Copenh). 1979;57:1084–90.
4. Samuel MA, Equi RA, Chang TS, et al. Idiopathic retinitis, vascu-litis, aneurysms, and neuroretinitis (IRVAN): new observations and
a proposed staging system. Ophthalmology. 2007;114:1526–9.
5. Landau J, Nelken E, Davis E. Hereditary haemorrhagic
telangiecta-sia; with retinal and conjunctival lesions. Lancet. 1956;271:230–1.
6. Mahmoud TH, Deramo VA, Kim T, et al. Intraoperative choroidal hemorrhage in the Osler-Rendu-Weber syndrome. Am J Ophthalmol. 2002;133:282–4.
7. Mennel S, Hoerle S, Meyer CH. Photodynamic therapy in symp-tomatic parafoveal telangiectasia secondary to Osler-Rendu-Weber
disease. Acta Ophthalmol Scand. 2006;84:273–5.
Fig. 5 Angiographic images of the patient with no hemorrhage or exudate. Retinal vessel walls were stained with fluorescein