w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
The
effectiveness
of
Kinesio
Taping
on
pain
and
disability
in
cervical
myofascial
pain
syndrome
Saime
Ay
a,∗,
Hatice
Ecem
Konak
a,
Deniz
Evcik
b,
Sibel
Kibar
aaUfukUniversity,SchoolofMedicine,DepartmentofPhysicalMedicineandRehabilitation,Ankara,Turkey
bAnkaraUniversity,HaymanaVocationalHealthSchool,DepartmentofTherapyandRehabilitation,Ankara,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received18June2015 Accepted20December2015 Availableonline10May2016
Keywords:
Myofascialpainsyndrome KinesioTaping
Disability Pain
a
b
s
t
r
a
c
t
Objective:TheaimofthisstudywastoinvestigatetheeffectivenessofKinesioTapingand shamKinesioTapingonpain,pressurepainthreshold,cervicalrangeofmotion,and dis-abilityincervicalmyofascialpainsyndromepatients(MPS).
Methods:Thisstudywasdesignedasarandomized,double-blindplacebocontrolledstudy. Sixty-onepatientswithMPSwererandomlyassignedintotwogroups.Group1(n=31)was treated withKinesioTapingandgroup2(n=30)wastreatedshamtapingfivetimesby intervalsof3daysfor15days.Additionally,allpatientsweregivenneckexerciseprogram. Patientswereevaluatedaccordingtopain,pressurepainthreshold,cervicalrangeofmotion anddisability.PainwasassessedbyusingVisualAnalogScale,pressurepainthresholdwas measuredbyusinganalgometer,andactivecervicalrangeofmotionwasmeasuredby usinggoniometry. Disabilitywasassessedwiththeneckpaindisability indexdisability. Measurementsweretakenbeforeandafterthetreatment.
Results:Attheendofthetherapy,therewerestatisticallysignificantimprovementsonpain, pressurepainthreshold,cervicalrangeofmotion,anddisability(p<0.05)inbothgroups. Alsotherewasastatisticaldifferencebetweenthegroupsregardingpain,pressurepain threshold,cervicalflexion-extension(p<0.05);exceptcervicalrotation,cervicallateral flex-ionanddisability(p>0.05).
Conclusion: ThisstudyshowsthatKinesioTapingleadstoimprovementsonpain,pressure pain thresholdandcervicalrangeofmotion,butnotdisabilityinshorttime.Therefore, KinesioTapingcanbeusedasanalternativetherapymethodinthetreatmentofpatients withMPS.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](S.Ay). http://dx.doi.org/10.1016/j.rbre.2016.03.012
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Efetividade
do
kinesio
taping
na
dor
e
incapacidade
na
síndrome
dolorosa
miofascial
cervical
Palavras-chave:
Síndromedolorosamiofascial Kinesiotaping
Incapacidade Dor
r
e
s
u
m
o
Objetivo: Investigaraeficáciadokinesiotapingedotapingplacebosobreador,limiardedor àpressão,amplitudedemovimentocervicaleincapacidadeempacientescomsíndrome dolorosamiofascial(SDM)cervical.
Métodos: Ensaioclínicorandomizadoduplo-cegocontroladoporplacebo.Foramalocados emdoisgrupos,aleatoriamente,61pacientescomSDM.Ogrupo1(n=31)foitratadocom kinesiotapingeogrupo2(n=30)foitratadocomtapingplacebocincovezesemintervalosde trêsdias,durante15dias.Alémdisso,todosospacientesforamsubmetidosaumprograma deexercíciosparaopescoc¸o.Ospacientesforamavaliadosemrelac¸ãoàdor,aolimiarde doràpressão,àamplitudedemovimentocervicaleàincapacidade.Adorfoiavaliadacoma escalavisualanalógica,olimiardedoràpressãofoimedidocomumalgômetroeaamplitude demovimentocervicalativafoimensuradacomagoniometria.Aincapacidadefoiavaliada comoNeckPainDisabilityScale.Asmensurac¸õesforamfeitasantesedepoisdotratamento. Resultados: Nofimdotratamento,houvemelhoriaestatisticamentesignificativanador,no limiardedoràpressão,naamplitudedemovimentocervicalenaincapacidade(p<0,05) emambososgrupos.Tambémhouveumadiferenc¸aestatisticamentesignificativaentreos gruposemrelac¸ãoàdor,aolimiardedoràpressãoeàflexão-extensãocervical(p<0,05); nãohouvediferenc¸anarotac¸ãocervical,flexãolateralcervicaleincapacidade(p>0,05). Conclusão: Okinesiotapinglevaàmelhorianador,nolimiardedoràpressãoenaamplitude demovimentocervical,masnãonaincapacidadeemumcurtoperíodo.Portanto,okinesio tapingpodeserusadocomoummétododeterapiaopcionalparaotratamentodepacientes comSDM.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Myofascialpainsyndrome(MPS)isoneofthemostcommon musculoskeletalproblemsandisanimportantcauseof mor-bidityinadults.MPSisaconditioncharacterizedbychronic painandassociatedwithtriggerpointsinoneormore mus-cles,tautbands,characteristicreferredpain,andlocaltwitch response.Patientsrefertohospitalswithlocalorreferredpain, muscleweakness,tightness,limitedmobility,weakness, ten-derness,autonomicdysfunctionsandlocaltwitchresponsein theaffectedmuscle.1,2
TheexactetiologyofMPSisnotfullyunderstood;therefore, thetreatmentisfocusedondecreasingpain,improving mus-clestrengthandprovidinggoodposture.Patients’education andtrainingprograms,nonsteroidalanti-inflammatorydrugs (NSAID),localinjections,physicaltherapy,acupunctureand exerciseprogramsarethemostcommontreatmentmethods.1
KinesioTaping(KT)hasbeen increasingly usedin mus-culoskeletal conditions and sports injuries. This technique was developed in Japan by Kase and recently it became very popular in pain treatment.3,4 Kinesio Tape is a thin,
light, and elastic material which does not restrict the jointmovement.4,5 Itisfoundtobeeffectiveindecreasing
pain and muscular spasm,increasing the range ofmotion (ROM),improvinglocalbloodandlymphcirculations, reduc-ing edema, strengthen weakened muscles, control joint
instability and postural alignment.6–8 Although the exact
mechanisms of KT is not understood, sensorimotor, pro-prioceptivefeedbackmechanisms, inhibitoryandexcitatory nociceptivestimuli,mechanicalrestraintwere explainedas underlyingmechanisms.4,6,7Inthisdouble-blinded,
random-ized placebo controlled study, we aimed to compare the efficacyofKTandplaceboKTmethodsonpain,pressurepain threshold,ROManddisabilityinpatientswithMPS.
Materials
and
methods
Seventy-threepatients(50female,23male)withcervicalMPS involvingtheupperneckandlevatorscapulamusclereferred toouroutpatientclinicwereincludedinthestudy.The diag-nosisofMPSwasbasedonthecriteriadescribedbyTravell and Simons (5 major and minimum 1 minor criteria are requiredforclinicaldiagnosis).9Thepatients’inclusion
crite-riawerepresenceofatleastoneactivetriggerpointlocated in levator scapulamuscle, ages greater than 18 years, and symptomdurationofatleast3months.Theexclusioncriteria werediagnosisoffibromyalgiasyndrome,cervicaldisclesion, radiculopathy,myelopathy,recent triggerpoint injectionor participatinginaphysicaltreatmentprogramwithinthelast 6months,neurologicandinflammatorydiseases,pregnancy orhistoryofneckandshouldersurgery.
Afterphysicalexamination,fullbloodcount,erythrocyte sedimentationrate,C-reactiveprotein,andbiochemical mark-erswereevaluated.
This study was prospective, randomized, placebo-controlleddouble-blindtrial.Beforetreatment,allparticipants wereinformedaboutthestudyandsignedwritteninformed consent.ThestudywasapprovedbytheUniversityofUfuk HumanResearchEthicsCommittee.
Randomization
Patientswere randomlyassigned into two groupsby num-beredenvelopesmethod.Thegroup1andgroup2noteswere putintototheclosedenvelopesseparately,andeachpatient randomlychoseanenvelopeandgaveittothe physiothera-pist.Bothpatientsandtwoexaminingphysicianswereblinded totreatmentallocation.Onlythephysiotherapistwhoapplied thetherapywasawareoftheprocedureandphysiotherapist recordthepatientnamesandtheirgroups.
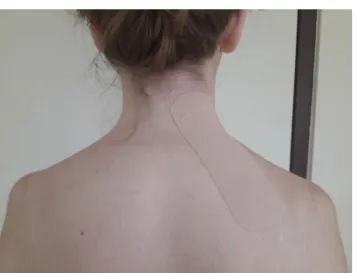
Group1patients(n=31)were treatedwith KinesioTape (KinesioTexGold,2in×103.3ft)suggestedbyKaseetal.five timesbyintervalsof3daysfor15days.Tapingwasperformed byaphysiotherapistwhoiscertifiedforthismethod.The mus-cleinhibitiontechnique which wasdescribed byKasewas used.Weappliedthetapingtolevatorscapulamuscle.The shoulderwasdepressedandneckwasinlateralflexionand rotation position tothe opposite side. A 15–20cm long “I” stripwasused.Applicationstartedfromthesuperior scapu-larangle.Initialportionofthetapewasstretchedmaximum 4–5cm andthen it wasstickedon the muscleorigowhich wasatthelevel of1–4 thoracictransverseprocess without stretching5(Fig.1).
Group2patients(n=30)weretreatedwithshamtapingfive timesbyintervals of3 daysfor15 days. Shamtaping was appliedwithan“I”stripofthesamematerialonineffective partsofthemusclewithoutatensionwiththeneckinneutral position(Fig.2).
Additionally, all patients received a home-based exer-cise program including isometric-isotonic neck exercises and back extensor stretching exercises everyday for two weeks.
Fig.1–KinesioTapingtechnique.
Fig.2–ShamKinesioTapingtechnique.
No analgesic drugsor NSAIDswere allowed during the treatmentprocess.
Clinicaloutcomes
Patients were evaluated according to pain, pressure pain threshold,cervicalROManddisability.
Pain
Painwasassessedbyusingavisualanalogscale(VAS,0–10cm; 0meansnopain,10meansseverepain).
Pressurepainthreshold
Pressurepainthreshold(PPT)onthetriggerpointwas mea-sured with an algometer (Algometer Commander, JTECH Medical,Utah).Themeasurementwastakenthreetimesand themeanaveragevaluewasrecorded.
Cervicaljointrangeofmotion
TheactiveROMofcervicaljoint(flexion,extension,right–left flexionandrotation)wasmeasuredusingagoniometerwhen thepatientwasinsittingposition.
Disability
Disability was measured byusing the Neck Pain Disability Scale(NPDS).Turkishversionofthisscalewasfoundvalidand reliable.Thequestionnaireconsistsof20itemsandmeasures neckmovements,painintensity,effectofneckpainon emo-tion factors,and interferencewithdailylifeactivities.Each sectionisscoredona0–5ratingscaleandtotalscoreranges from0to100.10
Statisticalanalysis
Themeansandstandarddeviationsweregivenasdescriptive statistics. All data for normality were tested by using the Kolmogorov–Smirnov test. Per-protocol analysis was used for the comparison of treatment groups. For determining the difference before and after treatment for all groups, non-parametric Wilcoxon test was used. To compare the
MAS (n=73)
Analisados (n=31) Lost to follow-up (n=5)
Discordance of therapy in 4 patients, allergic reaction in 1 patient Group 1 (n=36) Kinesio tape Lost to follow-up (n=7) Discordance of therapy in 6 patients, allergic reaction in 1 Group 2 (n=37)
Sham kinesio tape
Analyzed (n=30)
Allocation
Analysis 2 weeks Follow-Up
Randomized
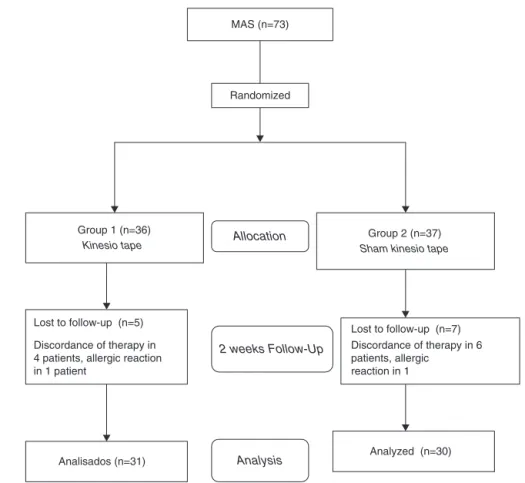
Fig.3–Flowdiagramshowingofpatientsthroughtheclinicalstudy.
differencesbetween twogroups, the Mann–WhitneyU test wasused.Alevelofsignificanceofp<0.05wasaccepted.All analyseswere performedusing theSPSS forWindows18.0 softwareprogram.
Results
Thirty-sixpatientsingroup1(27femalesand9males)and37 patientsingroup2(30femalesand7males)withMPSwere includedthestudy.Afterrandomization,4patientsinGroup 1and6patientsinGroup2droppedoutbecausetheycould notattendthefollow-upprogramregularlyinthestudy.Then, onepatientfromGroup1andonepatientGroup2dropped out because allergic reaction occurred. Sixty-one patients completedthestudyandnosideeffectshadbeenobserved (Fig.3).
Table1showsthedemographicandclinicalpropertiesof theGroup1andGroup2.Nostatisticallysignificantdifferences weredetectedbetweenthegroupsatbaselinevalues(p>0.05) exceptNPDS(p<0.05).
Theresultsoffullbloodcount,erythrocytesedimentation rate,C-reactiveproteinandbiochemicalmarkerswerewithin normalrangesforbothgroups.
Aftertwoweeksfollowup,therewerestatistically signif-icantimprovementsinbothgroupsregardingVAS,PPT,ROM andNPDS(p<0.05)(Table2).
Table1–Demographicandcliniccharacteristicsofthe patients. Group1 (n=31) Group2 (n=30) p Age(years) 44.80±17.19 44.10±17.45 0.76 Gender (female/male) 22/9 23/7 0.61 Durationofpain (month) 14.48±4.99 13.50±2.76 0.97 VAS 5.00±2.00 4.56±2.17 0.38 PPT(N) 61.29±8.92 61.73±5.35 0.61 NPDS 49.77±21.37 39.80±12.51 0.05a
VAS,visualanalogscale;PPT(N),pressurepainthreshold,Newton; NPDS,NeckPainDisabilityScale.
a p<0.05.
After the treatment, statistical significant differences wereobservedinVAS,PPT,cervicalflexion-extensionvalues (p<0.05)between thegroups. Howeverno differences were foundincervicalrotation,lateralflexionandNPDS(p>0.05) (Table2).
Discussion
Myofascialpainsyndromeisthemostcommonlyoccurring musculoskeletaldisorders seenbyphysiatrists. Thereisno acceptedstandardtreatmentprogramforMPS.Themainissue
Table2–Comparisonoftheassessmentparametersinbothgroupsandbetweenthegroups. Group1(n=31) (mean±SD) Group2(n=30) (mean±SD) p
Variable(independent)VAS
Baseline 5.00±2.00 4.56±2.17 Posttreatment 2.35±1.99 3.93±1.96 0.004b p 0.000a 0.000a PPT Baseline 61.29±8.92 61.73±5.35 Posttreatment 78.09±7.18 71.43±10.25 0.003b p 0.000a 0.000a Cervicalflexion Baseline 64.58±7.66 59.86±7.01 Posttreatment 71.90±7.54 64.86±6.79 0.001a p 0.000a 0.001a Cervicalextension Baseline 51.93±12.83 44.83±12.42 Posttreatment 55.96±13.63 47.20±14.21 0.015 p 0.007b 0.003b
Rightlateralflexion
Baseline 39.64±13.77 33.83±5.52
Posttreatment 42.61±14.78 35.93±5.80 0.357
p 0.001a 0.003b
Leftlateralflexion
Baseline 40.93±14.4 33.83±5.52 Posttreatment 43.90±14.94 42.43±17.97 0.390 p 0.000a 0.001a Rightrotation Baseline 60.58±11.58 61.36±12.31 Posttreatment 64.74±11.04 63.60±9.55 0.348 p 0.001a 0.006b Leftrotation Baseline 63.09±12.43 67.53±8.24 Posttreatment 66.83±13.01 67.93±7.97 0.907 p 0.001a 0.10 NPDS Baseline 49.77±21.37 39.80±12.51 Posttreatment 35.67±20.27 36.10±12.16 0.558 p 0.000a 0.000a
VAS,visualanalogscale;PPT,pressurepainthreshold;NPDS,NeckPainDisabilityScale;SD,standarddeviation. a p<0.001.
b p<0.05.
intheMPStreatmentistoprovidepainreliefontriggerpoints, improvingdisabilityandincreasingcervicalmotion.1,2
Kine-sioTapingisanewalternativetechniqueusedinMPS.3,4This
study was planned as a randomized double-blind placebo controlled study in which efficacy of KT and placebo KT methodsonpain,PPT,ROMofcervicaljointanddisabilityin MPStreatment.After2weeksoftreatment,all assessment parametersshowedstatisticallysignificantimprovementsin bothKTandshamgroups.Therewasastatisticaldifference between the groups regarding VAS, PPT, cervical flexion-extension,exceptcervicalrotation,cervicallateralflexionand NPDS.
Althoughtherearealotofstudiesintheliteratureaboutthe effectoftapingonmusculoskeletalsystemandsportinjuries, therearelimitednumberofrandomizedcontrolledstudieson
MPS.3,11,12However,thereisnoplannedrandomized
double-blindplacebocontrolledstudyinwhichefficacyofKTinpain, PPT,ROMofcervicaljointanddisabilityinMPStreatment.A casereporthassuggestedthatKTmaybebeneficialforthe treatmentofapatientwithshoulderpainofmyofascial ori-gin.Theyobservedsignificantimprovementinthefunctional testsactiveshoulderrangeofmotionandtherewasnochange intheVAS.13 Inarandomizeddouble-blindstudywithMPS
includedfiftypatients,theefficiencyofKTwascomparedwith dryneedlingandsignificantdecreaseinpain,PPTand disabil-itywasobserved.TheyfoundthatKTwasatleastaseffective asdryneedlinginthetreatmentofMPS.14Hernandezetal.
comparedtheeffectivenessofKTandcervicaltrust manipu-lationinmechanicalneckpainwith36patients;theyobserved KTorcervicaltrustmanipulationleadstosimilarreductionin
painseverity,disabilityandincreasesinROM.15Although
Gon-zalezetal.foundanimprovementinpainandROMinpatients withacutewhiplashinjurywithKT,theseweresmallandnot clinicallymeaningful.8Inourstudy,KTgroupshowed
statis-ticallysignificantimprovementsregardingVAS,PPT,ROMand NPDS.Althoughsignificantimprovementswereobservedin pain,PPT,cervicalflexion-extension,comparedtotheplacebo group,therewasnochangeincervicalrotation,cervicallateral flexionandNPDS.
Multipletheorieshavebeenproposedtoexplainthe mech-anismsof KT, including enhance proprioception, cutaneus mechanoreceptors, improved blood and lymphatic circula-tion,reducedpainseverity,realignmentofjoints,assistthe posturalalignmentandrelax theoverusedmuscles.4,7,11 As
aresultofKT,weobservedthatpain,PPT,ROMand disabil-itymeasures showedstatisticallysignificant improvements inKTgroup.Stimulatingthegatecontrolmechanismresults adecreaseinpainthroughtheincreaseinafferentfeedback foundintheskin.Anothertheorysuggeststhattheimproved ROMandpainareduetoanincreasedproprioseptivefeedback mechanismandmusclefacilitation.4,7,8,11
InthestudyThelenetal.,foundthatKTimproved pain-free shoulder range of motion but no effect on pain or function. They also observed KT and cervical spine trust manipulationreduceddisability.16Alotofpublishedclinical
trialshavesuggestedthat KT maybebeneficial intreating patellofemoralpain syndrome,shoulder impingement syn-drome,lowerextremityspasticityandposturalrehabilitation inParkinson’sDisease.6,7,17,18 Afewsystematicreviewshave
evaluated the effect of KT on musculoskeletal and differ-ent clinical conditions. These randomizedtrials compared KTversusshamtapingorotherinterventions.Theresultsof reviewssuggestedthatKT had no significantbenefitor its effectwas too small interms ofclinical practice.However thesetrialswerelow-moderatequality,smallsamplesizesand verysmallfollow-upperiods.4,7,8Themostimportant
differ-enceofourstudywastohavehighernumberpatientsand designed asa randomized double-blind placebo controlled study.
CervicalROMrestrictionmostlyoccursbecauseofmuscle spasminMPS.StudiesshowedimprovementinROMvalues afterKT.8,15Inourstudy,asignificantincreasewasobtained
in two weeks in cervical ROM in both groups. Although significantimprovementswereobservedoncervical flexion-extension,comparedtotheplacebogroup,buttherewasno changecervicalrotation,cervicallateralflexion.Theincrease in cervical ROM may be due to the reduction in patients’ cervicalmusclespasmsorexerciseprogramsappliedtothe patients.Inourstudy,homeexerciseprogramwasappliedto allpatientsandimprovementofcervicalROMwasobserved inbothgroups.Thelimitationofourstudywasnottohave an only exercise group which could be compared to KT and shamKT. Also, weinvestigatedthe short-term results ofKT.
Inconclusion,KTisanoninvasive,painlessmethodthat haslesssideeffects,iswelltoleratedandhasbeenusedin MPS.ThisstudyshowsthatKTleadstoimprovementsonpain, PPT,andROM,butnotindisabilityinshortperiod.Therefore, KTcanbeusedasanalternativetherapyinthetreatmentof
patientswithMPS.But,moreresearchisnecessaryforboth clinicalandlong-termeffectsoftheKinesioTapingtechnique.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GiamberardinoMA,AffaitatiG,FabrizioA,CostantiniR. Myofascialpainsyndromesandtheirevaluation.BestPract ResClinRheumatol.2011;25:185–98.
2.Radford-GraffSB.Myofascialpain:diagnosisand management.CurrPainHeadacheRep.2004;8:463–7. 3.ParreiraPCS,CostaLCM,TakahashiR,JuniorLCH,LuzJunior
MA,SilvaTM,etal.Kinesiotapingtogenerateskin convolutionsisnotbetterthanshamtapingforpeoplewith chronicnon-specificlowbackpain:arandomisedtrial.J Physiother.2014;60:90–6.
4.ParreiraPCS,CostaLCM,JuniorLCH,LopesAD,CostaLOP. Currentevidencedoesnotsupporttheuseofkinesiotaping inclinicalpractice:asystematicreview.JPhysiotherapy. 2014;60:31–9.
5.GüvenZ,C¸elikerR,AtalayA,Ba ˘gıs¸S,Aydo ˘gT,KorkmazN, etal.KinezyolojikBantlama ˙IleriKurs.Istanbul,Turkey: AcıbademÜniversitesi;2012.
6.SaygıEK,AydoseliKC,KablanN,Ofluo ˘gluD.Theroleof kinesiotapingcombinedwithbotulinumtoxintoreduce plantarflexorsspasticityafterstroke.TopStrokeRehabil. 2010;17:318–22.
7.KayaE,ZinnurogluM,TugcuI.Kinesiotapingcomparedto physicaltherapymodalitiesforthetreatmentofshoulder impingementsyndrome.ClinRheumatol.2011;30:201–7. 8.IglesiasJG,PenasCF,ClelandJ,HuıjbregtsP,VegaMRG.Short
termeffectsofcervicalKinesioTapingonpainandcervical rangeofmotioninpatientswithacutewhiplashinjury:a randomizedclinicaltrial.JOrthopSportsPhysTher. 2009;39:515–21.
9.SimonsDG.Muscularpainsyndrome.In:FrictionJR,Awad EA,editors.Advancesinpainresearchandtherapy.NewYork: RavenPres;1990.p.1–41.
10.BicerA,YaziciA,CamdevirenH,ErdoganC.Assessmentof painanddisabilityinpatientswithchronicneckpain: reliabilityandconstructvalidityoftheTurkishversionofthe neckpainanddisabilityscale.DisabilRehabil.2004;26: 959–62.
11.BassettKT,LingmanSA,EllisRF.Theuseandtreatment efficacyofkinaesthetictapingformusculoskeletalconditions: asystematicreview.NZJPhysiother.2010;38:56–62.
12.MorrisD,JonesD,RyanH,RyanCG.Theclinicaleffectsof KinesioTextaping:asystematicreview.PhysiotherTheory Pract.2013;29:259–70.
13.MuroFG,FernandezALR,LucasAH.Treatmentofmyofascial painintheshoulderwithkinesiotaping.Acasereport.Man Ther.2010;15:292–5.
14.WesthuizenVD,HendrikJ.Therelativeeffectivenessof Kinesiotapeversusdryneedlinginpatientswithmyofascial painsyndromeoftrapeziusmuscle,2012.
http://hdl.handle.net/10321/732.
15.HernandezMS,SanchezAMC,MoralesMA,ClelandJA, PalomoIL,PenasCF.Shorttermeffectsofkinesiotaping versuscervicalthrustmanipulationinpatientswith mechanicalneckpain:arandomizedclinicaltrial.JOrthop SportsPhysTher.2012;42:724–30.
16.ThelenMD,DauberJA,StonemanPD.Theclinicalefficacyof kinesiotapeforshoulderpain:arandomizeddoubleblinded, clinicaltrial.JOrthopSportsPhysTher.2008;38:
389–95.
17.FreedmanSR,BrodyLT,RosenthalM,WiseJC.Shortterm effectsofpatellarkinesiotapingonpainandhopfunctionin
patientswithpatellofemoralpainsyndrome.SportsHealth. 2014;6:294.
18.CapecciM,SerpicelliC,FiorentiniL,CensiG,FerrettiM,Orni C.Posturalrehabilitationandkinesiotapingforaxialpostural disordersinParkinson’sdisease.ArchPhysMedRehabil. 2014;95:1067–75.