CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports15(2015)103–106
ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
j o u r n al ho m e p a g e :w w w . c a s e r e p o r t s . c o m
Tarsal
tunnel
syndrome
masked
by
painful
diabetic
polyneuropathy
Tugrul
Ormeci
a,∗,
Mahir
Mahirogulları
b,
Fikret
Aysal
caMedipolUniversity,FacultyofMedicine,DepartmentofRadiology, ˙Istanbul,Turkey
bMedipolUniversity,FacultyofMedicine,DepartmentofOrthopedicsandTraumatology, ˙Istanbul,Turkey cMedipolUniversity,FacultyofMedicine,DepartmentofNeurology, ˙Istanbul,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received3July2015
Receivedinrevisedform5August2015 Accepted21August2015
Availableonline28August2015 Keywords:
Tarsaltunnelsyndrome Diabeticpolyneuropathy Pain
Magneticresonance Superficialultrasound
a
b
s
t
r
a
c
t
INTRODUCTION:Variouscausesinfluencetheetiologyoftarsaltunnelsyndromeincludingsystemic
diseaseswithprogressiveneuropathy,suchasdiabetes.
PRESENTATIONOFCASE:Wedescribea52-year-oldmalepatientwithcomplaintsofnumbness,burning
sensationandpaininbothfeet.Thelaboratoryresultsshowedthatthepatienthaduncontrolleddiabetes,
andtheEMGshoweddistalsymmetricalsensory-motorneuropathyandnerveentrapmentattheright.
UltrasonographyandMRIshowedthecystinrelationtomedialplantarnerve,andedema-moderate
atrophywereobservedatthedistalmusclesofthefoot.
DISCUSSION:Footneuropathyindiabeticpatientsisacomplexprocess.So,inplanningtheinitial
treat-ment,medicalorsurgicaltherapyisselectedbasedonthelocationandtypeofthepathology.Foot
deformitiescanbecorrectedwithresting,anti-inflammatorytreatment,appropriateshoes,orthesisand
socks,andifrequired,anklestabilizationcanbeattempted.Ifthepatientisstillunresponsive,surgical
treatmentmaybeapplied.
CONCLUSION:Itisessentialtoinvestigatemorelocalizedreasonsliketarsaltunnelsyndromethatmay
mimicdiabeticneuropathy,shouldbetreatedprimarily.
©2015TheAuthors.PublishedbyElsevierLtd.onbehalfofSurgicalAssociatesLtd.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Thetarsaltunnelisa fibroosseousstructureofthefoot posi-tioned posteromedially, extending from the medial malleolus towardthenavicularbone.Itenclosestheposteriortibialtendon, flexorhallucislongustendonandflexordigitorumlongustendon, alongwiththeposteriortibialartery,veins,nervesandbranches
[1].
Tarsal tunnel syndrome is an entrapment neuropathic syn-dromethatdevelopsuponcompressionoftheposteriortibialnerve oritsbranches(medialandlateralplantarnerves)bytheflexor retinaculum.Systemicdiseaseprogressionwithneuropathysuch as diabetes should be considered during differential diagnosis. Elucidatingtheetiologyisthefirststepintreatment.Wereport a case withtarsaltunnel syndromemaskedby painful diabetic polyneuropathyinanefforttoraiseawarenessofthissyndrome anddescribetodiagnosticapproachtothepatient.
∗ Corresponding authorat:MedipolUniversity,FacultyofMedicine, Depart-ment of Radiology, Medipol Mega Hastaneler Kompleksi, Radyoloji Bölümü, TEM Avrupa Otoyolu Göztepe c¸ıkıs¸ı No: 1 Ba˘gcılar, 34214 ˙Istanbul, Turkey. Fax:+902124607050.
E-mailaddresses:[email protected](T.Ormeci),
[email protected](M.Mahirogulları),fi[email protected]
(F.Aysal).
2. Presentationofcase
A52-year-oldmalepatientwasadmitted withcomplaintsof numbness,burningsensationandpaininbothfeet(but predom-inantlyintherightfoot).Thesecomplaintswerepresentforthe preceding5 monthsbut increasedwithinthe last1 month. He hadbeenusingoralantidiabeticsduetotype2diabetes.He suf-feredfromthepaininhisrightfootincreaseduponwalking,which intensifiedthroughthefirsttoeandmedialfoot.
On neurological examination, bilateral hypoactive Achilles reflexes,hypoesthesiaandhypoalgesiawerepresentonbothfeet, moreprominentonrightfoot.Tineltestwaspositiveinrightankle. Noweaknesswasdetected.
Thelaboratoryresultswereasfollows:fastingplasmaglucose 243mg/dl,hemoglobinA1c9.2%,spoturinecreatinine299mg/dl andmicroalbumin232mg/dl.Thelaboratoryresultsshowedthat thepatienthad uncontrolleddiabetes,and hiscomplaintswere consideredtoberelatedtothisfinding.Hisparaestheticcomplaints improvedafterinsulintreatmentfordiabetes;however,hispain remained.
Nerve conduction studies revealed low compound muscle action potential (CMAP)amplitude in righttibialis nerve, non-detectablesensorynerveactionpotential(SNAP)ofmedialplantar nerveandchronicneurogenicchangesonneedleEMG(longterm, polyphasic,high-amplitudemotorunitpotentialswithdecreased recruitment)ofrightabductorhallucis(AH)andabductordigitiquinti
http://dx.doi.org/10.1016/j.ijscr.2015.08.033
2210-2612/©2015TheAuthors.PublishedbyElsevierLtd.onbehalfofSurgicalAssociatesLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
CASE
REPORT
–
OPEN
ACCESS
104 T.Ormecietal./InternationalJournalofSurgeryCaseReports15(2015)103–106
Fig.1. Nerveconductionstudiesofbilateralposteriortibialnerves.Med.Malleo:medialmalleol,Pop.Fossa:poplitealfossa,ADQ:abductordigitiquinti,AH:abductorhallucis.
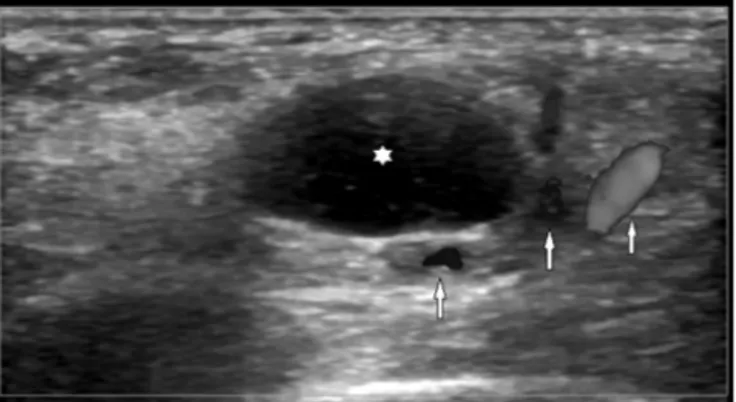
Fig.2. Wellcircumscribed,anechoiccysticlesion(asterisk)adjacenttotheposterior
tibialarteryandvein(arrows)inthemedialfoot.
(ADQ)muscles. These findings suggestedan entrapmentof the posteriortibialnerveattarsaltunnellevel(Fig.1).Amild sensory-motorpolyneuropathywasalsosuspected,becauseofslowingin motornervevelocityofexaminednervesandaslightdecreasein bothsuralnerves’SNAPamplitudes.Thiswasthoughttobe dia-betesrelated.Inaddition,resultscompatiblewithbilateralcarpal tunnelsyndromewerefound.
SuperficialUSimagingshowedahomogenouscysticlesionsized 15×10mmlocatedmediallytothemedialplantararteryandvein (Fig.2).
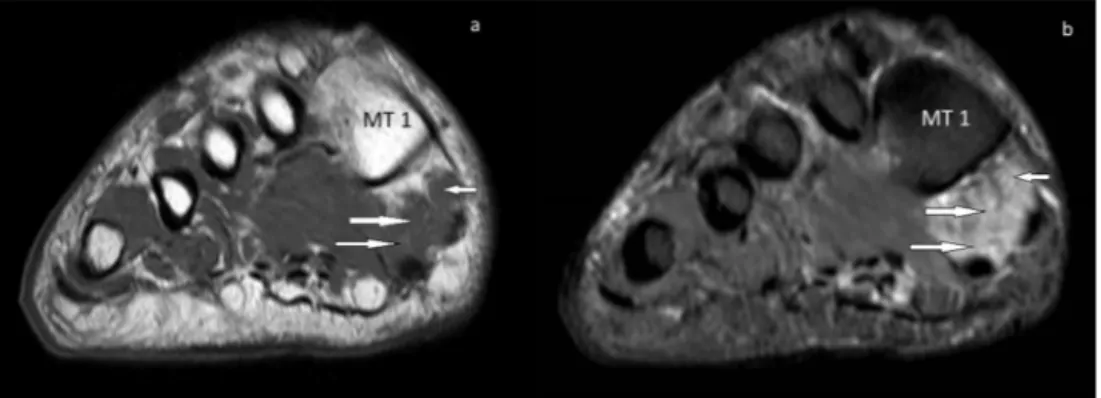
MRIofthefootandankle revealedahomogenous,T1 hypo-,T2hyperintense ganglioncystlocatedatthemedialcalcaneus, showingperipheralcontrastuptake.Thelocalizationofthecystin relationtotheflexorhallucislongustendon,posteriortibialartery andmedialplantarnervewasassessed(Fig.3).Edemaand mod-erateatrophywereobservedattheabductorhallucisandflexor hallucisbrevismuscles(Fig.4).
Tarsaltunnel syndromeinrelationwithmild sensory-motor polyneuropathyofdiabeticoriginwasdiagnosedbasedonclinical symptoms,electrophysiologicalfindingsandimagingofaganglion cystatthetarsaltunnellevelonUSandMRI.
Thepatientwasreferredtothedepartmentofsurgerywiththe diagnosisoftarsaltunnelsyndrome.However,thepatientrefused surgeryandregularlyusedhisanti-diabetesmedicationduringthe followingfourmonths,electrophysiologicalfindingsworsenedat controlinvestigation.
3. Discussion
Tarsal tunnel syndrome develops from compression of the posteriortibial nerve andits brancheswithinthetarsaltunnel. Compressionmayoccurduetotraumaticcausessuchasfracture, surgeryorscartissue[2],butitmayalsobeassociatedwith space-occupyinglesions includingtumors, ganglion, varicose vascular structuresandabnormalmuscletissue(accessoryflexordigitorum longusmuscleorhypertrophicadductorhallucis)[3].Inaddition, itmaydevelopinthefootinrelationtodeformitiessuchas
val-CASE
REPORT
–
OPEN
ACCESS
T.Ormecietal./InternationalJournalofSurgeryCaseReports15(2015)103–106 105
Fig.3.(a)AxialT1turbospinecho(TSE),(b)axialshorttauinversionrecovery(STIR)TSE,(c)axialpostcontrastT1spectralpresaturationwithinversionrecovery(SPIR)
demonstrateT1hypointense,T2hyperintenseandperipherallycontrastedcysticlesion(ganglioncyst)(star)withclosedrelationsintheflexorretinaculum(smallarrow),
medialplantarnerve(blackarrow),flexorhallucislongustendon(arrowhead)andposteriortibialartery–vein(largearrow)positionedmediallyonthecalcaneus(C)inthe
tarsaltunnellocalization.
Fig.4.(a)coronalT1TSE,(b)coronalshorttauinversionrecovery(STIR)TSE.Moderatevolumelossinaandhyperintensityinbareseenintheabductorhallucis(small
arrow)andflexorhallucisbrevis(largearrows)musclesattheplantarsideofthedistalfoot.Thefindingsarecompatiblewithmuscleatrophy.(MT1):firstmetatarsal.
gus/varusdeformity,pesplanusandtarsalcoalition[4].Systemic diseasessuchasdiabetes,rheumatoidarthritisandperipheral arte-rialdiseasemayalsocausetarsaltunnelsyndrome[5].Despiteall possiblecauses,theexactcauseofthediseaseissometimesunclear. Thesymptomsdependonwhich branchoftheposterior tib-ialnerveisinvolvedandthelocationoftheinvolvement.Physical examinationgenerallyshowslossofsensationattheplantarface ofthefootandpositiveTinel’sfindings.Patientssufferfrompain withaburningsensationatthetoesandplantarregion.The condi-tionmaybeaccompaniedbyparaesthesiaanddysesthesia,andthe findingsincreasewithactivity.Motorfunctionimpairmentisalate findingthatisgenerallyunnoticeable,andweaknessmaydevelop rarelyatthetoeflexors.Inadditiontotheclinicalmanifestations, decreasedconductionrateintheposteriortibialnerveasseenon EMGconfirmsthediagnosis.
US examinations can show space-occupying solid or cystic lesions;however,itisdifficulttoassessmuscleinnervationsinthe absenceofatrophy.
MRIexaminationsareextremelyusefulinassessingthetarsal tunnel, defining theetiology of thesyndromeand determining thedifferentialdiagnosis.Flexorhallucislongustenosynovitismay becomethecauseofnerve compressioninsevereconditions.In somecases,ankleganglionscausethesesymptoms.Inthemajority ofcases,thenervecannotbevisualizedcompletelyalongitstrace. However,thenervevolume,signalalterationsanddistortionsin thenerve traceshouldbeconsidered[6].Theseevaluationscan helpeliminatetheabove-mentionedetiologiccauses.Somecases maypresentwithamildsignalalterationintheabductorhallucis andflexorhallucisbrevismusclesinnervedbythemedial
plan-tarnerve,andadvancedcasesmaydevelopatrophy.Asinthecase presentedhere,atrophygenerallyaffectsdistalmuscles.
Systemic disease progression with neuropathy should be consideredduring differentialdiagnosis.Diabetic neuropathyis diagnosed in diabetic patientswith complaintsand findings of peripheralnerve dysfunctionin the absenceof other causative conditions[7].Themostcommonsymptomsofpolyneuropathy indiabeticpatientsaretingling,coldness,painandparaesthesia inthelegs,particularlynotableatdistalsites.Examinationshows stocking-glovesensoryloss.Moderateatrophyandparesismaybe encounteredattheintrinsicmusclesofthefoot[8].
Carpaltunnel syndrome, another entrapmentneuropathy, is encounteredinthediabeticpopulationathigherratethanthatin thegeneralpopulation.Watanabeetal.reportedthattibialnervein tarsaltunnelandmediannerveincarpaltunnelincreaseinterms ofcrosssectionalareaindiabeticpatients[9].Thoseresultswere compatiblewithsystemiceffectsofdiabetesandourpatientalso hadcarpaltunnelsyndromeaccompanyingtarsaltunnelsyndrome. Whether the entrapment neuropathies that develop in dia-beticpatientsaredirectlyassociatedwithdiabetesiscontroversial
[10,11].Footneuropathyindiabeticpatientsisacomplexprocess.
So,inplanningtheinitialtreatment,medicalorsurgicaltherapy isselectedbasedonthelocationandtypeofthepathology.Foot deformitiescanbecorrectedwithresting,anti-inflammatory treat-ment,appropriateshoes,orthesisandsocks,andifrequired,ankle stabilizationcanbeattempted.Physicaltherapymodalitiesmight bepreferredinsuitablecases.Tricyclicantidepressantmedications andantiepilepticagentssuchasgabapentinandpregabalinmaybe useful.Lidocainandcortisonecanbeinjectedlocallytothenerve
CASE
REPORT
–
OPEN
ACCESS
106 T.Ormecietal./InternationalJournalofSurgeryCaseReports15(2015)103–106
trace.Ifthepatientisstillunresponsive,surgicaltreatmentmaybe applied[1].
4. Conclusion
Successfultreatmentoftheinitialconditionofneuropathicfoot painindiabeticpatientsinvolveseliminationofthecausesof neu-ropathicpain,particularlytarsaltunnelsyndrome.Pathologiesthat maymimicdiabeticneuropathyshouldbetreatedprimarily. Funding None. Ethicalapproval N/A. Consent Obtained. Conflictofinterest None. References
[1]E.M.Delfaut,X.Demondion,A.Bieganski,M.C.Thiron,H.Mestdagh,A.Cotten,
Imagingoffootandanklenerveentrapmentsyndromes:from
well-demonstratedtounfamiliarsites,Radiographics23(2003)613–623.
[2]O.C.Aszmann,J.M.Ebmer,A.L.Dellon,Cutaneousinnervationofthemedial
ankle:ananatomicstudyofthesaphenous,sural,andtibialnervesandtheir
clinicalsignificance,FootAnkleInt.19(1998)753–756.
[3]G.J.Sammarco,S.F.Conti,Tarsaltunnelsyndromecausedbyananomalous
muscle,J.BoneJointSurg.Am.76(1994)1308–1314.
[4]E.Trepman,N.J.Kadel,K.Chisholm,L.Razzano,Effectoffootandankle
positionontarsaltunnelcompartmentpressure,FootAnkleInt.20(1999)
721–726.
[5]A.Donovan,Z.S.Rosenberg,C.F.Cavalcanti,MRimagingofentrapment
neuropathiesofthelowerextremity.Part2.Theknee,leg,ankle,andfoot,
Radiographics30(4)(2010)1001–1019.
[6]M.F.Lee,P.T.Chan,L.F.Chau,K.S.Yu,Tarsaltunnelsyndromecausedby
talocalcanealcoalition,Clin.Imaging26(2002)140–143.
[7]A.J.Boulton,F.A.Gries,J.A.Jervell,Guidelinesforthediagnosisandoutpatient
managementofdiabeticperipheralneuropathy,Diabet.Med.15(1998)
508–514.
[8]S.J.Bird,M.J.Brown,Diabeticneuropahhies,in:B.Katırjı,H.J.Kominski,D.C.
Preston,R.L.Ruff,B.E.Shapino(Eds.),NeuromuscularDisordersinClinical
Practice,ButterworthHeinemann,USA,2002,pp.598–621.
[9]T.Watanabe,H.Ito,A.Sekine,Y.Katano,T.Nishimura,Y.Kato,etal.,
Sonographicevaluationoftheperipheralnerveindiabeticpatients:the
relationshipbetweennerveconductionstudies,echointensity,and
cross-sectionalarea,J.UltrasoundMed.29(2010)697–708.
[10]D.M.Fraser,I.W.Campbell,D.J.Ewing,B.F.Clarke,Mononeuropathyin
diabetesmellitus,Diabetes28(1979)96–101.
[11]B.S.Boyd,A.Dilley,Alteredtibialnervebiomechanicsinpatientswith
diabetesmellitus,MuscleNerve.50(2014)216–223.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.