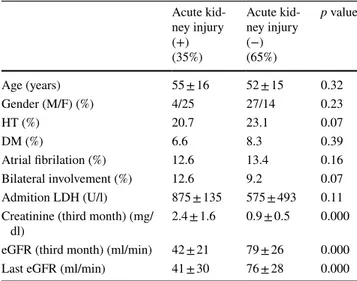
Acute renal infarction in Turkey: a review of 121 cases
Tam metin
Şekil
Benzer Belgeler
Myocardial infarction (MI) is very rare during pregnancy (1/10000), happens mostly during the third trimester and puerperium and mortality rates are high (19-21 %) (1).. In most
Effects of intracoronary infusion of peripheral blood stem-cells mobilised with granulocyte-colony stimulating factor on left ventricular systolic function and restenosis
[9] Supporting this data, development of acute coronary syndromes due to se- vere thrombus burden induced by the use of anabolic steroids has been reported.. [10] In our case,
Comparison of treatment delays in patients admitted with acute myocardial infarction during the pandemic (TURKMI-2) and pre- pandemic (TURKMI-1) periods. Time to treatment
CI - confidence interval; DPR - dual poor responsiveness; HTPR - high on-treatment platelet reactivity; NYHA - New York Heart Association; PRA - poor responsiveness to aspirin; PRC
Methods: In total, 1034 patients [514 patients with ST-segment elevation myocardial infarction (STEMI) and 520 with unstable angina/non-STEMI (UA/NSTEMI)] hospitalized for ACS
In his admission electrocardiogram (ECG), incomplete left bundle brunch block, ST-segment depression in V3-6, and ST-segment elevation with pathologic Q wave in the inferior
The aim of this study is to describe the epidemiological features of acute myo- cardial infarction (AMI) and outcomes in patients admitted for tertiary care in Trinidad.. We used
