www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
anatomic
analysis
of
the
vidian
canal
and
the
surrounding
structures
concerning
vidian
neurectomy
using
computed
tomography
scans
夽
Gülay
Ac
¸ar
a,∗,
Aynur
Emine
C
¸ic
¸ekcibas
¸ı
a, ˙Ibrahim
C
¸ukurova
b,
Kemal
Emre
Özen
c,
Muzaffer
¸eker
S
a, ˙Ibrahim
Güler
daNecmettinErbakanUniversity,MeramFacultyofMedicine,DepartmentofAnatomy,Konya,Turkey
bHealthSciencesUniversity,IzmirTepecikTrainigandResearchHospital,DepartmentofOtolaryngology-HeadandNeckSurgery, Izmir,Turkey
cKatipC¸elebiUniversity,FacultyofMedicine,DepartmentofAnatomy,Izmir,Turkey dSelcukUniversity,FacultyofMedicine,DepartmentofRadiology,Konya,Turkey
Received15September2017;accepted8November2017 Availableonline26December2017
KEYWORDS Intrasphenoid septum; Morphometric analysis; Pterygoidprocess pneumatization; Vidiancanal; Vidianneurectomy Abstract
Introduction:Thetypeofendoscopicapproachchosenforvidianneurectomycanbespecified
byevaluatingthevidiancanalandthesurroundingsphenoidsinusstructures.
Objective:Thevariationsandmorphometryofthevidiancanalwereinvestigated,focusingon
thefunctionalcorrelationsbetweenthemwhicharecrucialanatomicallandmarksfor
preoper-ativeplanning.
Methods:This study was performed using paranasal multidetector computed tomography
imagesthatwereobtainedwithasectionthickeningof0.625mmof250adults.
Results:The distributionsof500vidian canalvariants werecategorized asfollows;Type 1,
withinthesphenoidcorpus(55.6%);Type2,partiallyprotrudingintothesphenoidsinus(34.8%);
Type3,withinthesphenoidsinus(9.6%).Thepneumatizationofthepterygoidprocessismostly
seeninvidiancanalType2(72.4%)andType3(95.8%)(p<0.001).Themeandistancesfromthe
vidiancanaltotheforamenrotundumandthepalatovaginalcanalweregreaterinthevidian
canalType2and3withthepterygoidprocesspneumatization(p<0.001).Theprevalenceofthe
intrasphenoidseptumbetweenthevidiancanalandthevomerinecrestandlateralattachment
whichendingoncarotidprominenceweremuchhigherinvidiancanalType3thanothertypes
(p<0.001).Themeananglebetweentheposteriorendofthemiddleturbinateandthelateral
marginoftheanterioropeningofthevidiancanalwasmeasuredas33.05±7.71◦.
夽 Pleasecitethisarticleas:Ac¸arG,C¸ic¸ekcibas¸ıAE,¸ukurova ˙I,C ÖzenKE,S¸ekerM,Güler ˙I.Theanatomicanalysisofthevidiancanaland
thesurroundingstructuresconcerningvidianneurectomyusingcomputedtomographyscans.BrazJOtorhinolaryngol.2019;85:136---43.
∗Correspondingauthor.
E-mail:[email protected](G.Ac¸ar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial. https://doi.org/10.1016/j.bjorl.2017.11.008
1808-8694/©2017Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
Conclusions: Preoperativeradiologicanalysis ofthevidian canal andthesurrounding
struc-tureswillallowsurgeonstochooseanappropriateendoscopicapproachtoensurepredictable
postoperativeoutcomes.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published
by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/). PALAVRAS-CHAVE Septointraesfenoidal; Análise morfométrica; Pneumatizac¸ãodo processopterigoide; Canalpterigoideo; Neurectomiado pterigoideo
Avaliac¸ãoanatômicadocanalvidianoeestruturasadjacentesportomografia computadorizadaparaaneurectomiadovidiano
Resumo
Introduc¸ão: Otipodeabordagemendoscópicaparaaneurectomiadovidianopodeserdefinido
pelaavaliac¸ãodocanaldovidianoedasestruturasadjacentesaosseiosesfenoidais.
Objetivo: Investigar as variac¸ões e a morfometria do canal vidiano com enfoque nas suas
correlac¸ões funcionais, pois são parâmetros anatômicos cruciaispara o planejamento
pré-operatório.
Método: Esseestudofoirealizadoutilizando-seimagensdetomografiacomputadorizada
multi-detectoresdosseiosparanasaiscomespessuradecortede0,625mmobtidasde250indivíduos
adultos.
Resultados: A distribuic¸ão das 500 variantes do canal vidiano foi categorizada daseguinte
forma:Tipo1,dentrodocorpoósseoesfenoidal(55,6%);Tipo2,protrusãoparcialnointeriordo
seioesfenoidal(34,8%);Tipo3,nointeriordoseioesfenoidal(9,6%).Apneumatizac¸ãodo
pro-cessopterigoidefoiobservadaprincipalmentenocanalvidianoTipo2(72,4%)eTipo3(95,8%)
(p<0,001).Asdistânciasmédiasdocanalvidianoatéoforameredondoeocanalpalatovaginal
forammaioresnocanalvidianodoTipo2e3,comapneumatizac¸ãodoprocessopterigoide
(p<0,001).Apresenc¸adoseptointraesfenoidalentreocanalvidianoeacristavomerianaea
extensãolateral,queterminanaproeminênciadacarótida,foimuitomaiornocanalvidiano
Tipo3doquenosoutrostipos(p<0,001).Aangulac¸ãomédiaentreacaudadaconchamédiae
amargemlateraldaaberturaanteriordocanalvidianofoide33,05◦±7,71◦.
Conclusões: Aanáliseradiológicapré-operatóriadocanaldovidianoedasestruturas
circun-jacentes permitem ao cirurgião escolher uma abordagem endoscópica apropriadae prever
resultadospós-operatórios.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado
por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
Thepterygopalatinefossa(PPF)lookslikeaninverse pyra-mid in a relatively deep inaccessible anatomical location that is formed by the perpendicular lamina of palatine bonemedially,greaterwingofsphenoidbonesuperiorly,the pterygoidprocessofsphenoidboneposteriorlyandmaxillary sinusanteriorly.1Thevariousosseouscommunicationsofthe
PPF formsrecognizableanatomical landmarkson Multide-tector Computed Tomography (MDCT) scans that describe themarginsandopeningsofthePPF.2Fromlateraltomedial
theforamenrotundum(FR),thevidiancanal(VC)whichis locatedinferomedialtoFRandthepalatovaginalcanal(PVC) areclinicallyimportantopeningsincludingcritical neurovas-cularstructuresintheposteriorwallofthePPF.Also,these foraminaareincloseassociationwiththesurrounding sphe-noidsinusstructures.1
Theendoscopicsurgerytoresectatumorthatlocalizes in or around the PPF and to cure the chronic vasomotor rhinitisisanalternativetotraditionalsurgicalapproachand minimizesmorbidityandthesizeoftheincision.3Currently,
endoscopictransnasalandtranssphenoidvidianneurectomy
are performed; the success rate of both approaches can beinfluencedbythedifferentsurroundingsphenoid struc-ture variations such as; VC protrusion into the sphenoid sinus,intrasphenoidseptum,thepterygoidprocess pneuma-tization (PPP) and the relationship of the VC with the middlenasalturbinate.4So,preoperativeradiological
eval-uation of the VC corpus types and surrounding sphenoid structuresguidesthesurgeoninchoosinganappropriate sur-gicalapproach,decreasingcomplicationsduringendoscopic surgery.5
Inthisstudy,weobservedVCvariationsandstudiedthe morphometricparametersoftheVCrelatedtothe surround-ing sphenoid structures. Specifically, we focused on the relationshipbetweenthemandanalyzedthefactorswhich affecttheformationofvariousVCcorpustypesrelatingto endoscopicapproaches.
Methods
The approval of thisretrospective investigation was done by our local Ethics Committee with an approval number 2016/543 and performed usingparanasal MDCT imagesof
Table1 Definitionsofvariationsofthevidiancanal and
thesurroundingstructures.
Variations Definitions
VCcorpustypes
Type1 Thevidiancanalwaslocatedwithin
sphenoidbonyroof
Type2 Thevidiancanalwaspartiallyprotruded
intosphenoidsinus
Type3 Thevidiancanalwastotallyprotrudedinto
sphenoidsinuswithastalk
Intrasphenoidseptumtypes
Vomerine crest-VC
Thesphenoidseptumbetweenthe
vomerinecrestandthevidiancanal
ICAS Thesphenoidseptumwhichdeviated
laterallyandattachedtothecarotid
prominence
OCS Thesphenoidseptumwhichdeviated
laterallyandattachedtotheopticcanal
Pterygoidprocesspneumatization
Existing Thesphenoidpneumatizationextendedinto
thepterygoidprocess
Not existing
Therewasnopneumatizationinthe
pterygoidprocess
VC-medialplateofthepterygoidprocessrelationship
Medial Thevidiancanalwaslocatedmediallyto
themedialplateofthepterygoidprocessor
onsameline
Lateral Thevidiancanalwaslocatedlaterallyto
themedialplateofthepterygoidprocess
Nasalseptumdeviation
Right Thenasalseptumdeviatingtoright
Left Thenasalseptumdeviatingtoleft
Absent Therewasnoseptumdeviation
250 patients who were referred to Department of Radi-ology from January 2016 to July 2016. All patients were evaluated using 128 slice MDCT scanner (Siemens, imag-ing parameters: kV, 120; mA, 160; rotation time, 0.5s; collimation,128×0.625;FOV,220mm).Multiplanar
recon-structionimages(associatedcoronalandsagittalimagesof 1mm slice thickness) were generated onthe basis of the axialimageswhichwereobtainedwithasectionthickening of0.625mm.AccordingtoapremadeprotocolonSyngoVia (Siemens,Germany)allscanswereanalyzed.The patients withapreviousparanasalsinussurgery,nasaltraumaor frac-tures,andparanasaltumorswereexcluded.
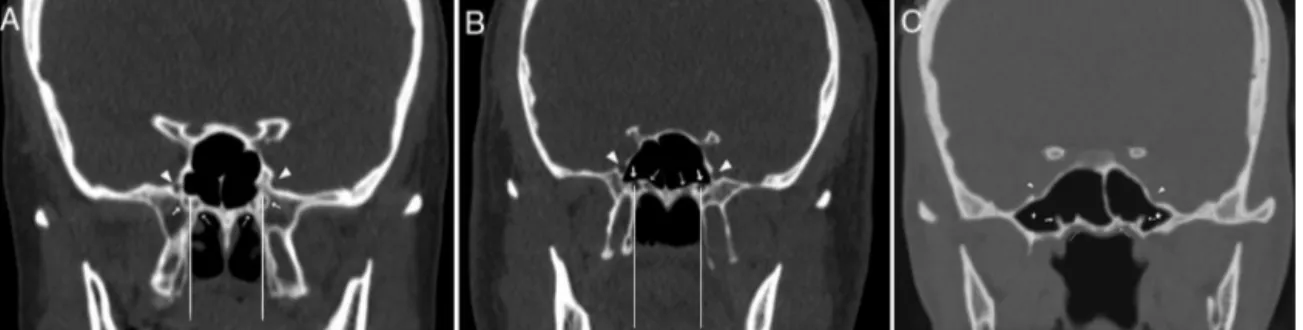
WeobservedthevariationsoftheVCcorpustypesandthe surroundingstructuresasshowninTable1.The VCcorpus typesaccordingtotherelationshipwiththesphenoidsinus werecategorizedintothreetypeswhicharebasedonYeh etal.’s4 classificationasfollows;Type1,withinthe
sphe-noidcorpus(Fig.1A);Type2,partiallyprotrudingintothe sphenoidsinus(Fig.1B);Type3,totallyprotrudingintothe sphenoidsinuswithastalk(Fig.1C).ThelocalizationofVC accordingtothemedialplateofthepterygoidprocess(MPP) wasdefinedasmedial(includingmedialandsameline)and lateral(Fig.1AandB). The sphenoidpneumatization pat-tern (Fig. 2A),the intrasphenoid septum between the VC andthevomerinecrest(Fig.1AandC)andlateral attach-mentsoftheseptumwhichendsonthecarotidprominence (ICAS)(Fig.2B)ortheopticcanal(OCS)wereanalyzed.Also, the presence of the PPP, which was defined asthe sphe-noid pneumatization extended into the pterygoid process wasobserved(Figs.1Cand3A).Thenasalseptumdeviation wasdeterminedastoright,toleftandnoseptumdeviation. AsseeninTable2,themorphometricparameters includ-ingthemeandiameterofthesphenopalatineforamen(SPF), thedistancesfromthevomerinecresttothePVCandVC, thedistancebetweentheFRandtheVCweremeasuredin coronalplane(Fig.3A).Topredictthefeasibilityofvidian neurectomy,wemeasuredthemeananglebetweenthe pos-teriorendofthemiddleturbinate(MTP)andlateralmargin oftheanterioropeningoftheVC(Fig.3BandC).Also,the lengthandthemeandiametersofthemiddlepart,anterior and posterior openings of the VC were measured in axial plane(Fig.3C).Inourstudy,afemalepatientwhowas 19-years-old hadnoleftFR(Fig.4A)andamalepatientwho was68-years-oldhadnorightFR(Fig.4B).
SPSS22(SPSS,Inc.,Chicago,IL,USA)wasusedfor statis-ticalanalysis.Forstatisticalcomparisons,Chi-squaretest, unpairedt-test,One-WayAnalysisofVariance(ANOVA)were usedandavalueofp<0.05wasconsideredsignificant.
Figure1 CoronalCTsectionsshowingthevidiancanal(thickarrow),palatovaginalcanal(thinarrow),foramenrotundum (arrow-head),pterygoidrecesspneumatization(star).(A)Bilateralvidiancanalsinsidethesphenoidcorpus(VCType1),therightvidian canallocatedlateraltomedialpterygoidplateandleftlocatedatsameline.(B)Thevidiancanalswhichpartiallyprotrudinginto thesphenoidsinus(VCType2)bilaterallylocatedatsamelinewiththemedialpterygoidplate.(C)Thevidiancanalswhichtotally insidethesphenoidsinuswithastalk(VCType3).
Figure2 (A)CoronalCTsectionshowingtheconchaltypesphenoidpneumatizationpattern(star);(B)AxialCTsectionshowing theintrasphenoidseptumwhichdeviatedandattachedonthecarotidprominence(ICAS)(thickarrow).
Results
Inthisstudy,thepatientsconsistedof107females(43%)and 143males(57%)withamedianageof45.76±17.64yearsfor femalesand40.80±16.47yearsformales.Threevariations of VC corpus anatomy according to the relationship with thesphenoidsinuswerefoundasfollows:Type1whichwas locatedwithin sphenoidbonyroof(55.6%,278/500), Type 2whichwaspartiallyprotrudedintosphenoidsinus(34.8%, 174/500),Type3whichwastotallyprotrudedintosphenoid sinuswithastalk(9.6%,48/500). Wedeterminedthatthe numberoftheintrasphenoidseptumwithsingleseptawas 197(78.8%),withmultipleseptawas45(18%),andwithout septawas8(3.2%).Thedistributionratiosofthesphenoid septumtypeswerefoundasfollows:intrasphenoidseptum betweenVCandthevomerinecrestas13.2%(66/500), lat-eralattachmentof theseptum whichendsonthe carotid prominence(ICAS)as28.4%(142/500)andontheopticcanal (OCS)as14.4%(72/500).Also,wefoundthepatternofthe sphenoidpneumatization asthesellar type(67%) and the prevalenceofthepresenceofthePPPas39.2%(196/500). The VC mostlylocated medialto theMPP (82%,410/500) andtheprevalencesoftheseptumdeviationwerefoundas toright34.4%(86/250),toleft25.2%(63/250),noseptum deviation40.4%(101/250).ThePVCwasidentifiedin372of the500computedtomography(CT)coronalsections(74.4%). TherelationshipoftheVCcorpustypeswiththesurrounding structuresvariationsisshown inTable3.The ratiosofthe presenceofthePPP,theICAS,theseptumbetweenVCand vomerinecrest weresignificantly higherin VCType2 and 3thanType1(p<0.001,p=0.03).Also,theconcurrenceof theICASandthePPPwasstatisticallysignificant(p<0.001), asseeninTable4.
We measured the meandiameters of themiddle part, anteriorandposterioropeningsoftheVCas1.0±0.4mm, 1.9±0.6mmand1.6±0.5mm,respectively.Also,themean length of the VC was found as 12.9±1.9mm. The mean distancesfromthevomerinecresttoVCandtoPVC were measuredas13.6±1.7mmand5.9±3.9mm,respectively. The meandistance betweenVC andFRwas8.1±2.3mm, andthe meandiameterof theSPFwas3.9±0.8mm. The meanvaluefortheanglebetweentheMTPandlateral mar-gin of the anterior opening of the VC was 33.05±7.71◦.
Table2 Definitionsofthemeasurements.
Measurements Definitions
VCdiameters
Anterior Theanterioropeningofthevidiancanalon
posteriorwallofthepterygopalatinefossa
Middle Themiddlepartofthevidiancanal
Posterior Theposterioropeningofthevidiancanalon
anteriormarginoftheforamenlacerum
VClength
(A---P)
Thedistancefromtheanteriortoposterior
openingsofthevidiancanal
VClocation
PVC-vomerine crest
Thedistancefromthepalatovaginalcanal
tothevomerinecrest
VC-vomerine crest
Thedistancefromthevidiancanaltothe
vomerinecrest
VC-FR Thedistancefromthevidiancanaltothe
foramenrotundum SPFdiameter Posterior tothe middle turbinate
Thediameterbetweentheperpendicular
plateofthepalatinebone(inferior)andthe
sphenoidbone(superior)
Endoscopicendonasalapproachangle
VC-MTP Angle
Theanglebetweentheposteriorendofthe
middleturbinateandthemostlateral
marginoftheanterioropeningofthevidian
canal
Tables5and6summarizethe relationshipofthe morpho-metricmeasurementswiththe VCvariations andthePPP. According to Tables 5 and 6 the VC Type 3 and the PPP alteredthe VC-FRandVC-PVCdistancesasincreased,but theoppositewastrueforthePVC-vomerinecrestdistance, the anterior and middle diameters of the VC that were smallerinVCType3andPPP(p<0.001).
Figure3 Morphometricmeasurements(A)CoronalCTsectionsshowingthedistancefromthevidiancanaltopalatovaginalcanal (blackdottedline)andtheforamenrotundum(whitedottedline),theseptum(thinarrow)betweenthevidiancanalandvomerine crest(thickarrow),thepterygoidprocesspneumatization(star).(B)AxialCTsectionshowingtheanglebetweentheposteriorend ofthemiddleturbinateandlateralmarginoftheanterioropeningofthevidiancanal,theanterioropeningofthevidiancanal (thickarrow)andtheposterioropeningofthevidiancanal(thinarrow).(C)CoronalCTsectionsshowingtheanglebetweenthe posteriorendofthemiddleturbinateandlateralmarginoftheanterioropeningofthevidiancanal.
Figure4 (A)CoronalCTimageof19-year-oldwomanshowingunilateralrightforamenrotundum(arrowhead,shehadnoleft foramenrotundum)andthevidiancanals(thickarrow);(B)coronalCTimageof68-year-oldmanshowingunilateralleftforamen rotundum(arrowhead,hehadnorightforamenrotundum)andthevidiancanals(thickarrow).
Table3 Therelationshipbetweenthevariationsofthevidiancanaltypesandthesurroundingstructures.
Thesurroundingstructurevariations VCtype p-Value
Type1N◦(%) Type2N◦(%) Type3N◦(%)
SSrelatedwithICA
Notexisting 223(80.2%) 105(60.3%) 30(62.5%) <0.001 Existing 55(19.8%) 69(39.7%) 18(37.5%) Pterygoidpneumatization Notexisting 254(91.4%) 48(27.6%) 2(4.2%) <0.001 Existing 24(8.6%) 126(72.4%) 46(95.8%) SSrelatedwithOC Notexisting 237(85.3%) 148(85.1%) 43(89.6%) 0.71 Existing 41(14.7%) 26(14.9%) 5(10.4%)
SSbetweenVCandVomerinecrest
Notexisting 251(90.3%) 145(83.3%) 38(79.2%) 0.03
Existing 27(9.7%) 29(16.7%) 10(20.8%)
VCrelationwithMPP
Medial 219(78.8%) 153(87.9%) 38(79.2%) 0.06
Lateral 59(21.2%) 21(12.1%) 10(20.8%)
VC,Vidiancanal;Type1,withinsphenoidcorpus;Type2,partiallyprotrudingintothesphenoidsinus;Type3,totallyprotrudingintothe sphenoidsinus;SS,sphenoidseptum;ICA,internalcarotidartery;OC,opticcanal;MPP,medialpterygoidplate.
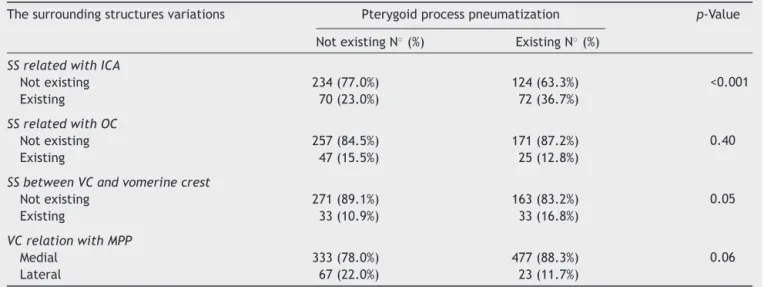
Table4 Therelationshipbetweenthepterygoidpneumatizationandthesurroundingstructuresvariations.
Thesurroundingstructuresvariations Pterygoidprocesspneumatization p-Value
NotexistingN◦(%) ExistingN◦(%)
SSrelatedwithICA
Notexisting 234(77.0%) 124(63.3%) <0.001
Existing 70(23.0%) 72(36.7%)
SSrelatedwithOC
Notexisting 257(84.5%) 171(87.2%) 0.40
Existing 47(15.5%) 25(12.8%)
SSbetweenVCandvomerinecrest
Notexisting 271(89.1%) 163(83.2%) 0.05
Existing 33(10.9%) 33(16.8%)
VCrelationwithMPP
Medial 333(78.0%) 477(88.3%) 0.06
Lateral 67(22.0%) 23(11.7%)
SS,sphenoidseptum;ICA,internalcarotidartery;OC,opticcanal;VC,vidiancanal;MPP,medialpterygoidplate.
Table5 Therelationshipbetweenthemorphometricmeasurementsandthevidiancanalcorpustypes.
Morphometricmeasurements Total VCtype p-Value
Type1 Type2 Type3
VCPdiameter(mm) 1.6±0.5 1.6±0.5 1.6±0.5 1.5±0.5 0.25
VCMdiameter(mm) 1.0±0.4 1.1±0.4 1.0±0.4 0.7±0.2 <0.001
VCAdiameter(mm) 1.9±0.6 2.0±0.5 1.9±0.6 1.5±0.6 <0.001
VClength(mm) 12.9±1.9 12.9±1.9 12.8±1.8 13.4±1.9 0.19
VC-MTPangle(◦) 33.05±7.71 33.15±7.86 32.58±7.76 34.14±6.57 0.44
PVC-vomerinecrestdistance(mm) 5.9±3.9 6.4±3.8 5.5±4.1 4.2±3.8 <0.001
VC-vomerinecrestdistance(mm) 13.6±1.7 13.5±1.6 13.4±1.7 14.8±1.4 <0.001
VC-FRdistance(mm) 8.1±2.3 7.1±2.1 9.3±2.0 9.8±2.2 <0.001
SPFdiameter(mm) 3.9±0.8 3.8±0.8 4.0±0.9 4.0±0.8 0.19
VC,vidiancanal;Type1,withinthesphenoidcorpus;Type2,partiallyprotrudingintothesphenoidsinus;Type3,totallyprotruding intothesphenoidsinus;VCP,posterioropeningofthevidiancanal;VCM,middlepartofthevidiancanal;VCA,anterioropeningof thevidiancanal;PVC,palatovaginalcanal;FR,foramenrotundum;SPF,sphenopalatineforamen;MTP,middleturbinateposteriorend. Mean±standarddeviation.
Table6 Therelationshipbetweenthemorphometricmeasurementsandthepterygoidprocesspneumatization.
Morphometricmeasurements Pterygoidprocesspneumatization p-Value
Notexist Exist
Mean±SD Mean±SD VCPdiameter(mm) 1.6±0.5 1.5±0.5 0.06 VCMdiameter(mm) 1.1±0.4 0.9±0.4 <0.001 VCAdiameter(mm) 2.0±0.6 1.7±0.6 <0.001 VClength(mm) 12.8±1.9 13.0±1.8 0.22 VC-MTPangle(◦) 33.21±7.80 32.79±7.58 0.54
PVC-vomerinecrestdistance(mm) 6.4±3.8 5.1±4.1 <0.001
VC-vomerinecrestdistance(mm) 13.5±1.6 13.7±1.8 0.39
VC-FRdistance(mm) 7.2±2.0 9.6±2.1 <0.001
SPFwidth(mm) 3.9±0.8 3.9±0.8 0.37
VCP,posterior opening ofthe vidiancanal; VCM,middle partof thevidian canal;VCA,anterior opening ofthevidian canal; VC, vidiancanal;PVC, palatovaginalcanal;FR,foramenrotundum;SPF,sphenopalatine foramen;MTP,middleturbinate posteriorend. Mean±standarddeviation.
Discussion
Since the surgical approach to the PPF is difficult, the intraoperativecomplicationssuchasexcessivebleedingand nerveinjurycanoccur. The vidiannerve,whichis formed bydeep(sympatheticfibers)andgreater(parasympathetic fibers) petrosal nerve, courses throughthe VC that is an importantlandmarkduringendoscopicaccesstothePPF.5
Especially,fortreatingtheresistantcasesofchronic vaso-motorrhinitis,thevidianneurectomyinterruptscholinergic innervationofthenasalmucosabyparasympatheticfibers.6
Inpreviousstudies, theendoscopicsurgicalapproaches to the VC were classified as transsphenoidal (Type I) that transectedthevidian nerveinside thesphenoidsinus and transnasal(Type II) thatis performed in theanteriorwall of the sphenoidsinus.7 Type I had its advantages shorter
operatingtime, less risk of injury and reduced bleeding. The patients withno intrasphenoid septum, theVC canal corpusType2and3,thepresenceofthePPP,thegreater distancebetweenVCandFRandtheVCnotinextreme lat-eralizedpositionweresuitableforTypeIapproach.Inother cases,TypeII approachwasmostlychosen.4,5The smaller
angle between the posterior end of the middle turbinate andthelateralmarginoftheanterioropeningoftheVC,no extremeseptumdeviation,thepresenceofthegapbetween thesphenoidprocessofthepalatineboneandthesphenoid bonejustmedialtotheVCsignificantlyincreasedthe suc-cessrateof TypeII approach.5---7 The VCcorpus typesand
thePPPwhichaffectsthemorphometricparametersshould beevaluatedonpreoperative CT scantoavoid iatrogenic injuryduringendoscopicsurgery.4
We observed the VCcorpus types andthe presence of the PPP with a correlation between them. The first aim of our study was to show the relationship of them with themorphometricmeasurementsandthevariationsofthe surroundingsphenoidstructures.Inpreviousstudies, Bidark-otimath et al., Yeh et al., Chen et al. and Cankal et al. reportedtheprevalenceoftheVCType1(withinthe sphe-noid corpus) as 67%, 50.8%, 55%, 54%; Type 2 (partially protrudingintothesphenoidsinus)as22%,39.8%,31%,36%; Type 3 (totally protruding into the sphenoid sinus with a stalk)as11%,9.4%,14%,10%,respectively.4,8---10Inthisstudy,
we classified theVC variants asType1, 55.6% (278/500); Type 2, 34.8% (174/500); Type 3, 9.6% (48/500). Conse-quently, the VC Type 3 constitutes a minority while the VCType 1 makes up half of the canals assimilar to pre-vious studies.The VC Type1that is embeddedinside the sphenoidcorpusinhibitsthevisualizationoftheVCinboth surgicalapproaches.Inthiscase,ifthereisnogapbetween thepterygoidprocessandthesphenoidprocessofthe pala-tinebone,one ofthemis partiallyremoved bytransnasal approach.5,7Ontheotherhand,theprevalenceofthePPP
wasdeterminedas39.2%(196/500),similartoprevious stud-iesresultsthatranged between19%and43.6%.4,11,12 Also,
wereportedthattheprevalenceofthePPPthatfacilitates theTypeIapproachweresignificantlyhigherin VCType2 (72.4%)andType3(95.8%)asshowninTable3(p<0.001).
Intheliterature,themostcommontypeof pneumatiza-tionofthesphenoidsinuswasfound asthesellartype.5,13
Wealsoobservedthepatternofthesphenoid pneumatiza-tionanddeterminedasthesellartype(67%).Thesellartype
pneumatizationfacilitatesalloftheendoscopicapproaches but, the conchal (nonpneumatized) sphenoid which was found as1%in ourstudy is arelativecontraindicationfor both types. The intrasphenoid septum is usuallydeviated andmostlyattachedtooneside(ICASorOCS).5
Fernandez-Miranda et al. reported that the prevalence of only one midlinesphenoidseptumwas87%andtheICASwas13%.14
WereportedthatthenumberoftheICASwas142(28.4%), theOCSwas72(14.4%)andtheseptumbetweentheVCand vomerinecrestwas66(13.2%).AccordingtoTables3and4, theprevalenceoftheICASandtheseptumbetweentheVC andvomerinecrestwerepositivelycorrelatedwiththeVC protrusionandthepresenceofthePPP(p<0.001),butthe prevalenceoftheOCSwasnotaffected.Inthisrespect,our studyisthefirstreportingthatthepresenceoftheICASand theintrasphenoid septumbetweenVC andvomerinecrest is associated withthe VCprotrusion andthe PPP. Specifi-cally,thepresenceoftheintrasphenoidseptumbetweenVC andvomerinecrestcaninhibitvisualizationduringsurgery. Removal of the septum is time-consuming and can cause skull base penetration and injury to the internal carotid arteryeventhoughtheVCprotrusionandPPPexist.4In
addi-tion,weanalyzedthattheVCismostlylocatedmedialtothe MPPandisnotaffectedbytheVCprotrusionandthePPPin
Tables3and4(p=0.06,p=0.16).Also,wefoundthatthere wasnorelationshipbetweentheseptumdeviationandother parameters.Themediallocationof theVCandnoseptum deviationfacilitatesthetransnasalapproach.
In the literature, the measured mean distances from vomerine crest to VC ranged between 12 and 16mm and to PVC ranged from 8 to 11mm, respectively.4,8,15 Also,
themeandistancesbetweenFRandVCweremeasuredas ranging between 4 and 8.5mm.3,4,8,15,16 In our study, we
measured the mean distance from vomerine crest to VC andtoPVCas13.6±1.7mmand5.9±3.9mm,respectively. The mean FR-VC distance was measured as8.1±2.3mm. AccordingtoTables5and6,theVCprotrusionalteredthe VC-FRandVC-PVCdistanceswhichwerelargerinVCType 2 and 3 (p<0.001). Also, these distances were affected asincreasedwiththepresenceofthePPP(p<0.001).Yeh et al., Hewaidi et al., Vescan et al. and Citardi et al. reported a positive correlation between the PPP and the VCprotrusionwhichincreasedthedistancebetweenVCand FRwassimilarwithourstudyresultsthatcanprovideagood surgicalguideinbothendoscopicapproaches.4,11,17,18
How-ever,thesmallerVC-FRandVC-PVCdistancesinVCType1 whichhadnoprotrusionintothesphenoidsinuscancause neurovascularcomplicationsthatshouldbekeptinmindby thesurgeons.Inaddition,thePPPusuallycausesprotrusion ofthesurroundingsphenoidstructuresintothesinus.4So,
duringtranssphenoidalsurgerythesurgeonshouldbecareful toavoidtheincreasedriskofneurovascularinjury.
Wereportedthatthemeasuredmeandiameters ofthe middle part, anterior and posterior openings of the VC were 1.0±0.4mm, 1.9±0.6mm and 1.6±0.5mm similar tothepreviousstudies,respectively.3,8,10Also,wefoundthe
meanlengthoftheVCas12.9±1.9mmwhileotherstudies reportedvaluesrangingfrom12.5to17mm.8,10Matoetal.
reportedthatduringthetransnasalapproach,theamountof bonydrillingontheinferomedialsurfaceoftheVCdepends on the length, protrusion of the VC and pneumatization
degree ofthepterygoidprocess.So,thesedatacanguide asafeproceduretotheanteriorgenuofthepetrousICA.19
ButinthisstudywefoundthatthelengthoftheVCandthe diameteroftheposterioropeningoftheVCwerenot statis-ticallyrelatedwiththetypeoftheVCandthedegreeofthe PPPasseeninTables 5and6.The meandiameters ofthe middlepartandanterioropeningoftheVCweresmallerin VCType3andtheVCwithPPP(p<0.001).
On theotherhand, theanterioropening oftheVCwas located above and 4---6mm posterolateral to the inferior margin of the SPF that is used in transnasal approach.20
Hwangetal.reportedthattheVC-SPFhorizontaldistance was positively, but the diameter of the SPF was nega-tivelycorrelatedwiththeVC-FRdistanceandmeasuredthe mean diameter of the SPF as5.3±1.3mm on the three-dimensionalreconstructionoftheCTscans.3Wemeasured
the mean diameter of the SPF as 3.9±0.8mm but, we reportedthatthe diameteroftheSPF wasnotcorrelated withtheVC-FRdistance,theVCcorpustypesandthePPP asseeninTable5and6(p=0.19,p=0.27).
The lateralmarginof theanterioropeningoftheVCis usuallylocated at thesuperolaterallevel of theposterior end of the middle turbinate; the smaller angle between themincreasesthesuccessrateoftheoperations.5Liuetal.
measuredtheaveragevalueofthatangleandcomparedto theoperatingsuccess rates.Theyreportedthat themean angle fromaxialand coronalCT imagingwere30.2±4.9◦ and26.4±9.1◦inthesuccessfulgroup,butthevalueswere 33.8±4.8◦and44.3±8.1◦inthefailedgroup,respectively.6
Inour study,we measured thisangle as33.05±7.71◦ and foundthattheanglevaluewasnotaffectedbytheVC pro-trusionandthePPPasshowninTables5and6.
This studyhassomelimitations. Unapparentmarginsof thePPFcomplicateselectionofsuitableplanesfor measure-ments.CTimagingmaynot representthetrue plane that iscompatiblewhenencounteredduringendoscopicsurgery. Recruitmentofthehighernumberofpatientsandpatients fromdifferentracesmaygiveresearchersmore comprehen-siveresults.
Conclusion
In this study, we examined the VC in all respects and reportedthattheICAS,theseptumbetweenthevidiancanal andthevomerinecrest,theVCcorpustypes,theVC-FRand theVC-PVCdistanceswereaffectedbythepresenceofthe PPPwhich play akey rolein endoscopicsurgery. But, we found thatthe presence ofthe PPPdidnot alterthe dis-tancefromthevomerinecresttotheVCandthelocationof theVCrelatedtoMPP.So,thePPPcanhaveaninfluenceon theconfigurationofthevidiancanalbutnotontheposition of it.Precise knowledgeof the radiologic anatomyof the pterygopalatine fossamaybeessential fordiagnosing vid-iannervepathologyandchoosinganappropriateendoscopic approachandsideofthesurgicalintervention.Asaresult, the surgical complications associated with an endoscopic vidianneurectomycanbedecreased.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.WilliamsPL,WarwickR,DysonM,BannisterLH.Gray’sanatomy. 37thed.Edinburgh:ChurchillLivingstone;1989.
2.DanielsDL,MarkLP,UlmerJL,MafeeMF,McDanielJ,ShahNC, etal.Osseousanatomyofthepterygopalatinefossa.AJNRAm JNeuroradiol.1998;19:1423---32.
3.HwangSH,JooYH,SeoJH,KimSW,ChoJH,KangJM. Three-dimensionalcomputedtomographyanalysistohelpdefinean endoscopicendonasalapproachofthepterygopalatinefossa. AmJRhinolAllergy.2011;25:346---50.
4.YehIK,WuIS.Computedtomographyevaluationofthesphenoid sinusandthevidiancanal.B-Ent.2013;9:117---21.
5.SuWF,WangHW, LiuSC.Endoscopicvidian neurectomy.The anatomyconsiderationandpreoperativeimagesanalysis.Intech OpenAccess.2012;5:85---105.
6.LiuSC,SuWF.Evaluationofthefeasibilityofthevidian neurec-tomyusingcomputedtomography.EurArchOtorhinolaryngol. 2011;268:995---8.
7.LiuSC,WangHW,KaoHL,HsiaoPC,SuWF.Three-dimensional boneCTreconstructionanatomyofthevidiancanal.Rhinology. 2013;51:306---14.
8.Bidarkotimath S, Viveka S, Udyavar A. Vidian canal radio-logical anatomy and functional correlations. JMorpholl Sci. 2012;29:27---31.
9.CankalF,HaholuA, Kilic¸C,TekdemirI.CTevaluationofthe vidiancanallocalization.ClinAnat.2007;20:751---4.
10.ChenJ,XiaoJ.Morphologicalstudyofthepterygoidcanalwith highresolutionCT.IntJClinExpMed.2015;8:9484---90. 11.CitardiMJ,Gallivan RP,BatraPS,MaurerCR, RohlfingT, Roh
HJ,etal.Quantitativecomputeraidedcomputedtomography analysisofsphenoidsinusanatomicalrelationships.AmJRhinol. 2004;18:173---8.
12.Kazkayasi M, Karadeniz Y, Arikan OK. Anatomic variations of the sphenoid sinus on computed tomography. Rhinology. 2005;43:109---14.
13.HamidO,ElFikyL,HassanO,KotbA,ElFikyS.Anatomic vari-ationsofthesphenoidsinusandtheirimpactontranssphenoid pituitarysurgery.SkullBase.2008;18:9---15.
14.Fernandez Miranda JC, Prevedello DM, Madhok R, MoreraV, Barges-Coll J, Reineman K, et al. Sphenoid septations and theirrelationshipwithinternalcarotidarteries.Anatomicaland radiologicalstudy.Laryngoscope.2009;119:1893---6.
15.KasemsiriP,SolaresCA,CarrauRL,ProsserJD,PrevedelloDM, OttoBA,etal.Endoscopicendonasaltranspterygoidapproaches Anatomicallandmarksforplanningthesurgicalcorridor. Laryn-goscope.2013;123:811---5.
16.Bryant L, Goodmurphy CW, Han JK. Endoscopic and three dimensionalradiographic imagingof thepterygopalatineand infratemporal fossa: improving surgical landmarks. Ann Otol RhinolLaryngol.2014;123:111---6.
17.HewaidiG,OmamiG.Anatomicvariationofsphenoidsinusand relatedstructuresinlibyanpopulation.CTscanstudy.LibyanJ Med.2008;3:128---33.
18.Vescan AD, Snyderman CH, Carrau RL, Mintz A, Gardner P, BranstetterBT,etal.Vidiancanalanalysisandrelationshipto theinternalcarotidartery.Laryngoscope.2007;117:1338---42. 19.Mato D,Yokota H, Hirono S, Martino J, SaekiN. The vidian
canalradiologicalfeaturesinJapanesepopulationandclinical implications.NeurolMedChir(Tokyo).2015;55:71---6.
20.Savard P,Stoney P,HawkeM.An anatomicalstudy ofvidian neurectomyusing anendoscopic technique.A potentialnew application.JOtolaryngol.1993;22:125---9.