Aim: This study aimed to determine the sleeping habits and sleeping periods of kindergarten children, in order to analyze the problems related to sleep hygiene and determine the underlying factors. Methods: The sample size of this cross‑sectional study consisted of 390 children. A questionnaire filled in by the parents was used as the data collection tool. The data were analyzed with appropriate statistical tests. Results: According to the mothers, 77.2% of the children had their own room at home. Thirty nine percent of children slept with the full light on in their room, 50.3% slept with night light on in their room, 12.3% slept with the radio/television on in their room. Infant sleep practices found in this study are swaddling (18.5%), wrapping of the infant’s arms (21.0%), and rocking (58.7%). Conclusions: In terms of sleep hygiene, the vast majority of the children slept in a bright environment, and there were electronic appliances in the room. Common infant‑transition‑to‑sleep practices observed were wrapping their arms and swaddling them. In our point of view, awareness training for parents about the subject will support sleep hygiene practices.
Keywords: Child health, kindergarten, sleep hygiene
Sleep Habits and Related Factors in Kindergarten Children
Y Durduran, S Pekcan1, B Çolpan2
Address for correspondence: Dr. Y Durduran, Department of Public Health, Necmettin Erbakan University Meram Medical Faculty, 42080 Meram, Konya, Turkey. E‑mail: [email protected] bed for non‑sleep activities, bedtime behavior, sleep onset delay, and sleep duration, the child’s sleep may become much better and hygienic.[11‑13] Clinical and
public health studies are important when they are considered to be related to infant sleep and cognitive or behavioral development. Additionally, they may also be useful for early screening of sleep related problems, prevention, and early intervention studies.[14] Parents
have the responsibility for increasing the sleep quality of their children. To increase awareness of parents on sleep hygiene, more study in children are required. This study is aimed at determining the factors which affect sleeping habits, sleeping times, and evaluate the sleep hygiene problems of kindergarten children located in Konya centrum, Turkey.
Materials and Methods
The location of this cross‑sectional study was the centrum of Konya. The study was made in 2012 among
Introduction
S
leep problems are common in all childhood periods, from infancy to adolescence.[1,2] Therefore,understanding the development of sleeping habits is valuable for health professionals who are concerned with behavioral sleep problems in children.[3] Additionally, the
normal sleeping process in children should be known.[4]
From birth to the end of childhood, many parameters such as sleep duration, how long it takes the child to eventually fall asleep, the length of night‑time sleep, and the length of day‑time sleep vary.[5] In fact, sleep
habits and duration may vary between communities and geographical regions within the same country.[6,7] ‘‘Sleep
hygiene” defines comfortable, quality, and sufficient sleep. And sleep hygiene practices cover a number of domains, including the sleep environment, sleep routine, nap times and daytime activities, sufficient sleep duration, sleeping alone, before bedtime routine.[8‑10]
There are several regional studies on sleep hygiene and sleep habits in healthy children,[7,9] but not too many. If
sleep hygiene is provided well with simple suggestions including stimulant activities prior to bedtime, using
Departments of Public Health and 1Pediatric Pulmonary
Medicine, Necmettin Erbakan University, Meram Medical Faculty, 2Department of
Otorhinolaryngology, Head and Neck Surgery, Selçuk University, Medical Faculty, Konya, Turkey
Abstract
Access this article online Quick Response Code:
Website: www.njcponline.com
DOI: 10.4103/njcp.njcp_520_18 PMID: *******
Date of Acceptance:
06-May-2019
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: Durduran Y, Pekcan S, Çolpan B. Sleep habits and related factors in kindergarten children. Niger J Clin Pract 2019;22:1218-23.
the kindergarten children. Since the kindergartens in our country have 4‑‑5 age group children, the previous study[3] which had bed‑sharing rate of 38% in 4‑year‑old
children was considered in this study. G‑Power sample size calculation program[15] with a difference of 10%, the
sample size was calculated to be 195 with 0.80 power and at a 0.95 confidence level in our study. With the assumption that each classroom represented one cluster consisting of 20 children, in order to represent the society, the cluster effect was taken as 2 and it was planned to reach 390 children. As all of the parents could not fulfill the questionnaire, it was thought that 487 parents would be contacted with the expectation that the rate of acceptance and response would be about 80%. List of the schools was obtained from the Provincial Directorate of National Education and 15 kindergartens were visited through selection by the random sampling method. Local ethics committee approval was obtained (Decision number: 153) and institutional written permission was acquired from the National Education Directorate. There were 44 questions in the questionnaire which was prepared by the researchers after searching literature as data collection tool of this study. It was including sociodemographic information and about problems that would affect falling asleep and sleeping patterns. The independent variables of the study were the sex of the child, the number of children in the family, number of people living in the household, the age of the parents, their employment‑‑education status, the school type; dependent variables were the sleeping environment and sleeping habits of the kindergarten children. Following this, the schools were contacted, and in order to inform the parents, the teachers were informed about the purpose and content of the study. The teachers who agreed to participate in the study were asked to send the surveys to the parents. Only the teachers and parents who gave an informed consent were recruited into this study. The schools included in the study were visited once a week for 3 months. At the end of the study, the surveys that were received by the teachers were collected. The data were analyzed using SPSS program (SPSS for Windows, Version 16.0. Chicago, SPSS Inc.). The data were summarized with descriptive statistics appropriate to the distribution. Chi‑squared test was used to compare categorical data. Logistic regression analysis was used for multiple evaluations of variables which were significant in previous analyses. The limit value for significance was taken as P < 0.05.
Results
Demographic findings: Among the children of
390 mothers who participated in the survey, 58.5% were male, 41.5% were female. Mothers of 8 state
kindergartens and 7 special kindergartens stated that 73.3% of the children were in private kindergartens and 26.7% were in public kindergartens. The mean age of the mothers was 34.1 ± 5.1 years, and the mean number of person living in the house was 3.9 ± 0.9. Among the families, 32.2% had one child, 51.4% had two, and 16.4% had three or more children. The percentage of the employed mothers and fathers were 56.2% and 92.3%, respectively. 64.1% of the mothers and 67.7% of the fathers had college degrees.
Sleep environment and characteristics of falling asleep: In our study, 77.2% of the children had their
own rooms at home [Table 1]. Attending to private school was 4.01 times, mother’s high school or higher education graduate was 6.32 times effective on the child had their own room [Table 2]. Among the mothers who participated in the survey, 15.4% stated that before their children went to sleep, they made their children listen to music and 42.1% stated that they sang lullabies for their children. The mothers who played music for their children listed the music types they played. These were 38.6% lullabies, 22.8% classical music, 15.8% children’s songs, 12.3% Turkish classical music, 7.0% slow music, and 3.5% hymns. The rate of listening of
Table 1: Sleep Habits of Children (n, %)
Sleep-related issues n Percentage
Having his/her own room 301 77.2 Daytime sleep Determining his/her own bedtime 156 131 40.0 33.6 Before going to bed
Brushing teeth 265 67.9 Eating and drinking 254 65.1 Before falling asleep
Used to and still reading tales‑books 242 62.1 Playing music/singing a lullaby 224 57.5 Light and technological tools
Falling asleep, sleeping with light on 152 39.0 Turned on night/room light before sleeping
Sleeping with the night light on Radio in the room
Turning the radio on before sleeping
53 196 27 7 13.6 50.3 6.9 1.8 Television in the room 73 18.7 Turning the TV on before sleeping
Computer in the room Practices used for sleeping
Sleeping with a pacifier before and still Sleeping with a toy
Swaddling during infancy
Wrapping around the baby’s arms for sleeping Rocking baby to sleep
Swing or blanket swing
41 73 96 58 72 82 229 85 10.5 18.7 24.6 14.9 18.5 21.0 58.7 21.8
music was 3.26 times higher in mothers with two and more children (P < 0.001) [Table 2].
The mean age of the children was 2,4 ± 1.5 years when reading the book‑tale while the child was sleeping and 4.1 ± 1.6 years when the reading was stopped. 62.1% of the mothers read books to their children before they went to sleep. 51.0% of the mothers stated that they still read books for their children before sleeping. The fathers with high school or college degrees were 2.17 times effective on reading books or tales for putting their children to sleep [Table 2]. 13.6% of the mothers stated that their children preferred night lights or room lights to be on while sleeping, but the parents turned them off when they slept. The percentage of children slept with night light was 50.3% and accustomed to sleeping while the room light was on was 39.0%. 3.8% of the families stated that their children still slept with the pacifier and 20.8% said they were not using pacifiers any more [Table 1]. Considering the times of stopping to use pacifiers, 69.1% of the children stopped using pacifiers before the age of two, and this percentage increased to 91.0% with the age of 3. The rest of the children were not using pacifiers when they reached the ages of four or older. The toys the children were sleeping with were listed as baby‑plush dolls (29.3%), cars (27.6%), teddy bears‑‑cats (20.7%), pillows‑‑pillowcases‑‑blankets (13.8%), any toys (5.2%), and new toys (3.4%).
Sleep-related practices during infancy: The
percentage of the mothers stated that their children slept during breastfeeding in their infancy was 54.1%.
Swaddling: 18.5% of the mothers said they swaddled
their children for sleeping in infancy. 83.0% of the mothers who expressed swaddling their babies left the swaddle before the child reached the age of 1 year,
while the others continued to swaddle until 2 years of age. Wrapping: 21.0% of the mothers stated that they
wrapped their babies’ arms in order for them to sleep comfortably. 77.0% of the mothers wrapping around their babies’ arms quit doing so before the age of 1; 17.0% had just quit this practice when their babies were 2 years old and 6.0% continued until they were 3‑‑6 years old. Rocking: 58.7% of the mothers rocked
their children for sleeping, 22.7% continued rocking until the age of 1 year, 35.9% stopped this practice when their children were 2 years old, and 30.1% stopped this practice when their children were 3 years old. The percentage of the children who were not rocked to sleep anymore between the age of 3 and 6 was 11.3%. 21.8% of the mothers said they preferred swings or blanket swings for their children to sleep [Table 1], and the mean time for quitting this behavior was 1.8 ± 1.1 months. Table 3 presents the factors that were effective in these practices. Other practices: The
percentage of the children who woke up during night sleep was 76.4%. The mothers expressed that the main reasons for waking up at night were the need of going to the toilet and drinking milk/water (87.0%). During the infancy stage of their children, the percentage of the mothers who performed different practices when their children could not sleep was 69.0%. These practices were sleeping in the car, running the vacuum cleaner, tiring the baby through playing, rocking on the swing, and sleeping next to the baby.
Daytime sleep habits: 40.0% of the mothers said
their children were still falling asleep during the day [Table 1]. The mean daytime sleep duration was 0.4 ± 0.5 h. The mothers of the children—who used to sleep in the daytime but not now—stated the mean age for going on daytime sleeping as 1.5 ± 1.9 years and the mean duration of sleep in daytime used Table 2: Significant results in Multivariate Analysis with Sociodemographic Variables Related to Children’s Room
Presence and Sleeping Environment
Variables Risk Factors OR (95%CI)* P
Presence of the child’s own room Type of school (Private and Public School) 4.01 (2.12‑‑7.56) <0.001** Education status of the mother
(High school/College education graduates and others) 6.32 (3.10‑‑12.87) <0.001** Playing music before falling asleep Number of children in the family (single child and more
children) 3.26 (1.84‑‑5.78) <0.001** Reading books/tales for putting children to sleep Education level of the father (High School/College
Education graduates and others) 2.17 (1.02‑‑4.60) 0.04** Sleeping with night/room light on Age of the parents (Under 35 and over 35 years old) 0.56 (0.36‑‑0.86) 0.009**
Type of school (Private and Public School) 0.43 (0.26‑‑0.70) 0.001** Sleeping with television on Age of the parents (Under 35 years and over 35 years old) 0.38 (0.16‑‑0.91) 0.03**
Type of school (Private and Public School) 0.34 (1.17‑‑0.70) 0.004** *OR: Odds ratio and 95% confidence interval ** Significant results in multiple evaluations of chi‑squard test‑end meanings
to be 0.6 ± 1.1 h. Children who were private school students were significantly more likely to be sleeping in the daytime than those attending public schools (P = 0.02).
Sleep time--duration--position: The mean time of
going to bed was 21.4 ± 0.6 h during school days, 22.3 ± 1.3 h on the weekends, the mean duration of falling asleep was 16.9 ± 13.4 min, and 10.3% of the parents stated that they were sleeping at the same time with their children. The mean time of waking up was at 7.6 ± 0.6 o’clock during school days, 8.8 ± 1.0 o’clock on the weekends. The mean total sleep time was 10.1 ± 5.4 h. 27.9% of the mothers stated that their children were always sleeping on their back, and 27.9% were always sleeping on their sides [Figure 1]. Sleeping on the side was higher in girls than boys, and sleeping alone was higher in boys than girls [(P = 0.007, χ2 = 7.20) (P = 0.01, χ2 = 5.53)]. The mean age for
sleeping in his/her own bed alone was 1.3 ± 1.7 years. The rate of children who did not sleep alone in their bed was 52.8%. Of children, 7.9% were sleeping with their siblings and the sleeping place for the others varied. Getting accustomed to sleeping in their own bed before 3 years of age was higher in children studying in private schools than those in public schools, and it was higher
in children of mothers who have a job than mothers who have not a job (P = 0.008, P = 0.01).
Discussion
There are several studies showing sleep hygiene and sleeping habits differ among countries in the world.[16‑18]
However, there is not much information on children’s sleeping habits in Turkey. Besides, to our knowledge, this is the only study showing sleep profiles, patterns, and durations in kindergarten children in the Central Anatolia Region. Nearly half of the mothers in the study sang lullabies in order to put their babies to sleep. The number of the mothers who played music for their child before falling asleep was not high. Playing music before their babies go to sleep was prevalent in those with two or more children. This may be due to the fact that they tried this earlier in their families with more than one child, or because of the children’s will plausible reason may be the sound makes them assume mothers are around in the room and also offers soothing effect. Since causality was not tested in the study, this statement is limited only to the interpretations of the researchers. In our study, two‑thirds of the families used to read books or tales for their children before sleep, but unfortunately, it was still observed in only half of the families. The habit of parents to read books to their children may be an important part of the child’s future reading habits. This suggests that informing parents about the continuity of reading in the family may help children read books later. In the study, concerning sleep hygiene, while there were few children who had a night lamp turned on before sleeping but turned off after sleeping, the cases where the room light or night light was on was higher in total (89.3%). According to our data, this situation may be an indication that children did not sleep effectively. Because, a dark environment is more effective in terms of melatonin secretion (melatonin is produced by the pineal gland at night and strongly inhibited by light[19])
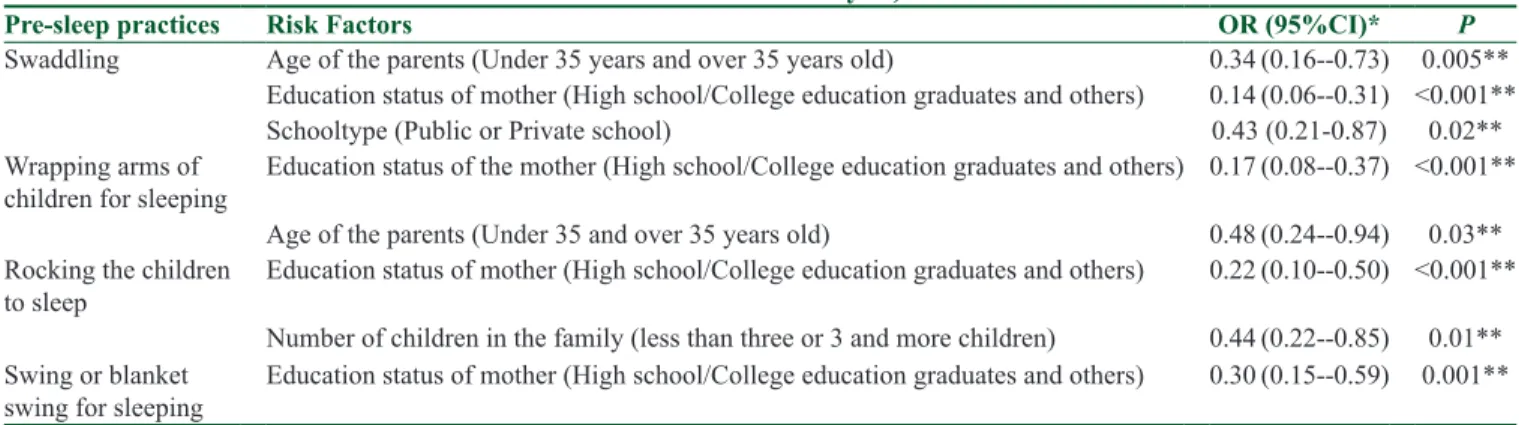
In the study, children with computers, television, or radio Table 3: Some sleep practices during infancy and relation to sociodemographic variables (Significant Results in
Multivariate Analysis)
Pre-sleep practices Risk Factors OR (95%CI)* P
Swaddling Age of the parents (Under 35 years and over 35 years old) 0.34 (0.16‑‑0.73) 0.005** Education status of mother (High school/College education graduates and others) 0.14 (0.06‑‑0.31) <0.001** Schooltype (Public or Private school) 0.43 (0.21‑0.87) 0.02** Wrapping arms of
children for sleeping Education status of the mother (High school/College education graduates and others) 0.17 (0.08‑‑0.37) <0.001** Age of the parents (Under 35 and over 35 years old) 0.48 (0.24‑‑0.94) 0.03** Rocking the children
to sleep Education status of mother (High school/College education graduates and others) 0.22 (0.10‑‑0.50) <0.001** Number of children in the family (less than three or 3 and more children) 0.44 (0.22‑‑0.85) 0.01** Swing or blanket
swing for sleeping Education status of mother (High school/College education graduates and others) 0.30 (0.15‑‑0.59) 0.001** *OR: Odds ratio and 95% confidence interval ** Significant results in multiple evaluations of Chi‑squaredtest‑end meanings
in the room were not rare at all. Even some of the children were still sleeping while the television was on. Similarly, there are another studies investigating the presence of electronic devices such as televisions in children’s rooms and their effects on sleep behaviors.[18,20]
In this study, there were few children who slept in their own rooms or in their bed. A study on the sleep environment and practices in Turkey found that 71.9% of the mothers who gave birth planned to share the same room with their infants, and 10% considered sleeping in the same bed with their infants for 0‑‑6 months.[21]
In another study, sleeping with each other in the same room was 80.8% among 5‑year‑olds.[7] Another study
reported that the habit of sharing the bed among children was closely related to cultural beliefs and practices.[22]
For example, while American parents generally expect their children to sleep alone, in the traditional population of Mayan families infants and toddlers sleep with their mothers and at the time or before the new baby is born, the toddler may be moved to sleep by sharing bed with father or in another bed in the same room.[23] The rate of
bed‑sharing in children in our study also it seems like a real cultural habits related in Turkey because half of the children do not sleep alone in their bed.
In our study, some of the children were sleeping with different kinds of toys and there were still a few children who were sleeping with a pacifier. Half of the mothers said their children used to sleep while breastfeeding in their infancy. Two of the most important sleep habits still practiced as a transition to sleep were the swaddle and wrapping around child’s arms. Also, especially singing lullabies and swaddling, covering and swinging were the common pre‑sleep rituals. This prevalence suggests that there may be a cultural effect in all these rituals. There is an interaction between biology and culture in sleep in childhood.[24] And, cultural characteristics such
as geographical, climatic, economic, regional, and historical features influence sleep initiation rituals and sleep time.[25] The mean total sleep time of the children
in our study was similar to the sleep time data in preschool in the studies by Hirhkowitz et al.,[26] and
Tso et al. found that pre‑school children in China were sleeping for 10 h and only 11% of them were sleeping for the recommended 11‑‑12 h.[27] Aishworiya et al.
found a nighttime sleeping time of 8.8 h for children of age 5‑‑6 years in Singapore;[7] this time it was lower
than our study. In order to be able to take care of sleep hygiene practices, it is important to identify the current situation, learn the truth information and to apply it. In our study, two‑thirds of the children were eating and drinking something and brushing their teeth before
bed. It was observed that most of the children woke up from sleep at night because of reasons such as toilet needs and drinking water‑‑milk. The most important sleep problem for this age was waking up from night sleep. In this study, almost half of the children still had daytime sleepiness, and this was higher in private school students. Daytime sleepiness is affected by day‑care, family routines, school activities, cultural differences, developmental expectations of families, and individual differences in the regulatory system.[25,28,29] We may
interpret from our study that sleep hygiene practices of the mothers who worked and had a high level of education were more regular. Wilson et al.[30] found in
the pre‑school age group that weekday bedtime was between 20:53 pm and 21:16 pm, waking was between 07:11 am and 07:26 am, and weekend bedtimes were between 21:35 pm and 21:52 pm, which was similar to our study. According to our study, the children’s weekend sleeping and waking hours could be different by about one‑and‑a‑half hours in bedtime on school days.
Good sleep hygiene should be encouraged for all children with sleep problems. In the article named the ABCs of Sleep by Allen et al.,[31] it was claimed that
consistent sleeping‑‑waking up times according to age, sleep schedule and routine, place of sleeping, pre‑sleep exercise and diet, the absence of electronic devices in the bedroom or before sleep, sleeping alone, and sleep routines are necessary for children to maintain a healthy sleep. In this study, we have seen in our society that these practices are not always carried out by families and children for a healthy sleep. The review reported that the general knowledge of parents on child sleep was poor; with small interventions, it was possible to increase parental knowledge in the short term, but this was not maintained in terms of effectiveness during follow‑ups.[32] For this reason, it may be worthwhile to
provide periodic trainings to families in relation to this subject.
Conclusion
Our study showed that the most important pre‑sleeping habit is sleeping with a pacifier, wrapping around the baby’s arms, and swaddling. Majority of the children slept in bright light and had electronic devices in their rooms. This may be an indication showing compliance problems with sleep hygiene in children and families. These results suggest that parents and their educational status play an important role in these habits and parental knowledge on sleep hygiene and quality of sleep was low in our study. Providing awareness training to parents about the subject can be valuable in acquiring accurate
information. We believe that every piece of information about sleep hygiene of children given by healthcare professionals, especially physicians, would support raising healthy generations. Additionally, since these characteristics may vary according to the regional habits and there may be different practices, we think there is a need for future work in Turkey involving all regions and a broader parent group.
Acknowledgements
The authors desire to thank all the participants in the study.
Financial support and sponsorship Nil.
Conflicts of interest
There are no conflicts of interest.
Edited by Glocal Translation.
References
1. Carter KA, Hathaway NE. Common sleep disorders in children. Am Fam Physician 2014;89:376‑7.
2. Owens JA. The practices of pediatrics sleep medicine: Results of a community survey. Pediatrics 2001;108:1‑16.
3. Jenni OG, Fuhrer HZ, Iglowstein I, Molinari L, Largo RH. A longitudinal study of bed sharing and sleep problems among Swiss children in the first 10 years of life. Pediatrics 2005;115:233‑40.
4. McLaughlin Crabtree V, Williams NA. Normal sleep in children and adolescents. Child adolesc Psychiatr Clin N Am 2009;18:799‑811.
5. Ward T, Mason TB 2nd. Sleep disorders in children. Nurs Clin North Am 2002;37:693‑706.
6. Liu X, Liu L, Owens JA, Kaplan DL. Sleep patterns and sleep problems among school children in the United States and China. Pediatrics 2005;115:241‑9.
7. Aishworiya R, Chan P, Kiing J, Chong SC, Laino AG, Tay SKH. Sleep behavior in a sample of preschool children in Singapore. Ann Acad Med Singapore 2012;41:99‑104.
8. Mindell JA, Meltzer LJ, Carskadon MA, Chervin RD. Developmental aspects of sleep hygiene: Findings from the 2004 National Sleep Foundation Sleep in America Poll. Sleep Med 2009;10:771‑9.
9. LeBourgeois MK, Giannotti F, Cortesi F, Wolfson AR, Harsh J. The relationship between reported sleep quality and sleep hygiene in Italian and American adolescents. Pediatrics 2005;115:257‑65. 10. Galland BC, Mitchell EA. Helping children sleep. Arch Dis
Child 2010;95:850‑3.
11. Ednick M, Cohen AP, McPhail GL. A review of the effects of sleep during the first year of life on cognitive, psychomotor, and temperament development. Sleep 2009;32:1449‑58.
12. Owens JA, Spirito A, McGuinn M. The children’s sleep habits questionnaire (CSHQ): Psychometric properties of a survey instrument for school‑aged children. Sleep 2000;23:1043‑51. 13. Gruber R, Cassoff J, Knäuper B. Sleep health education in
pediatric community settings: Rationale and practical suggestions
for incorporating healthy sleep education in to pediatric practice. Pediatr Clin North Am 2011;58:735‑54.
14. Halal CS, Nunes ML. Education in children’s sleep hygiene: Which approaches are effective? A systematic review. J Pediatr (Rio J) 2014;90:449‑56.
15. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for thesocial, behavioral, and biomedical sciences. Behav Res Methods 2007;39:175‑91. 16. Liu Z, Wang G, Geng L, Luo J, Li N, Owens J. Sleep patterns,
sleep disturbances, and associated factors among Chinese urban kindergarten children. Behav Sleep Med 2016;14:100‑17. 17. Sheares BJ, Kattan M, Leu CS, Lamm CI, Dorsey KB, Evans D.
Sleep problems in urban, minority, early‑school‑aged children more prevalent than previously recognized. Clin Pediatr (Phila) 2013;52:302‑9.
18. Garrison MM, Christakis DA. The impact of a healthy media use intervention on sleep in preschool children. Pediatrics 2012;130:492‑9.
19. Sack RL, Hughes RJ, Edgar DM, Lewy AJ. Sleep‑promoting effects of melatonin: At what dose, in whom, under what conditions, and by what mechanisms? Sleep 1997;20:908‑15. 20. Paavonen EJ, Pennonen M, Roine M, Valkonen S,
Lahikainen AR. TV exposure associated with sleep disturbances in 5‑ to 6‑year‑old children. J Sleep Res 2006;15:154‑61. 21. Efe E, Sarvan S, Kukulu K. Sleep practices and environment
and the risk of sudden infant death syndrome in Turkey. J Spec Pediatr Nurs 2007;12:253‑63.
22. Jain S, Romack R, Jain R. Bed sharing in school‑age children clinical and social implications. J Child Adolesc Psychiatr Nurs 2011;24:185‑9.
23. Morelli G, Rogoff B, Oppenheim D, Goldsmith D. Cultural variation in infants’ sleeping arrangements: Questions of independence. Dev Psychol 1992;28:604‑13.
24. Jenni OG, O’Connor BB, Children’s sleep: An inter play between culture and biology. Pediatrics 2005;115:204‑16.
25. Giannotti F, Cortesi F. Family and cultural influences on sleep development. Child Adolesc Psychiatr Clin N Am 2009;18:849‑61.
26. Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, Doncarlos L, et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015;1:40‑3.
27. Tso W, Rao N, Jiang F, Li AM, Lee SL, Ho FK, et al. Sleep duration and school readiness of Chinese preschool children. J Pediatr 2016;169:266‑71.
28. Ward TM, Gay C, Anders TF, Alkon A, Lee KA. Sleep and napping patterns in 3‑to‑5‑year old children attending full‑day child care centers. J Pediatr Psychol 2008;33:666‑72.
29. Whiteford L, Fleming P, Henderson AJ. Who should have a sleep study for sleep related breathing disorders? Arch Dis Child 2004;89:851‑5.
30. Wilson KE, Miller AL, Lumeng JC, Chervin RD. Sleep environments and sleep durations in a sample of low‑income preschool children. J Clin Sleep Med 2014;10:299‑305.
31. Allen SL, Howlett MD, Coulombe JA, Corkum PV. ABCs of sleeping: A review of the evidence behind pediatric sleep practice commendations. Sleep Med Rev 2016;29:1‑14.
32. McDowall PS, Galland BC, Campbell AJ, Elder DE. Parent knowledge of children’s sleep: A systematic review. Sleep Med Rev 2017;31:39‑47.