www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Radix
saw:
a
useful
tool
for
rhinoplasty
to
correct
high
radix
Süreyya
¸eneldir
S
a,
Denizhan
Dizdar
b,∗,
Altu˘
g
Tuna
caSüreyyaS¸eneldirClinic,Istanbul,Turkey
b˙IstinyeUniversity,FacultyofMedicine,Bahc¸elievlerMedicalParkHospital,DepartmentofOtolaryngology, ˙Istanbul,Turkey cPrivateOffice,Frankfurt,Germany
Received13February2019;accepted26June2019 Availableonline7August2019
KEYWORDS Rhinoplasty; Radix; Nose
Abstract
Introduction:Themostdifficultaspectofradixloweringisdeterminingthemaximumamount
ofbonethatcanberemovedwithosteotomes;here,wedescribeuseofaradixsaw,whichis anewtoolfordeterminingthisamount.
Objective:Inthisstudy,wedescribeuseofaradixsaw,whichisanewtooltoreducetheradix.
Methods:Themedicalchartsof96patientsundergoingsurgerytolowerahighradixbetween
2016and2017 were assessed retrospectively.All operations were performedby thesenior surgeon.Outcomeswereassessedbycomparingpreoperativephotographswiththemostrecent follow-upphotographs(minimumof6monthspostoperatively).Thephotographswerealltaken usingthe same imaging settings,andwith consistent subjectdistance andangulation. The photographsweresubsequentlyanalysedbyauthors.
Results:Thestudypopulationconsistedof96patients(70women, 26men)whounderwent
rhinoplastybetween 2016and2017. The mean age ofthe patients was 28.8 years(range: 18---50years)andthemeanclinicalfollow-upperiodwas1.8years.Nopatientrequiredrevision surgeryduetoradixproblems,andtherewerenocaseswithunwantedbonefragmentsorradix asymmetry.Theswellingandoedemaseenimmediatelyaftersurgerysubsidedafteranaverage of7---10days.
Conclusion:In conclusion, a radixsaw can be used for rhinoplasty requiring delicate bone
removalinpatients withahighradix.LevelIV:Evidenceobtainedfrommultipletimeseries withorwithouttheintervention,suchascasestudies.Dramaticresultsinuncontrolledtrials mightalsoberegardedasthistypeofevidence.
© 2019 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](D.Dizdar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
https://doi.org/10.1016/j.bjorl.2019.06.013
S.¸eneldir,S D.DizdarandA.Tuna
Introduction
The radix is a depression at the root of the nose, which definesthenasalrootandtheoriginof thenosefromthe pointoftheglabella.Theradixextendsinferiorlyfromthe nasiontothelevelofahorizontallinepassingthroughthe lateralcanthi,andsuperiorlyfromthenasionforan equiv-alentdistance.1
Radixlocalisationcanbeperformedusingseveral meth-ods.Theradixdefinesthemostconcavepartofthecephalic dorsum. The normal distance from theradix tothe inner canthus is 6mm and the distance between the corneal planeandtheradixplaneisabout9---14mm.1---4Radix
posi-tionisevaluatedinthecephalocaudalandanteroposterior axes.Thenormalpositionoftheradixinthecephalocaudal axis isbetween thelevel ofthe upperlid marginand the supratarsalfoldwiththeeyeslookingstraightahead.Lower andhigherradixpositionsinbothaxesnotonly affectthe aestheticappearanceofthe nose,butalsothenasalbase andapparentlength.4
Thepositionoftheradixsignificantlyinfluencesthe over-allbalanceofthenasalprofile;itimpactsthenasalcontour, length,angulationandheight.
Alowradixpositionresultsinreducednasalprojection, increased tip projection, and a nasal base that appears largerthanitsactualsize.Ahighradixmaybeseeninsome patientswhoseekrhinoplasty.Inpatientswithahighradix, the radix projection is above the normal limit, such that thenoseappears excessivelylong.Intheprofileview, the nose-to-foreheadanglemaybewide,suchthatthenoseand forehead appear continuous, an effect known as ‘‘avatar nose’’.Alternatively,thenasalbonesmaybesituatedapart fromeachother, leadingtotheappearanceofexcessively widespacingoftheeyes.
The most difficult aspect of radix lowering is deter-mining the maximum amount of bone that can be removed with osteotomes; piezoelectric and classical osteotomies are widely used.5---7 Here we describe use of
a radix saw, which is a new tool for determining this amount.
Methods
Thisretrospectivecaseseriesstudywasperformedin accor-dance withthe Declaration of Helsinki. Informed consent wasprovided by all patients following institutional ethics board approval (Istanbul Education and Research Hospital EthicsBoardno:1538).The medicalcharts of96 patients undergoingsurgerytolowerahighradixbetween2016and 2017wereassessedretrospectively.Alloperationswere per-formedbytheseniorsurgeon.
Outcomes were assessed by comparing preoperative photographs with the most recent follow-up photographs (minimum of 6 monthspostoperatively). The photographs were alltaken usingthe same imagingsettings, andwith consistent subject distance and angulation; from 1.5m; frontal, 45 degree, profile, basal angles. A Nikon d800 camera was used, with 100mm, f14, macro lens, ˙ISO 100, double paraflash from 1.5m. The photographs were
subsequently analysed by the senior author (Figs. 1---3). The outcomes were also assessed by asking the patients’ opinions on their own radix position and shape. Radix asymmetryandunwantedbonefragmentswereevaluated. The postoperative oedema was assessed with physical examination.
Patients wereselected from a database of rhinoplasty cases containing information regarding patient demo-graphics,preoperativeanalyses,operativetechniques,and postoperativeoutcomesandcomplications.
Radixsaw
Theradixsawwasmadeofhardenedstainlesssteelandhas atipwidthof4mm,depthof7mm,gearangle of90◦ and shanklengthof12cm.Theheadoftheinstrumentwassmall, suchthatit didnotrequireexcessivesofttissueelevation anddidnotcausebruisingorreddeningoftheskin(Fig.4). Thetoolwascreatedbytheseniorauthor.
Surgicaltechnique
In a sitting posture on the operatingtable (to avoid any influence of gravity), the actual radix positionand depth of thedesired position wasmeasured and marked onthe skin.Aftergeneralwithinfiltrationanaesthesia,thedorsum was reached by supraperichondrial dissection (via subcu-taneous dissection) with an inverse V-shaped columellar incisionif open technique was used or the dorsum could also be reached via intercartilagineous incision. For both openandclosedtechniquetheoperativestepswereas fol-lows.Theskinandsofttissueenvelopeweredissectedand raisedinthesupraperichondrialplanetotherhinion. Subse-quentsubperiostealelevationwasperformedoverthenasal bones.
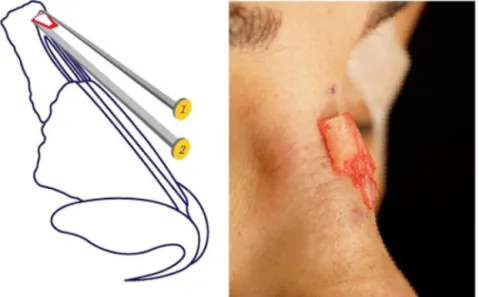
Theradixanddorsumoperationconsistedofthreestages inpatientswithahighradix:(1)initialworkonany exist-ing hump in the nasal dorsum; (2) lowering of the radix; (3)removalofanyresidualhump followingradix lowering (Fig.5).
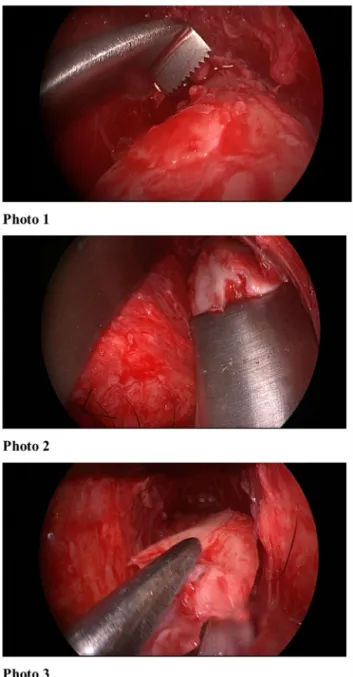
Itwasimportanttopayattentiontotheorderofsteps. First the existing primary hump was lowered using stan-dard ostetomes or rasps. Than the ideal radix position was determined by making a straight and non-traumatic incisioninthenasalbone,whichrequiredfinewrist move-ment, usinga radix sawin the vertical plane. The depth of the radix was adjusted by varying the bone incision depthwiththeradixsaw,uptoamaximumdepthof7mm (i.e.thelengthofthesaw).Nopressureshouldhavebeen applied to the saw at this point. However, the borders of the medial canthus could be palpated and supported laterally.
Thus, the upper limit of the bone tobe removed was determinedandcut.Then,astraightosteotomewasplaced intheradixareaata40/60(Fig.6)degreeangleandabone incisionwasmade that reaches the transverse osteotomy above.Aftertheincisionswerefinished,thewedge-shaped bonewasreleased.Controlledincisionsandresectionwere performedwiththeuseofanosteotomeandasaw.If
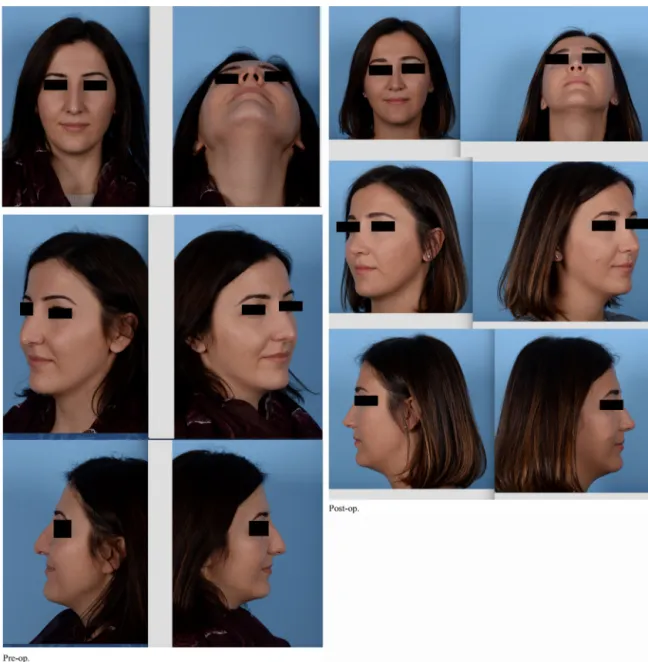
neces-Figure1 Patient1.Preandpost-opphotos.
sarymorebonecouldberemovedwitharasp.Atthispoint theradixsawcouldalsobeusedasarasp.Carewasrequired toavoid over-resection. Reduction shouldhave been per-formed using the saw as a rasp tool, to ensure minimal resection,irregularityanddorsalreduction.Inthismanner, theradix sawcouldbeusedasan alternativetoafile,to avoidscrapingoftheradixinthecaudaldirectionandensure radix alignment according to the pre-determined dorsum height(SupplementaryMaterial1)(Fig.7).
Aftertheradixanddorsumweremodifiedasdesired,the operations is continued with standart lateral osteotomies andtipplasty.
Results
Thestudypopulationconsistedof96patients(70women,26 men)whounderwentrhinoplastybetween 2016and2017. Tenpatientswereoperatedwithclosedtechnique;other86 wereoperatedwithopen technique.Themeanageofthe patientswas28.8years(range:18---50years)andthemean clinicalfollow-upperiodwas1.8years.Themeanlong-term follow-upperiodwas1.6years.Directfollow-upwas avail-ablefor96 patientsafter1 year;theywereasked ifthey weresatisfiedwiththeradixpointsandtheywereallhad physicalexaminationoftheradixarea.
S.¸eneldir,S D.DizdarandA.Tuna
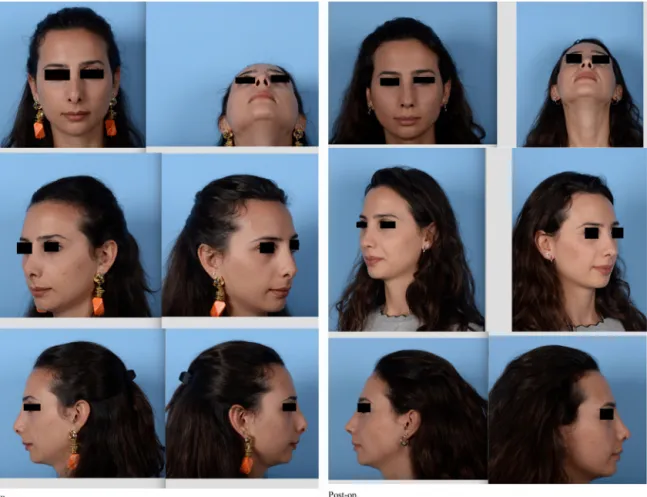
Figure2 Patient2.Preandpost-opphotos.
Over the2yearstudyperiod95patientsweresatisfied withtheradixpointsandphysical examinationshowedno problem in the radix area; 1 patient (<1%) presented to the author with complaints about the bony dorsum near theradix.Thecauseofdissatisfactioninthispatientwere minimalbonyprominences.
Twopatientshadrevisionsurgeriesduetotipproblems. Theserevisionswereduetotipgraftvisibilityandtip asym-metry.Theoedemaandswellingwasevaluatedwithphysical examination. The swelling andoedema seen immediately after surgery subsidedafter an average of 7---10 days.No undesirableoedemawasobservedafter10days postopera-tively.
Discussion
Twoparametersmust beknowntoidentifytheidealradix position:
1) Theidealverticalpositionoftheradix:thisisthepoint atwhichahorizontallinedrawnfromthemiddleofthe uppereyelidintersectsthecenterlineofthenose.The radix positionaffects nose length: whereas a caudally locatedradixresultsinashortnose,inpatientswitha morecephalicradixpositionthenosewillbelong.The formeroccursmorefrequently.
Figure3 Patient3.Preandpost-opphotos.
2) Theidealradixprojection(height)intheanterior coro-nal is 9---14mm. Radix projection is important as it directlyaffectstheextentofnasalprojection.Theradix anddorsum heightsmust bein balance.To establish a goodbalance,theradixheight mustfirstbeideal,i.e. 9---11mminwomen.Menrequireastrongerdorsum,and theradixheightmustbeattheupperlimitofidealfor patientswiththickerskin.8,9
Mosttechniquesusedtoreducetheradixfocuson low-eringthenasalbonesandtheresultslargelydependonthe statusofthenasalskin, subcutaneoustissuesandmuscles (suchasthe procerusandcorrugator supercilii).A combi-nationofthickskinandtissuesoftnessmakesitdifficultto precisely determinethe extent of radixreduction or aug-mentationrequired.
Allmeasurementsoftheradixshouldbemadewhilethe patientisinasittingposition,andplanningshouldbe per-formed with this in mind.When measurementsare made withthepatientlyingdown,gravity cannegativelyaffect theradixposition.
Various techniques have been proposed for removal of bone fromthe radix region,including rasping, osteotomy anduseof aburr.10---13 Osteotomyis thepreferredmethod
for dealing with a high radix accompanied by a
moder-resectionofthebonewithoutresidualbonyparticles,while drawbacks include a risk of over-resection and asymmet-rical bone removal. It is also possible toachieve a clear breakwith osteotomy. Raspingcan facilitate step-by-step removal of excess bone, but it causes severe trauma to the soft tissue and is not suitable for cases with a very highradix. Anotherdisadvantageofrasping isits impreci-sionregardingradixposition.Variousosteotomeshavebeen usedtodeepenthenasofrontalangle.Flatosteotomesused togetherwitharadixsawhavebeen suggestedtoweaken thebonyroot.QuislingandRubinosteotomesdonothave thesamehighdegreeofaccuracyassociatedwith percuta-neousosteotomy.
Guyuronwasthefirsttouseaguardedburrfordeepening oftheradix,whichmakesconservativeboneremoval possi-ble.Thecomplicationsassociatedwithuseofaburrinclude arisksofseromaandpenetrationofthefrontalsinus.12
Piezoelectricsystemswhichareusedcommonlycan be usedtoreduceradixbut,becausetheareamustbewashed withsaline,thatmayaffecttheperceptionoftheradixand oedemacanoccuraftertheuseofpiezo.13
Thesofttissueoftheradixoccasionallyrequires atten-tion. In such cases, it is recommended to perform the dissectionsuperficial to themuscle and removethe bone withthe procerusmusclestillattached.Itis necessary to exertconstantpressureontheareaforafewdaystoavoid
S.¸eneldir,S D.DizdarandA.Tuna
Figure4 Radixsaw.
haematoma,fibrosisandscar formation.Theuseofa spe-ciallydesignedsplintmaybeconsidered.
Anumberofrhinoplastysurgeonshavedeveloped tech-niques to lower the radix, but no procedures capable of thinning the skin envelope over the radix have yet been reported.Althoughminorreductionsinthecaudalportion oftheradixmaybeachievedusingarasp,substantial reduc-tion requires a more aggressive approach. The use of an osteotometoperform wedgeresectionof the nasofrontal bones may effectively reduce the projectionof the radix and deepen the nasofrontal angle. If theradix is overde-veloped and thus makes a significant contribution to the nasofrontal angle, a guarded burr can be used toreduce thebone.Guyuronsuggestedthattheboneheightmustbe reducedbyatleast4---5mmtoaffordavisiblereductionof 1mm. However, thisis not possible in allpatients due to variationsinfrontalboneanatomy.Removalofnasofrontal boneattheleveloftheradixleadstoavisiblereductionin boneheightofonlyapproximately25%.14---16
Nasal skin thickness differs among the various nasal regions.Giventhatoverprojectionintheareaoftheradix maynotbeattributableonlytobone,manipulationsofonly thenasalbonesmaynotyieldanidealsolution.17
Figure5 Stepsofprocedure.
Theradixsawhasanumberofadvantages;forexample, itis possible to markthe upper limitwith respecttothe amount of bone toberemoved and,by usingosteotomes
Figure7 Per-opendoscopicview.
thereafter,thebonecanbesmoothlyremovedandtheideal radix positionpreciselydetermined. Use ofa radix sawis associated with less oedema and swelling,as the cutting of the bone can be precisely controlled,in additionto a reductionin bonyirregularitiesand,in caseswithasmall hump,directremovalthereof.
Conclusion
Aradix sawcan beusedforrhinoplastyrequiring delicate boneworkinpatientswithahighradix.
TheEnglishinthisdocumenthasbeencheckedbyatleast twoprofessionaleditors, both native speakersof English. For a certificate, please see: http://www.textcheck. com/certificate/PaBdx8.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
A.
Supplementary
data
Supplementary data associated with this article can be found, in the online version, at doi:10.1016/ j.bjorl.2019.06.013.
References
1.SteigerJD,BakerSR.Nuancesofprofilemanagement:theradix. FacialPlastSurgClinNorthAm.2009;17:15---28.
2.GuyronB.Precisionrhinoplasty.PartII:prediction.Plast Recon-strSurg.1988;81:500---5.
3.LazovicGD,DanielRK,JanosevicLB,KosanovicRM,ColicMM, KosinsAM.Rhinoplasty:thenasalbones---anatomyandanalysis. AesthetSurgJ.2015;35:255---63.
4.Saban Y, Daniel RK, PolselliR, Trapasso M,Palhazi P.Dorsal preservation:thepushdowntechniquereassessed.AesthetSurg J.2018;38:117---31.
5.Gerbault O, Daniel RK, Kosins AM. The role of piezoelec-tric instrumentation in rhinoplasty surgery. Aesthet Surg J. 2016;36:21---34.
6.Tirelli G, Tofanelli M, Bullo F,Bianchi M, Robiony M. Exter-nal osteotomyinrhinoplasty:piezosurgeryvsosteotome.Am JOtolaryngol.2015;36:666---71.
7.RobionyM,PoliniF,CostaF,ToroC,PolitiM.Ultrasound piezo-electricvibrationstoperformosteotomiesinrhinoplasty.JOral MaxillofacSurg.2007;65:1035.
8.DanielRK.Rhinoplasty.Anatlasofsurgicaltechniques.1sted. NewYork,NY:Springer;2002.p.27.
9.SheenJH,SheenAP.Aestheticrhinoplasty.2nded.StLouis,MO: Mosby;1987.p.103---7.
10.Mowlavi A, Meldrum DG,Wilhelmi BJ.Implications for nasal recontouring: nasion position preferences as determined by a survey of white North Americans. Aesthetic Plast Surg. 2003;27:438---45.
11.TardyME.Rhinoplasty:theartandthescience.Philadelphia, PA:WBSaundersCo.;1997.p.103---8.
12.GuyuronB.Guardedburrfordeepeningofnasofrontaljunction. PlastReconstrSurg.1989;84:513---6.
13.Tas¸kınÜ,BatmazT,ErdilM,AydınS,Yücebas¸K.Thecomparison of edema and ecchymosis after piezoelectric and conven-tional osteotomy in rhinoplasty. Eur Arch Otorhinolaryngol. 2017;274:861---5.
14.BeckerDG,PastorekNJ.Theradixgraftincosmeticrhinoplasty. ArchFacialPlastSurg.2001;3:115---9.
15.Cohen JC, Pearlman SJ. Radix grafts in cosmetic rhino-plasty:lessonsfroman8-yearreview.ArchFacialPlastSurg. 2012;14:456---61.
16.JohnsonCMJr,AlsarrafR. Theradixgraftincosmetic rhino-plasty.ArchFacialPlastSurg.2001;3:120---1.
17.TardyMEJr,Becker D,WeinbergerM.Illusionsinrhinoplasty. FacialPlastSurg.1995;11:117---37.