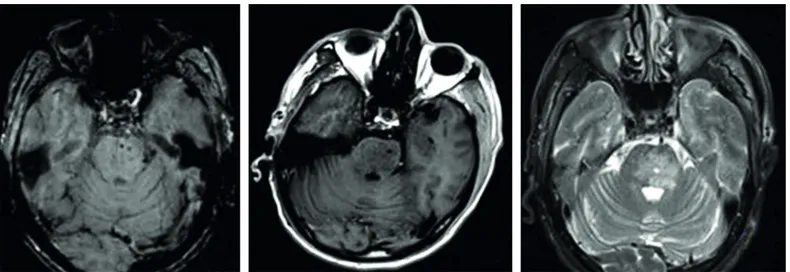
Traumatic isolated brain stem hematoma: a case report presenting with hemiparesis
Tam metin
Şekil
Benzer Belgeler
Isolated middle sacral artery rupture after blunt abdominal trauma in a pediatric patient.. Çocuk hastada künt abdominal travma sonrası izole orta sakral
We hereby present the use of 532 nm laser in treatment of premacular subhyaloid hemorrhage as a safe and effective alternative to Nd:YAG laser hyaloidotomy in a pregnant patient..
Bleeding findings related with hemophilia in the neonatal period may be in the form of blood leakage from the umbilical cord, hemorrhage in the scalp, extracranial
Ülkemizde aile hekimli¤i uygulamalar›n›n örgütlenmesi sürecinde her ortamda üzerinde en çok vurgu yapt›¤›m›z konu da aile hekimli¤i uzmanl›k e¤itiminin
yüksekliğini, tablonun dışında verilen sayılar ise o yönden bakıldığında daha yüksek apartmanların arkasında kalmayıp görülebilen apartman sayısını
The high temperature (~ 450 0 C) calcination is not the best way to remove the organic surfactant molecules, because the semiconductor Cd 1-x Zn x S nanoparticles oxidize in
Motivated by the recent results given in [ 15 , 20–25 , 29 ], in the present note, we establish here new Ostrowski type inequalities for s-convex functions in the second sense
Hazırlanan bu çalışmada stratejik yönetimin örgütlerde uygulanmasını etkileyen unsurlardan birisi olan örgüt kültürü üzerinde durulacak, "örgüt kültürü
