© Medical University of Bialystok, Poland
The analgesic and antiemetic efficacy of gabapentin
or ergotamine/caffeine for the treatment of postdural
puncture headache
Department of Anesthesiology and Reanimation, School of Medicine, Ufuk University, Ankara, Turkey
Erol DD
ABSTRACT
Purpose: We investigated the analgesic and antiemetic efficacy of gabapentin or ergotamine/caffeine (Cafergot), in addition to conservative treatment consisting of bed rest and adequate fluid intake, for the treatment of postdural puncture headache (PDPH).
Methods: In this randomized, prospective, controlled study, gabapentin or Cafergot was administered to 42 adult patients suffering from PDPH. Patients were asked to record the severity of their headache and the number of vomiting episodes on a visual analogue scale (VAS) on days 1, 2, 3 and 4. The pain scale consisted of a 10 cm horizontal line marked from 0 (denoting no pain) to 10 (denoting worst possible imaginable pain) Emesis was scored as 0 = no emetic symptoms, 1 = nausea or 2 = vomiting.
Results: Demographic and anesthetic variables were similar between the groups. Gabapentin group had less pain, nausea and vomiting compared to the Cafergot group. No patients withdrew, gabapentin and Cafergot were well tolerated, and adverse events (somnolence, dizziness, tremor, and ataxia) did not occur.
Conclusions: Gabapentin significantly reduced pain, nausea and vomiting compared to Cafergot in patients with PDPH. Lastly, we hypothesize that the gabaergic action of gabapentin, perhaps combined with other mechanisms, such as calcium channel blockade, may be responsible for its remarkable effects on PDPH.
Key words: Postdural puncture headache, emesis, gabapentin, ergotamine/caffeine, spinal anesthesia
* CORRESPONDING AUTHOR:
Department of Anesthesiology and Reanimation. School of Medicine Ufuk University
42.Cad. 455 Sok. No: 6/19 Dilay Sitesi. 06520 Çukurambar/ Ankara, Turkey.
Tel: 00 90 542 4308744; Fax: 00 90 312 2044033 E-mail: [email protected] (Demet Dogan Erol)
Received 30.03.2010 Accepted 16.12.2010 Advances in Medical Sciences Vol. 56(1)
·
2011·
pp 25-29 DOI: 10.2478/v10039-011-0009-z © Medical University of Bialystok, PolandINTRODUCTION
Postdural puncture headache (PDPH) continues to be a vexing problem for patients and anesthesiologists today. Supportive therapies, (such as bed rest and rehydration), acetaminophen (paracetamol), non-steroidal anti-inflammatory drugs, opioids and antiemetics may control the symptoms and so, reduce the need for more aggressive therapy, such as epidural blood patches, but do not provide complete relief [1-3].
Gabapentin is an antiepileptic drug that is also used for analgesia. It is a structural analogue of the neurotransmitter gamma-aminobutyric acid (GABA) but its exact mechanism of action is unknown. Gabapentin has been reported to be effective in treatment of PDPH [4,5].
We investigated the analgesic and antiemetic efficacy of either gabapentin or Cafergot (ergotamine/caffeine), in addition to conservative treatment consisting of bed rest and adequate fluid intake, for the treatment of PDPH.
MATERIAL AND METHODS
Following an approval from the ethics committee of the School of Medicine, Kocatepe University, informed consent was obtained from each patient. Forty-two adult patients who developed PDPH after spinal or epidural anesthesia were enrolled in the study. Exclusion criteria were: known allergy to, or contraindications (pancreatitis, galactosemia) to the use of gabapentin or Cafergot, other medication use (postoperative
analgesics, phenytoin, carbamazepine, valproic acid, phenobarbital, naproxen, hydrocodone, morphine, cimetidine, oral contraceptive, antacid, probenecid), migraine, asthma, coronary artery disease, and hepatic or renal insufficiency. Patients were treated in the Kocatepe University Hospital. For diagnosis we used the criteria suggested by the International Headache Society (IHS).
Diagnostic criteria
A. Headache that worsens within 15 minutes after sitting or standing and improves within 15 minutes after lying, with at least one of the following and fulfilling criteria C and D: 1. neck stiffness
2. tinnitus 3. hypacusia 4. photophobia 5. nausea
B. Dural puncture has been performed
C. Headache develops within 5 days after dural puncture D. Headache resolves either:
1. Spontaneously within 1 week
2. Within 48 hours after effective treatment of the spinal fluid leak (usually by epidural blood patch)
After being diagnosed with PDPH, all patients were treated with bed rest and fluid hydration (3000cc/24h) for 4 days. During the 4 days we also administered gabapentin/ Cafergot treatment.
Patients with PDPH were randomized to receive either oral gabapentin (Neurontin; Pfizer) 300 mg three times a day (Group G; n = 21) or oral Cafergot (Novartis), which contains 1 mg of ergotamine and 100 mg of caffeine, three times a day for 4 days (Group C; n = 21).
Postural headache has been defined by certain criteria as the headache occurring after a dural puncture and one that has a significant effect on the patients’ post operative well being i.e. headache, that is not only postural, but also continues for more than 24 hours at any level of intensity or so severe at any time that the patient is unable to maintain an upright position.
Patients were asked to record the severity of their headache in an upright position on a visual analogue scale (VAS) and the number of vomiting episodes on days 1, 2, 3 and 4. The pain scale consisted of a 10 cm horizontal line marked from 0
(denoting no pain) to 10 (denoting worst possible imaginable pain) and scores were made when the patient was supine. Emesis was scored as 0 = no emetic symptoms, 1 = nausea or 2 = vomiting. Pain, nausea and vomiting scores, spinal or epidural anesthesia, needle size and attempts of punctures were recorded. Side-effects − such as somnolence, ataxia, light-headedness, dizziness or visual disturbances − were determined by asking the patient.
Statistical evaluations were made using SPSS for Windows (SPSS 14.0 for Windows). Descriptive statistics were used for the means of the demographic variables and anesthetic data; comparisons of the 2 parallel groups were performed using analysis of variance (unpaired-sample t-test); significance was set at p < 0.05.
RESULTS
From October 1, 2003 to December 1, 2009, 42 consecutive patients who fulfilled the inclusion criteria were included in the study. Demographic characteristics regarding age, gender, weight, height and anesthetic data were similar between the groups (Tab. 1).The mean systolic and diastolic blood pressure, mean heart rate were not different between the two groups in any of the measured times.
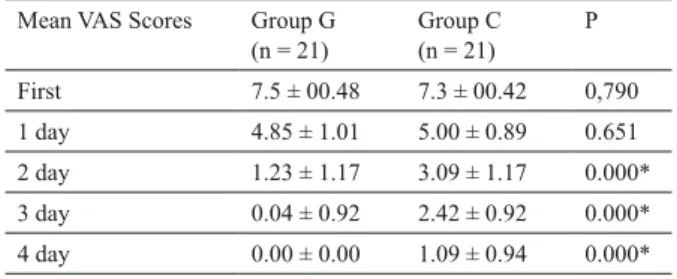
The visual analogue scale scores on days 2, 3 and 4, and the emesis scores on days 3 and 4 were significantly low (P < 0.05) in the gabapentin group when compared with the Cafergot group (Tab. 2; Tab. 3).
No patients withdrew; gabapentin and Cafergot were well tolerated; no adverse events (such as somnolence, dizziness, tremor or ataxia) were reported.
DISCUSSION
Carrie and Collins [6] define PDPH as “a headache occurring after dural puncture and which has a significant effect on the patients’ post operative well being i.e. headache which is not only postural but also continues for more than 24 hours at any level of intensity or so severe at any time that the patient is unable to maintain upright position”. Symptoms include nausea, vomiting, hearing loss, diplopia, tinnitus, vertigo, dizziness, paraesthesia of the scalp, and upper and lower limb
*Values are means ± SD.
P > 0.05 indicates no statistically significant difference. Group G (n = 21) Group C (n = 21) P Age (y) 45 47 0.605 Gender (m/f) 12/9 13/8 0.748 Weight (kg)* 76.14 ± 13.48 74.09 ± 13.69 0.639 Spi/Epi 20/1 21/0 0.329 Needle size* 22.19 ± 0.87 22.28 ± 1.30 0.789 Attempts of punctures* 1.19 ± 0.40 1.47 ± 0.74 0.162
Table 1. Demographic characteristics and anesthetic data.
Mean VAS Scores Group G (n = 21) Group C (n = 21) P First 7.5 ± 00.48 7.3 ± 00.42 0,790 1 day 4.85 ± 1.01 5.00 ± 0.89 0.651 2 day 1.23 ± 1.17 3.09 ± 1.17 0.000* 3 day 0.04 ± 0.92 2.42 ± 0.92 0.000* 4 day 0.00 ± 0.00 1.09 ± 0.94 0.000*
Table 2. Mean VAS Scores.
Values are means ± SD.
pain [7-9]. There is a potential for considerable morbidity [10,11]. In some patients, the headache lasts for months or years. Visual disturbances such as diplopia or cortical blindness have been reported [12]. Neurological symptoms may precede the onset of grand mal seizures. Intracranial subdural haematomas, cerebral herniation and death have been described as consequences of dural puncture [10].
The headache is described as severe, ‘searing and spreading like hot metal’ by our patients. The common distribution is over the frontal and occipital areas radiating to the neck and shoulders. The temporal, vertex and nuchal areas are reported less commonly as the site of discomfort, although neck stiffness may be present. The pain is exacerbated by head movement, and adoption of the upright posture, and relieved by lying down. An increase in the severity of the headache on standing is the sine qua non of postdural puncture headache. Other symptoms associated with dural puncture headache include nausea and vomiting. The severity of PDPH can render the patient bedridden and unable to eat, drink, or carry out activities of daily living.
Postdural puncture headache is currently diagnosed using varying sets of clinical criteria in anesthesia studies. These include study-specific as well as formal criteria set out by the IHS [13]. According to the IHS Headache Classification Committee, headache after lumbar puncture is defined as “bilateral headaches that develop within 7 days after an lumbar puncture and disappears within 14 days. The headache worsens within 15 min of resuming the upright position, disappears or improves within 30 min of resuming the recumbent position”. This definition helps to avoid confusion with migraine or simple headache after lumbar puncture. For diagnosis we used the criteria suggested by the HIS [13].
Symptoms are believed to be the result of the loss of cerebrospinal fluid (CSF) from the intrathecal space, which causes a cerebral vasodilatation, an increased arteriovenous pressure gradient, dural traction and compression of the cranial contents resulting from the loss of the cranial fluid cushion. Current management of PDPH aims to increase CSF production, reduce the arteriovenous pressure gradient using cerebral vasoconstriction, or decrease CSF loss by tamponade at the dural puncture site [14-16].
In our study, some patients suffering from PDPH received spinal anesthesia in other hospitals, and we were unable to
compare anesthesia procedures. Generally, the patients were referred our hospital 2 days after dural puncture. Obstetric patients were included in the study, but generally they were outpatients. The obstetric patient is at a particular risk of dural puncture (and the subsequent headache) because of sex, young age, and the widespread application of regional anesthesia [17]. All patients received bed rest and fluid hydration, VAS score of about 5 means the severity of PDPH. No patient received an epidural blood patch. The recommended dose of gabapentin in severe headaches (such as migraine) is 900 mg/day. So we justify this dose in the treatment of PDPH. As the advised dose of caffeine combined with ergotamine is 1 mg of ergotamine and 100 mg of caffeine three times a day all patients were administered this standard dose.
Camann et al. [18] observed that 300 mg oral caffeine is superior to placebo for the relief of PDPH. Caffeine is a central nervous system stimulant, that among other effects, causes cerebral vasoconstriction. It is assumed that caffeine acts on dilated cerebral vessels. The effects of caffeine on PDPH seem, at best, temporary [19]. In addition, caffeine is not a therapy without complications - therapeutic doses have been associated with central nervous system toxicity and atrial fibrillation and it does not restore normal CSF dynamics, thus leaving the patient at a risk of serious complications associated with low CSF pressure [20]. Caffeine therapy is simple to administer compared with the technical skills required to perform an epidural blood patch procedure, which is considered the ″gold standard” of treatment but is invasive [21].
Ergotamine is an alpha-adrenergic blocking agent with a direct stimulating effect on the smooth muscle of peripheral and cranial blood vessels and depresses the central vasomotor centers. Its properties also include serotonin antagonism. In comparison with the effects of dehydrogenated ergotamine, the adrenergic blocking actions of ergotamine tartrate are less pronounced and its vasoconstrictive actions are greater. The addition of caffeine to ergotamine tartrate facilitates the absorption of ergotamine when administered orally or rectally, resulting in a more rapid onset of the vasoconstrictive effect and an increase in the effectiveness [22].
Gabapentin is an antiepileptic drug and a structural analogue of GABA. Despite its structural similarity to GABA, it doesnot act via GABA receptors [23]. Though its exact mechanismof action is not known, its presumed mechanisms are: theability to increase the concentration and the rate of synthesisof GABA in the brain; theability to bind with high affinity to the binding sitesin the brain tissues that are associated with an auxiliary subunitof voltage sensitive calcium channels (α2δ subunit); theability to reduce the release of monoamine neurotransmitters; theability to inhibit voltage activatedsodium channels; and theability to increase serotonin concentrations in humanblood [24,25].
Numerous laboratory studies have described theanalgesic effects of different anticonvulsant drugs. Recent clinical trials haveshown that anticonvulsants may reduce spontaneous and movement-evoked pain and decrease opioid requirements
Table 3. Emesis Scores.
Mean VAS Scores Group G (n = 21) Group C (n = 21) P First 2.5 ± 00.42 2.8 ± 00.43 0.860 1 day 0.85 ± 1.23 0.90 ± 0.99 0.883 2 day 0.14 ± 0.35 0.42 ± 0.14 0.137 3 day 0.00 ± 00.00 0.28 ± 00.46 0.010* 4 day 0.00 ± 00.00 0.04 ± 00.21 0.029* Values are means ± SD.
postoperatively. In a review of 16 studies, Ho et al. [26] concludedthat a single preoperative dose of gabapentin (1200 mg or less)reduced pain intensity, opioid consumption and opioid-relatedadverse effects such as vomiting and pruritus for the first24 h postoperatively.
Pharmacological effects of anticonvulsant drugs that may beimportant in the modulation of the postoperative neural changesinclude suppression of the sodium channel, calcium channel and glutamatereceptor activity at peripheral, spinal and supraspinal sites [26]. Gabapentin and pregabalin have antiallodynic and antihyperalgesic properties useful for treating neuropathic pain. Gabapentinoids effectively reduce postoperativepain, opioid consumption, and opioid related adverse effectsafter surgery [27]. Gabapentin is also effective in diabetic neuropathy, neuropathic cancer pain, postherpetic neuralgia and inflammatory injury [28 - 32]. In the study by Agarwal et al. [33], gabapentin (600 mg) administered orally 1 h beforesurgery reduced the incidence and severity of catheter-related bladder discomfort (CRBD), postoperativepain, the number of patients requiring fentanyl, and postoperativetotal fentanyl requirements. Recently an open clinical study demonstrated the antiemetic effect of gabapentin in chemotherapy induced acute (within 24 h) and delayed onset (days 2-5) of nausea and vomiting in breast cancer [34]. Gabapentin has been reported to be effective in the treatment of emesis in patients undergoing laparoscopic cholecystectomy [35].
Gabapentin has been reported to be effective in the treatment of PDPH [4,5], possibly through its GABAergic actions, combined with other mechanisms such as calcium channel blockade. In our study, gabapentin was more effective in reducing the overall incidence of headache and vomiting compared to Cafergot in patients with PDPH.
Lastly, we hypothesize that the GABAergicaction of gabapentin, perhaps combined with other mechanisms,such as calcium channel blockade, may be responsible for its remarkable effects on PDPH.
ACKNOWLEDGEMENTS
The author thanks the residents, nurses and staff of the Kocatepe University Hospital for their multiple contributions.
REFERENCES
Spriggs DA, Burn DJ, French J, Cartlidge NE, 1.
Bates D. Is bed rest useful after diagnostic lumbar puncture? Postgrad Med J. 1992 Jul;68(801):581-3.
Ostheimer GW, Palahniuk RJ, Shnider SM. Letter: 2.
Epidural blood patch for post-lumbar-puncture headache. Anesthesiology. 1974 Sep;41(3):307-8.
Flaatten H, Rodt S, Rosland J, Vamnes J. 3.
Postoperative headache in young patients after spinal anaesthesia. Anaesthesia. 1987 Feb;42(2):202-5.
Erol DD. The effect of oral gabapentin on postdural 4.
puncture headache. Acute Pain. 2006;8(4):169-73.
Lin YT, Sheen MJ, Huang ST, Horng HC, Cherng 5.
CH, Wong CS, Hot ST. Gabapentin relieves post-dural puncture headache - a report of two cases. Acta Anaesthesiol Taiwan. 2007 Mar;45(1):47-51.
Carrie LE, Collins PD. 29-gauge spinal needles. Br 6.
J Anesth. 1991 Jan;66(1):145-6.
Lybecker H, Andersen T. Repetitive hearing loss 7.
following dural puncture treated with autologous epidural blood patch. Acta Anaesthesiol Scand. 1995 Oct;39(7):987-9.
Nishio I, Williams BA, Williams JP. Diplopia: 8.
a complication of dural puncture. Anesthesiology. 2004 Jan;100(1):158-64.
Schabel JE, Wang ED, Glass PS. Arm pain as 9.
an unusual presentation of postdural puncture intracranial hypotension. Anesth Analg. 2000 Oct;91(4):910-2.
Eerola M, Kaukinen L, Kaukinen S. Fatal brain 10.
lesion following spinal anaesthesia. Report of a case. Acta Anaesthesiol Scand. 1981 Apr;25(2):115-6.
Reynolds F. Dural puncture and headache. BMJ. 11.
1993 Apr 3;306(6882):874-6.
Vandam LD, Dripps RD. Long-term follow-12.
up of patients who received 10,098 spinal anesthetics; syndrome of decreased intracranial pressure (headache and ocular and auditory difficulties). J Am Med Assoc.1956 Jun 16;161(7):586-91.
Headache Classification Subcommittee of the 13.
International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004;24 Suppl 1:9-160.
Weeks SK. Spinal headache-prevention and 14.
treatment. Can J Anaesth. 1990 May;37(4 Pt 2):Sliii-Sixiii. Reid JA, Thorburn J. Headache after spinal 15.
anaesthesia. Br J Anaest. 1991 Dec;67(6):674-7.
Raskin NH. Lumbar puncture headache: a review. 16.
Headache. 1990 Mar;30(4):197-200.
Kuczkowski KM. Post-dural puncture headache in 17.
the obstetric patient: an old problem. New solutions. Minerva Anestesiol. 2004 Dec;70(12):823-30.
Camann WR, Murray RS, Mushlin P S, Lambert D 18.
H. Effects of oral caffeine on postdural puncture headache. A double-blind, placebo-controlled trial. Anesth Analg. 1990 Feb;70(2):181-4.
Bolton VE, Leicht CH, Scanlon TS. Postpartum 19.
seizure after epidural blood patch and intravenous caffeine sodium benzoate. Anesthesiology. 1989 Jan;70(1):146-9.
Jarvis AP, Greenawalt JW, Fagraeus L. Intravenous 20.
caffeine for postdural puncture headache. Anesth Analg. 1986;65(3):316-7.
Scavone BM, Wong CA, Sullivan JT, Yaghmour E, 21.
Sherwani SS, McCarthy RJ. Efficacy of a prophylactic epidural blood patch in preventing post dural puncture headache in parturients after inadvertent dural puncture. Anesthesiology. 2004 Dec;101(6):1422-7.
Silberstein SD, Young WB.
22. Safety and efficacy of
ergotamine tartrate and dihydroergotamine in the treatment of migraine and status migrainosus. Working Panel of the Headache and Facial Pain Section of the American Academy of Neurology. Neurology. 1995 Mar;45(3 Pt 1):577-84.
Goa KL, Sorkin EM. Gabapentin. A review of its 23.
pharmacological properties and clinical potential in epilepsy. Drugs. 1993 Sep;46(3):409-27.
Patel S, Naeem S, Kesingland A, Froestl W, Capogna 24.
M, Urban L, Fox A. The effects of GABA(B) agonists and gabapentin on mechanical hyperalgesia in models of neuropathic and inflammatory pain in the rat. Pain. 2001 Feb 15;90(3):217–26.
Gee NS, Brown JP, Dissanayake VU, Offord J, 25.
Thurlow R, Woodruff GN. The novel anticonvulsant drug, gabapentin (Neurontin), binds to the alfa2delta subunit of a calcium channel. J Biol Chem. 1996 Mar 8;271(10):5768-76.
Gilron I.
26. Review article: the role of anticonvulsant drugs in postoperative pain management: a bench-to-bedside perspective. Can J Anaesth. 2006 Jun;53(6):562-71.
Tiippana EM, Hamunen K, Kontinen VK, Kalso E. 27.
Do surgical patients benefit from perioperative gabapentin/ pregabalin? A systematic review of efficacy and safety. Anesth Analg. 2007 Jun;104(6):1545-56.
Mao J, Chen LL. Gabapentin in pain management. 28.
Anesth Analg. 2000 Sep;91(3):680-7. Backonja
29. M, Beydoun A, Edwards KR, Schwartz
SL, Fonseca V, Hes M, LaMoreaux L, Garofalo E. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: a randomized controlled trial. JAMA. 1998 Dec 2;280(21):1831-6.
Rowbotham M, Harden N, Stacey B, Bernstein P, 30.
Magnus-Miller L. Gabapentin for the treatment of postherpetic neuralgia: a randomized controlled trial. JAMA. 1998 Dec 2;280(21):1837-42.
Caraceni A, Zecca E, Martini C, De Conno F. 31.
Gabapentin as an adjunct to opioid analgesia for neuropathic cancer pain. J Pain Symptom Manage. 1999 Jun;17(6):441-5.
Ho KY, Gan TJ, Habib AS. Gabapentin and 32.
postoperative pain--a systematic review of randomized controlled trials. Pain. 2006 Dec 15;126(1-3):91-101.
Agarwal A, Dhiraaj S, Pawar S, Kapoor R, Gupta 33.
D, Singh PK. An evaluation of the efficacy of gabapentin for prevention of catheter-related bladder discomfort: A prospective, randomized, placebo-controlled, double-blind study. Anesth Analg. 2007 Nov;105(5):1454-7.
Guttuso T Jr, Roscoe J, Griggs J. Effect of gabapentin 34.
on nausea induced by chemotherapy in patients with breast cancer. Lancet. 2003 May 17;361(9370):1703-5.
Pandey CK, Priye S, Ambesh SP, Singh S, Singh 35.
U, Singh PK. Prophylactic gabapentin for prevention of postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy: a randomized, double-blind, placebo-controlled study. J Postgrad Med. 2006 Apr-Jun;52(2):97-100.