M
How to cite this article: Yücel AO, Demir-Dora D, İsbir MF, Dora B. Agomelatine is superior to melatonin in pain suppression: An experimental study. Neurol Sci Neurophysiol 2020;37:203-7.
Agomelatine is Superior to Melatonin in Pain Suppression: An
Experimental Study
Ali Okan Yücel, Devrim Demir-Dora, Mehmet Ferit İsbir1, Babür Dora2
Department of Medical Pharmacology, Faculty of Medicine, Akdeniz University, Antalya, 1Department of Pharmacology, Istinye University Faculty of Pharmacy, Istanbul, 2Department of Neurology, Faculty of Medicine, Akdeniz University, Antalya, Turkey
Submitted: 14-Apr-2020 Revised: 05-May-2020 Accepted: 26-May-2020 Published: 29-Dec-2020
Introduction
elatonin is a hormone synthesized in and secreted from the pineal gland which is involved in circadian functions like the sleep–wake cycle, mood, immune system, inhibition of oncogenesis, antioxidant functions and free radical scavenging, vasoregulation, and pain.[1] Melatonin has been shown to have antinociceptive
properties at pharmacological doses in many experimental studies and has been utilized in
numerous pain conditions such as cluster headache, migraine, tension-type headache, fibromyalgia and chronic back pain.[2-6] Melatonin’s effect on pain suppression is not only by its effect on opioid receptors but also via the melatonin receptors MT1 and mainly
Address for correspondence: Dr. Devrim Demir-Dora, Department of Medical Pharmacology, Akdeniz University Faculty of Medicine, Konyaaltı, Antalya, Turkey. E-mail: [email protected] This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
Objective: Agomelatine is a synthetic analog of melatonin with selective agonist action on melatonin MT1 and MT2 receptors and antagonistic effect on serotonin 5HT2c receptors. Similar to melatonin, it also has antinociceptive properties. There are only a few studies comparing the antinociceptive effects of agomelatine to melatonin. Methods: Male Wistar albino rats were grouped into seven treatment groups and a control group (8 animals each). Treatment groups received intraperitoneal injections of agomelatine 25 mg/kg, 35 mg/kg and 50 mg/kg; agomelatine 35 mg/kg + luzindole 10 mg/kg; melatonin 60 mg/kg and 90 mg/ kg and melatonin 60 mg/kg + sertraline 10 mg/kg. Animals were placed on a hot plate and time to pain avoidance behavior was measured. Results: Agomelatine 25 mg/kg, 35 mg/kg and 50 mg/kg were significantly superior to placebo (all
p < 0.0001); agomelatine 35 mg/kg and 50 mg/kg were significantly superior
to melatonin 60 mg/kg (p < 0.05 and p < 0.01, respectively) and melatonin 90 mg/kg (p < 0.001 and p < 0.001, respectively) in prolonging reaction times. Agomelatine 50 mg/kg was superior to melatonin 60 mg/kg + sertraline 10 mg/ kg (p < 0,05); on the contrary; agomelatine 25 mg/kg was significantly inferior to this combination in prolonging reaction times (p = 0,041). Melatonin 90 mg/ kg but not 60 mg/kg was significantly superior to placebo in prolonging reaction times (p < 0.0001). Both agomelatine 50 mg/kg and 35 mg/kg were superior to agomelatine 25 mg/kg (p < 0.0001 and p = 0.002, respectively), but the difference between agomelatine 50 mg/kg and 35 mg/kg was not significant. Conclusions: We demonstrated that agomelatine is superior to melatonin on pain behavior in a dose-dependent manner using an experimental pain model. The addition of a serotonergic agent increased the antinociceptive effect of melatonin in regard to agomelatine, but high doses of agomelatine were still more effective, suggesting a dose-dependent effect of agomelatine on 5-HT2c receptors.
Keywords: 5 HT2c receptor, agomelatine, melatonin, nociception, pain,
serotonin
A
b
str
ac
t
Access this article online
Quick Response Code:
Website: www.nsnjournal.org
MT2, as has been demonstrated by studies showing that luzindole, a MT1 and MT2 receptor antagonist, abolishes the antinociceptive effect of melatonin completely and the MT2 blocker 4-phenyl-2-propionamidotetralin has a partial diminishing effect.[7-9] Melatonin MT1 and MT2 receptors are widely distributed in pain involved areas such as the thalamus, hypothalamus, trigeminal nucleus, spinal laminae I–V and X and spinal-trigeminal projections.[10-12] It also has been shown to attenuate trigeminovascular nociception triggered by spreading cortical depression in rats by reducing fos expression and diminishing NO synthetase immunoreactive cell numbers in the trigeminal caudal nucleus.[13]
The antidepressant drug agomelatine is a synthetic analog of melatonin with selective agonist action on melatonin MT1 and MT2 receptors and antagonistic effect on serotonin 5HT2c receptors.[14-16] The inhibitory role of 5HT2c receptors on the dopaminergic and noradrenergic pathways also gives agomelatine a noradrenergic and dopaminergic disinhibitory function.[17-19] Agomelatine has recently come into interest for its possible role in pain. Agomelatine has been investigated and found effective in the treatment of experimental painful neuropathy both alone or when combined with gabapentin.[20,21] Similarly, some other antidepressants with antinociceptive properties such as amitriptyline, mirtazapine and mianserin also have antagonistic effect on the serotonin 5-HT2c receptor.[22,23] Despite these similar effects on receptors involved in pain, there are few studies about the antinociceptive effects of agomelatine in the literature so far, and to our knowledge, no studies have compared the antinociceptive effects of agomelatine and melatonin directly.[20,21,24,25] A single study compared agomelatine + a serotonin antagonist to melatonin + a serotonin antagonist and found both combinations ineffective, while the addition of gabapentin to both groups produced marked antiallodynic effect in the agomelatine group but not in the melatonin group.[20] The aim of this study was to assess whether agomelatine has similar antinociceptive properties like melatonin in an experimental pain model.
Methods
In this study, adult male Wistar albino rats (290 ± 30 g) which were bred in the Research Animals Unit were used. All experiments were conducted in accordance with the Guidelines on Ethical Standards for Investigation of Experimental Pain in Animals, and ethic approval was obtained from the Akdeniz University Local Ethics Committee on Animal Experiments (Approval number: 2013.06.01).
Melatonin, agomelatine, luzindole and sertraline were purchased from Sigma Aldrich (St Louis, MO, USA). For the studies, a May Com 9601 Analgesic hot plate was used.
All rats were kept in environmentally controlled conditions at 24.0 ± 1.0°C with 50% humidity and a 12 hour light/dark cycle 1 week prior to the experiments. The rats were given free access to food and water. Seven treatment groups and a control group, each consisting of eight randomly distributed animals were formed.
Control: 1 ml of saline was injected intraperitoneally • AGO25: 25 mg/kg of agomelatine was injected
intraperitoneally
• AGO35: 35 mg/kg of agomelatine was injected intraperitoneally
• AGO50: 50 mg/kg of agomelatine was injected intraperitoneally
• AGO35 + LUZ: First 10 mg/kg luzindole was injected intraperitoneally, and 10 min later, 35 mg/kg of agomelatine was injected intraperitoneally
• MEL60: 60 mg/kg of melatonin was injected intraperitoneally
• MEL90: 90 mg/kg of melatonin was injected intraperitoneally
• MEL60 + SERT: 60 mg/kg of melatonin was injected intraperitoneally, and 10 min later, 10 mg/kg sertraline was injected intraperitoneally.
Animals were injected with the test substances intraperitoneally (not exceeding 1 ml) and were placed on a hot plate with a set surface temperature of 50.0°C ± 5.0°C which was placed inside a 17 cm × 20 cm open glass cylinder, 30 min after the last injection. Testing was started as soon as the animal was placed on the hot plate and time to avoidance action (jumping, paw withdrawal or rear paw licking (for a detailed description of the avoidance behavior, please refer to the literature[26])) was measured and noted by three different observers simultaneously. The test was terminated after 50 s to avoid tissue injury and 50 s was taken as the cut-off time. The surface was cleaned with 20% ethanol after each testing and every animal was only used once. The mean average time noted by the three observers was used.
Statistical analysis
Data were analyzed by SPSS IBM 24 software (IBM Corp, Armonk, NY). One-way analysis of variance (ANOVA) and post hoc Tukey test were performed for statistical comparison between three or more groups. Homogeneity of variances was tested by Levene’s test. When the variances were not
homogeneous, non-parametric Kruskal–Wallis test was done instead of ANOVA. The significance level was accepted as p < 0.05.
Results
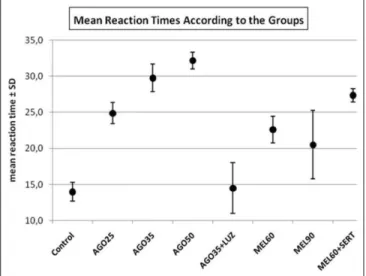
Reaction times in all groups are presented in Table 1 and Figure 1.
The reaction times for all groups except the MEL60 and AGO35 + LUZ group were significantly longer than the control group (p < 0.0001).
Agomelatine 25 mg/kg, 35 mg/kg and 50 mg/kg were significantly superior to placebo (p < 0.0001, p < 0.0001 and p < 0.0001, respectively) in prolonging reaction times.
Figure 1: Reaction times (±standard deviation) to hot plate exposure
in the treatment groups. AGO25: Agomelatine 25 mg/kg, AGO35: Agomelatine 35 mg/kg, AGO50: Agomelatine 50 mg/kg, AGO35+LUZ: Luzindole 10 mg/kg + Agomelatine 35 mg/kg, MEL60: Melatonin 60 mg/kg, MEL90: Melatonin 90 mg/kg, MEL60+SER: Melatonin 60 mg/kg + Sertraline 10 mg/kg
Table 1: Reaction times to hot plate exposure in the groups
Reaction time(s)±SD Control 14.00±1.31 AGO25 24.87*,††±1.46 AGO35 29.75*,†,‡,¶,††±1.91 AGO50 32.17*,†,‡,¶,††,§±1.17 AGO35+LUZ 14.50±3.50 MEL60 22.62±1.85 MEL90 20.50*±4.75 MEL60+SERT 27.37*,||,**±0.92
Please refer to the text for explanations of the groups. *Superior compared to placebo (p<0.0001), †Superior compared to MEL90 (p<0.001), ‡Superior compared to MEL60 (p<0.05 for AGO35 and p<0.01 for AGO50), §Superior compared to MEL60+SERT (p<0.05), ||Superior compared to AGO25 (p<0.05), ¶Superior compared to AGO25 (p<0.002 for AGO35 and p<0.0001 for AGO50), ††Superior compared to AGO35+LUZ (p<0.05), **Superior compared to MEL90 (p<0.002). MEL: Melatonin, AGO: Agomelatine, LUZ: Luzindole, SERT: Sertraline, SD: Standard deviation
Agomelatine 35 mg/kg and 50 mg/kg were significantly superior to melatonin 60 mg/kg (p < 0.05 and p < 0.01, respectively) and melatonin 90 mg/kg (p < 0.001 and
P < 0.001, respectively) in prolonging reaction times.
Subjects in the agomelatine 25 mg/kg group had longer reaction times compared to both melatonin doses, but this difference did not reach significance.
Agomelatine 50 mg/kg was superior to melatonin
60 mg/kg + sertraline 10 mg/kg (p < 0.05), but agomelatine 35 mg/kg was not. On the contrary agomelatine 25 mg/kg was significantly inferior to this combination in prolonging reaction times (p < 0.05). Both agomelatine 50 mg/kg and 35 mg/kg were superior to agomelatine 25 mg/kg (p < 0.0001 and p = 0.002, respectively), but the difference between agomelatine 50 mg/kg and 35 mg/kg was not significant. All three agomelatine doses were superior to the agomelatine– luzindole combination (p < 0.05).
Melatonin 90 mg/kg was significantly superior to placebo in prolonging reaction times (p < 0.0001), but although melatonin 60 mg/kg was better than placebo, this difference did not reach significance.
Reaction times did not differ between the MEL60 and MEL60+SERT groups, but MEL60 + SERT was significantly better than MEL90 (p = 0.002). Subjects in the agomelatine–luzindole combination group had similar reaction times compared to controls.
Discussion
Our results demonstrate that agomelatine is highly effective in pain control compared to placebo even at lower doses like 25 mg/kg. This effect was dose dependent and was blocked by luzindole.
Kasap and Can reported that agomelatine 40 mg/kg and 60 mg/kg prolonged reaction times to the tail clip test and hot plate test in rodents and hypothesized that the possible antinociceptive effect of agomelatine might be through spinal mechanisms as well as at suprapinal levels because the tail clip test predominantly shows nociceptive transmission at the spinal level and the hot plate test is mainly involved in supraspinal nociceptive mechanisms.[27-29] In the aforementioned study, agomelatine also reduced the number of acetic acid-induced writhing behavior which was suggestive of an peripherally mediated antinociceptive effect as well.[27-29] Antinociceptive of naloxone to the animals abolished the antinociceptive effect of agomelatine, leading the authors to conclude that the opioid receptors were also involved in agomelatine-mediated nociception.[27]
Aydın et al. showed that doses of 40 mg/kg and 80 mg/kg agomelatine improved hyperalgesia and mechanical and thermal allodynia in experimental diabetic neuropathic pain.[21] This effect was suppressed with inhibitors of catecholamine synthesis or adrenoreceptor blockers. They suggested that agomelatine possibly exerted its antinociceptive effect over the catecholaminergic system.
We also demonstrated that agomelatine was better in controlling pain compared to melatonin. This effect was only evident at doses over 25 mg/kg. Although agomelatine has been compared to melatonin in numerous studies in regard of its effects in sleep regulation and depression, studies comparing these two agents in pain are scarce. Both agomelatine and melatonin have effects on pain involved neurotransmitter systems which suggests that they would be effective in pain management.[7-9,14-19] Both experimental and clinical studies have demonstrated the effectiveness of melatonin in pain conditions and studies with agomelatine have begun to accumulate.[2-6,20,21,24,25] In the only study comparing agomelatine and melatonin, both agomelatine and melatonin were found to be ineffective in controlling allodynia when combined with a serotonin antagonist. The addition of gabapentin to both groups produced marked antiallodynic effect in the agomelatine group but not in the melatonin group. The authors suggested that this effect was due to the involvement of noradrenalin-mediated pain control mechanisms via
2- and 2-adrenoreceptors.[20]
We combined melatonin which only acts via MT1 and MT2 receptors with sertraline, a selective serotonin reuptake inhibitor, to achieve a similar effect as agomelatine which is known to also block 5-HT2c receptors involved in pain. The combination of melatonin with sertraline was superior to low doses (25 mg/kg) and similar to medium doses (35 mg/kg) of agomelatine, while melatonin alone was similar to low doses and inferior to medium doses of agomelatine. High-dose (50 mg/kg) agomelatine was better in controlling pain compared to the melatonin–sertraline combination. This suggests that the addition of an agent acting on serotonin receptors to melatonin increases its antinociceptive properties. We were unable, though, to show any difference between melatonin 60 mg/ kg and sertraline combined compared to melatonin 60 mg/kg alone, although the combination was significantly better than higher dose melatonin (90 mg/kg). These results might suggest that the effect of agomelatine on 5-HT2c receptors could be dose related and show that serotonin receptors also play an important role in the antinociceptive effect of agomelatine.
As a result, we demonstrated that agomelatine is superior to melatonin on pain behavior in a dose-dependent manner using an experimental pain model. The addition of a serotonergic agent increases the antinociceptive effect of melatonin in regard to agomelatine, but high doses of agomelatine are still more effective, suggesting a dose-dependent effect of agomelatine on 5-HT2c receptors.
Financial support and sponsorship
This study was funded by the Akdeniz University Scientific Research Project Unit.
Conflicts of interest
There are no conflicts of interest.
References
1. Xu S, Wei W, Shen Y, Hao J, Ding C. Studies on the antiinflamatory, immnoregulatory, and analgesic actions of melatonin. Drug Dev Res 1996;39:167-73.
2. Calandre EP, Slim M, Garcia-Leiva JM, Rodriguez-Lopez CM, Torres P, Rico-Villademoros F. Agomelatine for the treatment of patients with fibromyalgia and depressive symptomatology: An uncontrolled, 12-week, pilot study. Pharmacopsychiatry 2014;47:67-72.
3. Peres MF, Zukerman E, da Cunha Tanuri F, Moreira FR, Cipolla-Neto J. Melatonin, 3 mg, is effective for migraine prevention. Neurology 2004;63:757.
4. Leone M, D’Amico D, Moschiano F, Fraschini F, Bussone G. Melatonin versus placebo in the prophylaxis of cluster headache: A double-blind pilot study with parallel groups. Cephalalgia 1996;16:494-6.
5. Miano S, Parisi P, Pelliccia A, Luchetti A, Paolino MC, Villa MP. Melatonin to prevent migraine or tension-type headache in children. Neurol Sci 2008;29:285-7.
6. Citera G, Arias MA, Maldonado-Cocco JA, Lázaro MA, Rosemffet MG, Brusco LI, et al. The effect of melatonin in patients with fibromyalgia: A pilot study. Clin Rheumatol 2000;19:9-13.
7. Ambriz-Tututi M, Granados-Soto V. Oral and spinal melatonin reduces tactile allodynia in rats via activation of MT2 and opioid receptors. Pain 2007;132:273-80.
8. Wang T, Li SR, Dai X, Peng YL, Chen Q, Wang R. Effects of melatonin on orphanin FQ/nociceptin-induced hyperalgesia in mice. Brain Res 2006;1085:43-8.
9. Tu Y, Sun RQ, Willis WD. Effects of intrathecal injections of melatonin analogs on capsaicin-induced secondary mechanical allodynia and hyperalgesia in rats. Pain 2004;109:340-50. 10. Weaver DR, Rivkees SA, Reppert SM. Localization and
characterization of melatonin receptors in rodent brain by in vitro autoradiography. J Neurosci 1989;9:2581-90.
11. Williams LM, Hannah LT, Hastings MH, Maywood ES. Melatonin receptors in the brain and pituitary. J Pineal Res 1995;19:173-7.
12. Zahn PK, Lansmann T, Berger E, Speckmann EJ, Musshoff U. Gene expression and functional characterization of melatonin receptors in the spinal cord of the rat: İmplications for pain modulation. J Pineal Res 2003;35:24-31.
13. Le Grand SM, Patumraj S, Phansuwan-Pujito P, Srikiatkhachorn A. Melatonin inhibits cortical spreading depression-evoked trigeminal nociception. Neuroreport
2006;17:1709-13.
14. Millan MJ, Brocco M, Gobert A, Dekeyne A. Anxiolytic properties of agomelatine, an antidepressant with melatoninergic and serotonergic properties: Role of 5-HT2C receptor blockade. Psychopharmacology (Berl) 2005;177:448-58.
15. Millan MJ, Gobert A, Lejeune F, Dekeyne A, Newman-Tancredi A, Pasteau V, et al. The novel melatonin agonist agomelatine (S20098) is an antagonist at 5-hydroxytryptamine 2C receptors, blockade of which enhances the activity of frontocortical dopaminergic and adrenergic pathways. J Pharmacol Exp Ther 2003;306:954-64.
16. Tardito D, Molteni R, Popoli M, Racagni G. Synergistic mechanisms involved in the antidepressant effects of agomelatine. Eur Neuropsychopharmacol 2012;22 Suppl 3:S482-6.
17. Di Matteo V, Cacchio M, Di Giulio C, Esposito E. Role of serotonin(2C) receptors in the control of brain dopaminergic function. Pharmacol Biochem Behav 2002;71:727-34.
18. Alex KD, Pehek EA. Pharmacologic mechanisms of serotonergic regulation of dopamine neurotransmission. Pharmacol Ther 2007;113:296-320.
19. Gobert A, Rivet JM, Lejeune F, Newman-Tancredi A, Adhumeau-Auclair A, Nicolas JP, et al. Serotonin(2C) receptors tonically suppress the activity of mesocortical dopaminergic and adrenergic, but not serotonergic, pathways: A combined dialysis and electrophysiological analysis in the rat. Synapse 2000;36:205-21.
20. M’Dahoma S, Poitevin M, Dabala E, Payan H, Gabriel C, Mocaër E, et al. 2- and 2-adrenoreceptor-mediated efficacy of the atypical antidepressant agomelatine combined with gabapentin to suppress allodynia in neuropathic rats with ligated ınfraorbital or sciatic nerve. Front Pharmacol 2018;9:587-604. 21. Aydın TH, Can ÖD, Demir Özkay Ü, Turan N. Effect of
subacute agomelatine treatment on painful diabetic neuropathy: İnvolvement of catecholaminergic mechanisms. Fundam Clin Pharmacol 2016;30:549-67.
22. Di Matteo V, Di Mascio M, Di Giovanni G, Esposito E. Acute administration of amitriptyline and mianserin increases dopamine release in the rat nucleus accumbens: Possible involvement of serotonin2C receptors. Psychopharmacology (Berl) 2000;150:45-51.
23. Millan MJ, Gobert A, Rivet JM, Adhumeau-Auclair A, Cussac D, Newman-Tancredi A, et al. Mirtazapine enhances frontocortical dopaminergic and corticolimbic adrenergic, but not serotonergic, transmission by blockade of alpha2-adrenergic and serotonin2C receptors: A comparison with citalopram. Eur J Neurosci 2000;12:1079-95.
24. Chenaf C, Chapuy E, Libert F, Marchand F, Courteix C, Bertrand M, et al. Agomelatine: A new opportunity to reduce neuropathic pain – Preclinical evidence. Pain 2017;158:149-60. 25. Tabeeva GR, Sergeev AV, Gromova SA. Possibilities of
preventive treatment of migraine with MT1 and MT2 agonist and 5-HT2c receptor antagonist agomelatine (Valdoxan). Zh Nevrol Psikhiatr Im S S Korsakova 2011;111:32-6.
26. Suaudeau C, do-Rego JC, Costentin J. Modifications in avoidance reactions of mice, on a second exposure to the hot plate, resist to various amnesia-inducing treatments. Brain Res Cogn Brain Res 2005;25:339-47.
27. Kasap M, Can ÖD. Opioid system mediated anti-nociceptive effect of agomelatine in mice. Life Sci 2016;163:55-63.
28. Cornélio AM, Mendes-Gomes J, Fugimoto JS, Morgan MM, Nunes-de-Souza RL. Environmentally induced antinociception and hyperalgesia in rats and mice. Brain Res 2011;1415:56-62. 29. Le Bars D, Gozariu M, Cadden SW. Animal models of