Non-invasive
detection
and
monitoring
of
experimental
hydrocephalus
with
distortion
product
otoacoustic
emissions
Hande
Ezerarslan
a,*,
Gu¨c¸lu¨ Kaan
Beriat
a,
Raziye
Handan
Nurhat
b,
Burak
Kazancı
b,
Ferda
Topal
C¸elikkan
c,
Bizden
Sabuncuog˘lu
c,
Hakan
Sabuncuog˘lu
baUfukUniversityMedicalSchool,DepartmentofOtorhinolaryngology,Turkey bUfukUniversityMedicalSchool,DepartmentofNeurosurgery,Turkey
cAnkaraUniversityMedicalSchool,DepartmentofHistologyandEmbriology,Turkey
1. Introduction
Hydrocephalus is a pathologic condition commonly co-existingwithintracranialhypertensioninwhichcerebrospinal fluid (CSF) is accumulated due to imbalance between CSF
production and absorption or obstruction in the CSF circulatory pathways [1]. It is classified as communicating whenthereis adisturbanceintheCSFabsorptionand non-communicatingwhenthereisanobstructioninthecirculatory pathways of CSF between the ventricles and subarachnoid space. In the fetal and neonatal period when thevestibular aquaduct is patent, hydrocephalus is usually non-communi-cating and CSF flow and intracranial pressure changes are directlyconductedviatheendolymphaticductandvestibular
ARTICLE INFO
Articlehistory:
Received8October2015 Accepted16November2015 Availableonline29December2015
Keywords: Otoacousticemissions Hydrocephalus Innerear Obstructivehydrocephalus ABSTRACT
Objective: We aimed tofind out the effectsof short term and long term hydrocephalus and intracranialventricularvolumechangesoncochlearfunctionsbyusingdistortionproductotoacoustic emission(DPOAE)inexperimentalhydrocephalusratmodelsforthefirsttimeinliterature. Methods: Thisstudywasperformedwith48healthy,adult(8weeksold),Sprague–Dawleyrats whichweighedbetween200and240g.Sixgroupswereformedinthisstudy:shorttermcontrol, shortterm sham,shortterm hydrocephalus,long termcontrol,long termsham and long term hydrocephalusgroups.Eachgroupcontainedeightrats.Shorttermperiodwas4weeksandlong termperiodwas8weeksafterthestudystarted.Attheendoftheseperiods,DPOAEmeasurements wereperformedandthenratsweresacrificedtodetermineventricularvolumes.
Results: DPOAE values at all frequencies were significantly decreased in the short term hydrocephalusgroupwhencomparedtotheshorttermcontrolandshorttermshamgroups.DPOAE valuesatallfrequenciesweresignificantlydecreasedinthelongtermhydrocephalusgroupwhen comparedtothelongtermcontrolandlongtermshamgroups.Besides,longtermshamgroupwhich hadhigherventricularvolumesthanlongtermcontrolgroupalsohadlowerDPOAEmeasurements. SignificantassociationswerepresentbetweenDPOAEmeasurementsandventricularvolumesin hydrocephalusmodels.
Conclusion: Thefunctionaldisturbancesincochlearfunctionsduetohydrocephalushavebeen demonstratedwithDPOAEmeasurementsinthisstudy.DPOAEmeasurementsmaybethought as an easily applicable non-invasive method in detection and follow-up of patients with hydrocephalus.Our findingsshouldbesupported with clinicalstudies inhumans.
ß2015ElsevierIrelandLtd.Allrightsreserved.
* Correspondingauthorat:UfukUniversityMedicalSchool,Departmentof Otorhinolaryngology,Ankara,Turkey.Tel.:+903122044383.
E-mailaddress:[email protected](H.Ezerarslan).
ContentslistsavailableatScienceDirect
Auris
Nasus
Larynx
j our na l ho me p a ge : w ww . e l se v i e r . com / l oc a te / a n l
http://dx.doi.org/10.1016/j.anl.2015.11.004
aquaducttothecochleacausingfunctionaldisturbancesinthe ear[2].
The functional disturbances of cochlea can be easily detectedbydistortionproductotoacousticemission(DPOAE) inpatientswithhealthymiddleears[3].DPOAEisdependent on the otoacoustic emissions caused by overlapping of two different waveforms in the non-diseased cochlea by two different tone stimuli. By this way, frequency specific informationcanbecollected.Inthediseasedcochlea,DPOAE isusuallydecreasedorlostindifferentfrequencies,aproperty whichdirectlyincludestheDPOAEintoclinicalpracticetofind outthecause ofsensorineuralhearingloss[4,5].
In the literature, non-invasive methods had been used forthedetection ofintracranialpressurechanges[6–9]such as impedance [6], and otoacoustic emission (OAE) [7,8]
measurements. Magnano et al. [6] observed OAE changes with respect to the change in intracranial pressures instantaneously by changing the position of the patient, whileBukietal.[8]observedOAEchangesinstantaneously againinagerbilmodelbyincreasingtheintracranialpressure gradually. These studies did not includeventricular volume changes. Herein, we aimed to find out the effects of hydrocephalus and intracranial ventricular volume changes on cochlear functions by using DPOAE measurements in experimental non-communicating hydrocephalus rat models inshort(4weeks)andlongterms(8weeks)forthefirsttime inliterature.
2. Methods
Theexperimentaldesignwasreviewedandapproved(date: 17.04.2014;number:113) bythe ethicscommittee inanimal experiments atKOBAYIC,andthe study was carriedout in compliancewiththeguidelinesforanimalexperimentationat theDepartmentofLaboratoryAnimalScienceatKOBAYIC (Ankara, Turkey). All animals used for the experiments receivedcareaccordingtothePrinciplesofLaboratoryAnimal Care recommended by the National Society of Medical Researchand the Guidefor the Care and Useof Laboratory Animals,proposedandpreparedbytheNationalAcademyof Sciences and published by the National Institutes of Health (NIHpublicationNo.85-23,revised1996).
Thisstudywasperformedon48healthy,adult(8weeksold), Sprague–Dawleyratswhichweighedbetween200 and240g. Theenvironmentfortheseratsinthesettingofthisstudywasas follows:12h darkand12hlightinaday,218Cstableroom temperature,externalnoise<50dB, andfreefood andwater income.Theoraltemperatureoftheratswasbetween37.5and 39.08C.
Sixgroups were formed inthis study:short termcontrol, shorttermsham,shorttermkaolin(hydrocephalus),longterm control,longtermshamandlongtermkaolin(hydrocephalus) groups.Eachgroupcontainedeightrats.Shorttermperiodwas 4 weeks and long term period was 8 weeks after the study started. At the end of these periods, DPOAE measurements wereperformedandthenratswereeuthanized.
Intracranialsurgerywasperformedtoallatthebeginningof thestudy exceptthecontrol groups:
2.1. Surgicaltechnique
Anesthesia was performed with intraperitoneal ketamine (80mg/g).Ratswerepositionedproneonasurgicalplatform with their four extremities andchins fixed. A2-cm midline verticalskinincisionwasperformedbetweentheocciputand firstcervicalvertebraanddurawasexploredafterthemuscular layerwaspulledawaytobothsides.Theshamgroupreceived 0.1ml serum physiologic and the study group received a 0.1-mlinjectionofkaolin(250mg/ml),asoftindustrialclay which ischeapandeasy touse,intothecerebellomedullary system via cisterna magna after 0.1ml CSF was taken
[10,11]. After this procedure, subcutaneous and cutaneous tissue was primarily sutured and the rats were placed in a resting cage and then in their study environmentafter total recoveryfromanesthesia.
2.2. Distortionproductotoacoustic emission(DPOAE) measurements
AlloftheratsunderwentDPOAEmeasurementattheir4th (short term phase) and 8th (long term) weeks after surgery. External and middle ear diseases (i.e. otitis media) were excluded after a detailed otoscopic examination because DPOAEmeasurementsmightbedisturbedduetothepresence of suchdiseases.
After sedation with intraperitoneal 80mg/g ketamine, DPOAE measurements were performed with Otodynamics ILO-288 Echoport equipment (Otodynamics Ltd., London, UK) with a plastic adaptor which showed the absence of artifacts in otoacoustic emissions.Positioning the rats’ head, DPOAEmeasurementswerestartedafterappropriate configu-rationofthestimulantwaveformwasobtained,probemarkerof thedevicewasturnedtogreenandasaresult,rightpositionof the device was confirmed. The DPOAEs (2f1 f2) were evoked bythesystem usingan f2/f1ratioof1.25 sothatthe strongestresponsecouldbeobtained.OnlyDPOAE measure-mentswithasignal-to-noiseratioof>6dBwereusedforthe furtherdataprocessing.Ataconstantstimulusamplitudeand time, distortion dependent otoacoustic emission data were savedatdifferentfrequencyzonesfromlowtohighfrequency between f2=0.75–8.0kHz (750, 1000, 1500, 2000, 3000, 4000,6000and8000Hz)anddistortiondependentaudiogram was attained.In DPgrammeasurements,the amplitudeofthe stimuli was equalized to 80dB SPL for both L1 and L2 (L1=L2). DPgram measurements were performed at f2frequency andmeans ofat leastthreemeasurements were noted.
2.3. Subjecteuthanization
Theratsinthreeshorttermgroupswereeuthanizedatthe4th weekandtheratsinthreelongtermgroupsweresacrificedat the 8thweekof thestudy.
Highdoseketamine(200mg/g)administrationwasusedfor euthanizingandthenintracardiacperfusionmethodwasused for fixation. In this method, 0.9% serum physiologic was infused to cardiac ventricles for tissue irrigation and 20% formaldehydewas infusedthereafterfortissue fixation.After
that,alltheratsweredecapitatedandtheirbrainswereexcised andfixedina10% formaldehydesolution.
2.4. Histopathologicalexamination
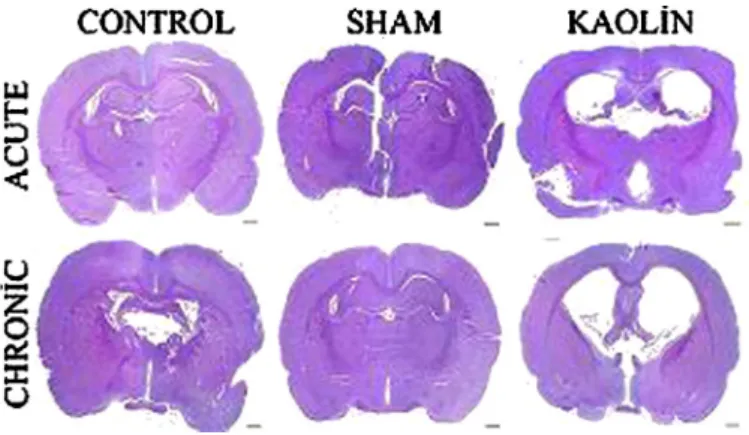
Braintissuewasexcisedfromthedecapitalizedratsandkept in10%formaldehydesolutionfor7days.Next,thebrainswere blockedandembeddedinparaffinand5mmwereobtainedat opticchiasmcoronally.Thesewere stainedwithhematoxylin andeosin(Fig.1).
2.5. Ventricularvolumemeasurements
Ventricular appendixwas markedfrom thecoronal planes crossing the optic chiasm and ventricular volume was calculatedusingthecommercialsoftware(Orbicule Macnifica-tion,v1.6.1,AppleInc.,Cupertino,CA,USA).
2.6. Statisticalanalysis
Statistical analyses were performed utilizing PASW (Predictive Analytics Software) Statistics 21.0 program. Numerical variables were expressed as medians and mini-mum–maximum values were expressed as numbers and percents.Kruskal–Wallis test was used to comparevariables betweenthegroups.Afterthistest,posthoccomparisonswith Conover’s multiple comparison test were used. Correlations wereperformedusingSpearman’scorrelationtest.Apvalueof <0.05was consideredsignificant.
3. Results
Tworatsdiedineachgroupinthesettingofthisstudyand finaldataanalysis encompassed36animals.
Ventricular volume measurements did not differ between short term control (median: 477.5mm3; min–max: 452–497mm3) and short term sham (median: 495mm3; min–max: 467–540mm3) groups (p: 0.880) but they were significantlyincreasedinthe shorttermhydrocephalusgroup (median:2148mm3; min–max:2100–2221mm3)when com-pared to short term control (p: 0.011) and short term sham (p:0.017)groups.
Inthelongterm,theshamgroup(median:1319mm3;min– max: 1227–1378mm3) had increased ventricular volumes
whencomparedtothecontrolgroup(median:487mm3;min– max:321–496mm3),butthisdifferencedidnotreachstatistical significance (p=0.522). However, long term hydrocephalus group (median: 5067mm3; min–max: 4950–5204mm3) had significantlyhigherventricularvolumeswhencomparedtothe longtermcontrol (p<0.001)andsham(p:0.048)groups.
Theshorttermcontrol,shamandhydrocephalusgroupshad similarventricularvolumeswhencomparedtotheirlongterm counterparts(p:0.88,p:0.121,p:0.324consecutively).
When DPOAE measurements were compared at all frequencies,nosignificantdifferencewasfoundbetweenshort term control and short term sham groups (p>0.05 for all frequencies).
DPOAE levels at all frequencies were significantly decreased in the short term hydrocephalus group when compared to the short term control and short term sham groups(Table1).
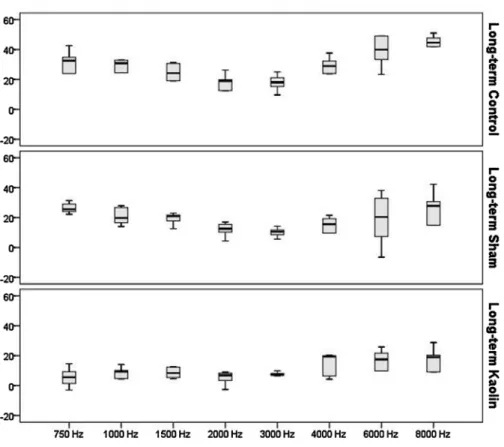
Table2showstheDPOAEmeasurementsinthe longterm groups.DPOAElevelsatallfrequencies,except1500Hz,were significantlydecreased inthelongtermhydrocephalus group when comparedtothelongtermcontrol andlongtermsham groups(Table2).Besides,longtermshamgroupalsohadlower DPOAElevelsthanthelongtermcontrolgrouphad(Table2). NosignificantdifferenceinDPOAElevelsatallfrequencies was found between short term control, short termsham and shorttermhydrocephalusgroupswhencomparedtotheirlong termcounterpartsseparately(p>0.05).
Figs.2and3showDPOAElevelsintheshortandlongterm groups.
Significant correlations between DPOAE levels and ventricular volumes were observed in the short term (Table 3) and long term (Table 4) hydrocephalus groups. Theresultsoflinearregressionanalysesofventricularvolumes andDPOAEvaluesinshortandlongtermperiodsareshownin
Table5,demonstratingsignificantassociationbetweenDPOAE measurements and ventricular volumes. Also Fig. 4 shows association between DPOAE measurements at 750Hz, 2000Hzand4000Hzfrequenciesandventricularvolumes.
4. Discussion
In this study, experimentally induced short (4 week post-blockage) and long term (8 week post-blockage) effects of hydrocephalus on DPOAE levels in an animal model were demonstrated for the first time in literature. DPOAE levels decreasedsignificantlyinbothshortandlongterm hydroceph-alusmodels andthe moststrikingfinding wasthe significant correlationsbetweenventricularvolumesandDPOAElevels. Inthisstudy,hydrocephalusmodelswerecreatedsuccessfully in both short andlong terms and these rats hadsignificantly decreasedDPOAElevelswhencomparedtotheircounterparts. Inshorttermshammodels,nosignificantchangewaspresentin termsofventricularvolumesandnosignificantdifferencewas observedbetweenshorttermshamandshorttermcontrolgroups in terms of DPOAE measurements. However, short term hydrocephalusmodels had significantly lower DPOAElevels possibly due to increased ventricular volumes which were significantlycorrelatedwithDPOAElevels.
Thethingsweredifferentinthelongterm.Therewasatrend forincreasedventricularvolumesinthelongtermshamgroup whencomparedtothelongtermcontrolgroupandlongterm hydrocephalusgrouphasthehighestventricularvolumeswhen compared toboth longterm groups. Probably, as a result of development of mild hydrocephalus in the long term sham group, we found lower DPOAE values in the long term sham group than the long term control group. In the long termhydrocephalus group, much lower DPOAE levelswere present thanbothlong termcontrol andshamgroups. These findingsare veryimportantbecausewe cansaythatDPOAE levels at high frequencies start to decline first during the development of hydrocephalus and it may be plausible that somesurgical proceduresintothe cerebellomedullary system viacisternamagnawouldcontributetoedemaorhydrocephalus inthe longterm.
In short term and long term hydrocephalus models, low and high frequency DPOAE levels both deranged probably duetotheincreaseinbothintracranialvolumeandpressure. Herein, weshowedsignificant correlationsbetween ventric-ular volumes and DPOAE levels in rats which developed hydrocephalus.Thisfindingmayhelpclinicianstodetermine the stage of hydrocephalus by a non-invasive easily applicable method, DPOAE but it should be confirmed by human studies.
In experimental animals, emission latency has been demonstrated tobe veryshort duetoshort cochlea andthus
click stimulant emissions cannot be shown because of the inabilitytodetecttheresponsetostimulants[12];however,this is not relevant for DPOAE measurements, and DPOAE measurements can be performed even in smallexperimental animals[13,14].Besidesinrodents,highleveldistortionforms during applicationof dual tonestimuli.In studiesperformed withtheseanimals,2f1 f2frequencyhadahighersensitivity for cochlear monitorization [15]. Herein, we used 2f1 f2 frequency in the light of these studies and did not get anydifficultywhile measuringDPOAEvalues.
Dynamics of CSF are very important for the hearing functionsofinnerear. EndolymphaticductconductstheCSF movements and intracranial pressure changes to endolymph anddirects perilymphtocochlearaquaductus toequalizethe pressure differences. By this mechanism, hearing functions continue permanently despite the physiological changes in CSF,butifanobstructioninthelevelofventricularductsoccurs due toexudates or fibrinoidadherences, non-communicating typehydrocephalusmaydevelop[16]andthenthechangesin CSFcirculationandpressuresmaycausetraumaticchangesin theendolymphaticsac.Bythisway,bloodflowdecreasesinthe epithelium of the sac and surrounding connective tissue and thereafter resorption capacity of the endolymphatic sac decreases [17]. Accumulating endolymph causes hydrops and blockage in the endolymphatic duct. The inequality between secretion and absorption then causes distortion in membranous labyrinthstructure.Thishypothesisissupported
Table1
DPOAEvaluesandventricularvolumesinshorttermhydrocephalus. Shorttermcontrol(dB SPL)
Shorttermsham(dBSPL) Shorttermkaolin (hydrocephalus)(dBSPL)
pvalue
Median Min–Max Median Min–Max Median Min–Max
Ventricularvolumes(mm3) 477.5 452–497 495 467to540 2148 2100to2221 *0.011 ** 0.017 *** 0.880 DPOAEfrequencies 750Hz 35.1 8.0–40.9 5.4 5.9to22.9 5.8 3.5to10.7 *0.005 ** 0.574 1000Hz 33.0 5.3–36.9 12.3 6.9to22.4 0.1 5.3to9.4 *0.003 ** 0.154 1500Hz 33.1 13.6–35.6 8.2 2.5to13.2 4.6 5.6to8.2 *0.001 ** 0.396 2000Hz 25.7 3.9–36.2 1.8 5.8to12.2 0.2 3.1to8.3 *0.012 ** 0.701 3000Hz 20.8 5.7–25.5 13 4.4to20.0 2.4 0.8to4.8 *0.002 **0.025 4000Hz 30.9 19.9–39.7 21.8 18.7to37.5 2.9 1.0to18.5 *0.001 **0.004 6000Hz 38.3 30.2–49.0 38.5 27.6to43.3 14.2 6.1to30.2 *0.007 **0.009 8000Hz 48.9 35.1–52.1 43.8 34.7to47.9 29.9 5.0to31.1 *0.028 **0.027 Note:Comparisonsbetweenshorttermcontrolvs.shorttermshamgroupswerenon-significantwhere***isabsent.
* Shorttermcontrolvs.shorttermhydrocephalus. ** Shorttermshamvs.shorttermhydrocephalus. *** Shorttermcontrolvs.shorttermsham.
clinicallyinpatientswhosufferfromhearinglossafterdecrease in CSF volume due to lumbar puncture, myelography or placementofashunt for reliefof hydrocephalus[18].In our study,we alsoshowedthenegativeeffectsofCSF circulation disturbanceoncochlearfunctionsbydemonstratingdecreased DPOAEvolumesinratswithhydrocephalus.
Intheirstudy,Malhotraetal.demonstratedhearinglossatlow frequencies due to replacement of endolymphatic hydrops insteadofthesensitivereceptorsofthecochlearbasalmembrane afterspinalanalgesia[19].Asimilarmechanismmighttakea roleinthedecrease ofDPOAEvaluesinthe shorttermsham group.Herein, decrease in DPOAEs at low frequencies was observedintheshorttermshamgroupinwhichminimalinjury tothecisternamagnawasapplied.Minimaldisturbanceinthe CSFcirculationmightcauselow-degreecochleardamageinthe shorttermshamgroup.However,intheshortterm hydrocepha-lus group, a possible Reissner membrane rupture and acute hydrops due to increased intracranial pressure might be the pathophysiological mechanism which caused decrease in DPOAEs at all frequencies. The increase in intracranial pressuresinexperimental rathydrocephalusmodels hasbeen
alreadydemonstratedbyShulyakovetal.[20].Theyhaveshown thattheintracranialpressuresincreasetoapeakat3rdto4thdays of kaolin injection andthenstay increased permanentlyafter 6days.
Therearesomelimitationsinourstudy.Althoughouterand middle ear diseases were excluded after an otoscopic examination, increased intracranial pressure could affect the motion of stapes footplate through intra-labyrinthine pressure changes, resulting in reduction of DPOAE levels. Histopathologicalexaminationofinnerearmightbeneededto confirminnereardegenerationbyhydrocephalus.Thecause of DPOAE lowering in rats with hydrocephalus might be investigatedbyhistopathologicalexaminationsofcochleaor brainstem evoked response audiometry (BERA) measure-ments which might have shown either cochlear hydrops or mechanical/chemicalinjurytoouterhaircellsthathadcaused hearing loss. Besides, CSF pressure measurements might be carriedout to showapossible relationshipwith DPOAE values, but this kind of an invasive measurement might have caused more rats to die due to its complications like infection.
Table2
DPOAEvaluesinlongtermhydrocephalus.
Longtermcontrol(dBSPL) Longtermsham(dBSPL) Longtermkaolin (hydrocephalus)(dBSPL)
pvalue
Median Min–Max Median Min–Max Median Min–Max
Ventricularvolumes(mm3) 487 321to496 1319 1227to1378 5067 4950to5204 *<0.001 ** 0.048 *** 0.522 DPOAEfrequencies 750Hz 32.5 5.1to42.7 25.6 22.2to31.4 5.6 3to14.6 *0.016 ** 0.045 *** 0.681 1000Hz 30.8 5.9to32.9 19.7 14.05to27.9 9.4 4.5to14.1 *0.023 ** 0.094 *** 0.546 1500Hz 24.2 6.4to31.2 20.9 12.5to23 8.4 4.5to12.5 *0.075 **0.049 ***0.848 2000Hz 18.9 1.6to26.3 12.6 4.4to16.9 6.9 2.6to9 *0.037 **0.154 0.511 3000Hz 18.1 9.7to25 10.5 5.6to14.2 7.1 6.6to9.9 *0.021 **0.476 ***0.112 4000Hz 28.9 23.8to37.6 15.6 7.5to21.5 19.4 4.3to20.4 *0.009 **0.784 *** 0.004 6000Hz 39.9 23.4to49.1 20.4 6.5to38.2 17.53 9.9to25.8 *0.003 **0.641 *** 0.014 8000Hz 44.6 25.7to51 27.8 17to42.3 19.03 9.1to28.8 *0.004 ** 0.468 *** 0.031 *
Longtermcontrolvs.longtermhydrocephalus.
**
Longtermshamvs.longtermhydrocephalus.
***
Fig.2.DPOAEmeasurementsinshorttermgroups.
5. Conclusion
The functional disturbances in cochlear functionsdue to hydrocephalus have been demonstrated with DPOAE measurements in this study. DPOAE measurements may be thought as an easily applicable non-invasive method in detection and follow-up of patients with hydrocephalus, since we have found a significant correlation between ventricularvolumesandDPOAElevels.Ourfindingsshould be supported with clinical studies in patients with hydrocephalus.
Disclosurestatement
Wedeclarethatnofinancialsupportorrelationshipthatmay pose aconflictof interestispresent.
References
[1] SchwambR,DalpiazA,MiaoY,GonkaJ,KhanSA.Clinical man-ifestationsofhydrocephalus:areview.NeurolClinNeurosci2014;2: 173–7.
[2] KandasamyJ,JenkinsonMD,MallucciCL.Contemporarymanagement andrecentadvancesinpaediatrichydrocephalus.BMJ2011;343:d4191.
Table3
ThecorrelationbetweenventricularvolumesandDPOAEvaluesinshortterm. DPOAEfrequencies 750Hz 1000Hz 1500Hz 2000Hz 3000Hz 4000Hz 6000Hz 8000Hz Ventricularvolume rvalue 0.57 0.36 0.67 0.321 0.49 0.64 0.71 0.92 pvalue 0.013 0.142 0.003 0.194 0.039 0.005 0.001 <0.001 Table4
ThecorrelationbetweenventricularvolumesandDPOAEvaluesinlongtermperiod. DPOAEfrequencies 750Hz 1000Hz 1500Hz 2000Hz 3000Hz 4000Hz 6000Hz 8000Hz Ventricularvolume rvalue 0.66 0.64 0.49 0.66 0.75 0.65 0.65 0.71 pvalue 0.005 0.004 0.038 0.003 <0.001 0.004 0.004 0.001 Table5
ThelinearregressionanalysesofventricularvolumesandDPOAEvaluesinshortandlongterm.
Shorttermhydrocephalus Longtermhydrocephalus
b pvalue R2 b pvalue R2 750Hz 25.4 0.027 0.27 123.56 <0.001 0.63 1000Hz 33.01 0.01 0.35 150.11 0.001 0.54 1500Hz 35.7 0.01 0.35 112.93 0.002 0.3 2000Hz 27.4 0.069 0.19 174.49 0.006 0.39 3000Hz 56.2 0.005 0.40 240.86 0.003 0.42 4000Hz 49.8 <0.001 0.723 70.1 0.133 0.14 6000Hz 48.6 <0.001 0.615 64.12 0.048 0.22 8000Hz 48.1 <0.001 0.65 59.20 0.038 0.24
[3] Lonsburry-MartinB, Harris F, Stagner B, Hawkins M, Martin G. Distortionproductotoacousticemissionsinhumans.I.Basisproperties innormallyhearingsubjects.AnnOtolRhinolLaryngol1990;47:3–13.
[4] Lonsburry-MartinB,MartinG.Theclinicalutilityofdistortionproduct otoacousticemissions.EarHear1990;11:144–54.
[5] MartinGK,OhlmsLA,FranklinDJ,HarrisFP,Lonsbury-MartinBL. Distortionproductemissionsinhumans.III.Influenceofsensorineural hearingloss.AnnOtolRhinolLaryngolSuppl1990;147:30–42.
[6] MagnanoM,AlberaR,LacillaM,GabiniA,NaddeoM,BrunoD. Impedancemeasurementasanoninvasivetechniqueforthemonitoring ofintracranialpressurevariations.Audiology1994;33:237–43.
[7] Frank A, Alexiou C, Hulin P, Janssen T, Arnold W, Trappe AE. Noninvasivemeasurementofintracranialpressurechangesby otoa-coustic emissions (OAEs) a report of preliminary data. Zentralbl Neurochir2000;61:177–80.
[8] BukiB,deKleineE,WitHP,AvanP.Detectionofintracochlearand intracranial pressure changes with otoacoustic emissions: a gerbil model.HearRes2002;167:180–91.
[9] RekateHL.Acontemporary definitionandclassification of hydro-cephalus.SeminPediatrNeurol2009;16:9–15.
[10] CrewsL,Wyss-CorayT,MasliahE.Insightsintothepathogenesisof hydrocephalusfromtransgenicandexperimentalanimalmodels.Brain Pathol2004;14:312–6.
[11] KondziellaD,EyjolfssonEM,SaetherO,SonnewaldU,RisaO.Gray mattermetabolisminacuteandchronichydrocephalus.Neuroscience 2009;159:570–7.
[12] HilgerAW,FurnessDN,WilsonJP.Thepossiblerelationshipbetween transientevokedotoacousticemissionsandorganofCortiirregularities intheguineapig.HearRes1995;84:1–11.
[13] BanfilsP,AvaP,FrancisM,TroteuxJ,NoreyP.Distortionproduct otoacousticemissionsinneonates.Normativedata.ActaOtolaryngol (Stockh)1992;112:739–44.
[14] KempDT,BrownAM.Earcanalacousticandroundwindowelectrical correlatesof2f1 f2generatedinthecochlea.HearRes1984;13: 39–46.
[15] SchmiedtR,AdamsJ.Stimulatedacousticemissionsintheearcanalof thegerbil.HearRes1981;5:295–305.
[16] Quagliarello V, Scheld WM. Bacterial meningitis: pathogenesis, pathophysiologyandprogress. NEnglJMed 1992;327:864.
[17] LawrenceM.Introductiontoinnerear(fluid)physiology.In:Paparella MM, ShumrickDA,editors.Otolaryngology. 3rded.,Philadelphia: Saunders;1991.p.199–218.
[18] NarchiP,VeyracP,VialeM.Long-termpostduralpunctureauditory symptoms:effectivereliefafterepiduralbloodpatch.AnesthAnalg 1996;82:1303.
[19] Malhotra SK, JoshiM, Grover S, Sharma SC, Dutta A. Auditory functionfollowingspinalanalgesia:comparisonoftwospinalneedles. EurJAnaesthesiol2002;19:69–72.
[20] ShulyakovAV,BuistRJ,DelBigioMR.Intracranialbiomechanicsof acuteexperimentalhydrocephalusinliverats.Neurosurgery2012;71: 1032–40.