ORIGINAL ARTICLE
Comparison of three different approaches in the treatment
of chronic low back pain
Şebnem Koldaş Doğan&Birkan Sonel Tur& Yeşim Kurtaiş&Mesut Birol Atay
Received: 2 September 2007 / Revised: 15 November 2007 / Accepted: 1 December 2007 / Published online: 11 January 2008
# Clinical Rheumatology 2007
Abstract Our aim is to investigate the effects of three therapeutic approaches in the chronic low back pain on pain, spinal mobility, disability, psychological state, and aerobic capacity. Sixty patients with chronic low back pain were randomized to three groups: group 1, aerobic exercise + home exercise; group 2, physical therapy (hot pack, ultrasound, TENS) + home exercise; group 3, home exercise only. Spinal mobility, pain severity, disability, and psychological disturbance of the patients were assessed before and after the treatment and at 1-month follow-up. Aerobic capacities of the patients were measured before and after treatment. All of the groups showed similar decrease in pain after the treatment and at 1-month follow-up, and there was no significant difference between the groups. In group 2, a significant decrease in Beck Depression Inventory scores was observed with treatment. At 1-month follow-up, group 1 and 2 showed significant decreases in General Health Assessment Questionnaire scores. In group 2, there was also a significant improvement in Roland
Morris Disability scores. There were similar improvements in exercise test duration and the MET levels in all the three groups. All of the three therapeutic approaches were found to be effective in diminishing pain and thus increasing aerobic capacity in patients with chronic low back pain. On the other hand, physical therapy + home exercise was found to be more effective regarding disability and psychological disturbance.
Keywords Aerobic exercise . Chronic low back pain . Disability . Home exercise and physiotherapy treatment
Introduction
Low back pain affects 50 to 80% of adults at some time during their lives [1–8], and it appears to be an important medical condition with its consequences. The low back pain lasting more than 3 months is referred to as chronic low back pain [4,9–15]. The chronic low back pain gives rise to physical and psychological problems, disability, and deterioration in the quality of life [1, 6, 8, 11, 16]. The chronic low back pain is also an important health problem from an economic point of view as regards to the decrease in the manpower of the individual, diagnostic interventions, repetitive treatments and the related treatment costs.
There are various approaches involved in the treatment of the chronic low back pain. The active treatment methods, which encourage individuals to participate in the treatment process, are increasingly advocated. It is recently claimed that these treatment approaches are effective in alleviating the pain and disability as well as increasing spinal mobility and endurance [9, 15–19]. However, physical therapy modalities, as conventional treatment methods, still main-tain their role in the treatment of patients with chronic low
DOI 10.1007/s10067-007-0815-7
Presented at the 5th Mediterranean Congress of Physical Medicine and Rehabilitation, Antalya, Turkey 30 September–4 October 2004. Ş. Koldaş Doğan (*)
Department of Physical Medicine and Rehabilitation, Ufuk University School of Medicine,
Ankara, Turkey
e-mail: [email protected] B. Sonel Tur
:
Y. Kurtaiş:
M. B. AtayDepartment of Physical Medicine and Rehabilitation, Ankara University School of Medicine,
Ankara, Turkey Present address: Ş. Koldaş Doğan
100.yıl mah. 399.sok. Ozpetek sitesi. 33/43, Ankara, Turkey
back pain. Diversity and cost of treatments, and the lack of sufficient randomized and controlled studies on the effec-tiveness of these treatment methods are the most important reasons leading to the confusion in choosing the appropriate treatment approaches, hence, the growth of interest in this field [11, 20–22]. As indicators of the effectiveness of treatment, the changes in the cardiopulmonary fitness level has recently gained importance, in addition to such determinants as pain severity, spinal mobility, disability and psychological status, etc [17,18,23,24].
The aim of this study is to investigate and compare the effects of three different treatment approaches (namely aerobic exercise + home exercise, physical therapy + home exercise and home exercise only) on pain, spinal mobility, disability, psychological status, and aerobic capacity to develop a better approach for these patients.
Materials and methods Subjects
Sixty patients who were admitted to the out-patient clinic of Physical Medicine and Rehabilitation Department with chronic low back pain were included in the study. The sociodemographical characteristics (age, gender, occupa-tion, marital status, disease duraoccupa-tion, previous treatments) of the patients as well as the severity of their pain were recorded.
The inclusion criteria were (a) a history of low back pain exceeding 3 months, (b) being above the age of 25 years old, (c) the willingness to comply with any one of the randomly chosen treatment programs, and (d) the written informed consent of the patient.
The exclusion criteria were (a) the presence of the herniated lumbar disk, (b) the acute phase of the lumbar disk protrusion, (c) the presence of the vertebral fracture(s), (d) cardiovascular or systemic diseases or any condition which contraindicated or made the exercise training impossible, (e) the neurological deficit, (f) the presence of the psychiatric disorder which might affect the compliance and the assessment of symptoms, (g) the history of the spinal surgery, (h) the pregnancy, (i) inflammatory, infec-tious or malignant diseases of the vertebra, (j) the presence of severe structural deformity.
Treatment groups
The patients were randomly assigned to one of the three groups using a sequence of random numbers before baseline assessments were performed. All three groups were requested to do home exercises: (1) basic flexion (sitting-up straight and with rotation to right and left), (2)
extension (prone trunk extension), (3) mobilization and (4) stretching (raising the legs, double-knee-to-chest in back lying position and lifting the right arm/left leg and left arm/ right leg alternately in all-four positions) for 6 weeks, performing each exercise once a day with 15–20 repetitions.
Group 1 The patients in this group were assigned aerobic exercise to be performed on the treadmill. The aerobic exercise has been performed three times a week for 6 weeks. Each exercise session was planned to last 40–50 min including 5 min of warm-up and cool-down periods. Being the lowest range recommended for aerobic exercise, the target heart rate was based on 65–70% of the maximum heart rate of each individual during the stress testing. Low intensity was preferred, since patients have pain, the aerobic exercise program was held under the supervision of a physical therapist and was controlled by the authors. Group 2 The patients in this group were assigned physical therapy. The superficial heating with hot packs was applied to the low back region for 15 min. The patients also received continuous ultrasound (US) using a 2776 Intellect Mobile Ultrasound device (Chattanooga, Tennessee, USA) that operated at 1 MHz frequency and 1.5 W/cm intensity and a transducer head with an area of 5 cm, an ERA of 4 cm and a BNR of 1:5. Slow circular movements were applied by the transducer head over the paravertebral low back region. The treatment duration was 10 min.“Aquasonic®” transmission-gel (Aquasonic, Ankara, Turkey) was used, which is known to be inert and has good acoustic conductive properties for ultrasound. Finally, transcutaneous electrical nerve stimula-tion (TENS; 30–40 Hz by means of convenstimula-tional method) was applied for 15 min. The physical therapy sessions have been practiced three times a week for 6 weeks.
Group 3 The patients in this group have performed only home exercises for 6 weeks. The patients’ compliance of home exercises was controlled by two ways: having an exercise diary and checking by phone calls. All patients were informed about the ways of the correct use and the strengthening of the low back, the benefits of strengthening and the gaining flexibility, the proper performance of repetitive movements during lying in the bed, standing, sitting, bending, lifting weights etc. in their daily life. Assessment methods
The patients were assessed for spinal mobility, pain, aerobic fitness, global status, disability, and psychological status both before and after the treatment as well as at a follow-up after 1 month. The spinal mobility was assessed by modified Schober test [25], finger tip to floor distance and lateral bending. The low back pain severity was assessed by
visual analogue scale (VAS, 0 mm: no pain, 100 mm: severe pain) [26]. For disability assessment, Roland Morris Disability Questionnaire (RMDQ) was used [27,28]. The General Health Questionnaire (GHQ) [29, 30] and Beck Depression Inventory (BDI) [31,32] were used for general and psychological state of the patients.
For the assessment of the aerobic fitness level, all the patients were given an ergospirometric exercise test (Bruce protocol) to volitional exhaustion on the treadmill both in the beginning and the end of the treatment period (6 weeks after). The patients were informed about the test and it was ensured that the individuals had not eaten anything at least 2 h before the test. To rule out any respiratory problems, which may adversely affect the exercise, the dynamic respiratory function tests were carried out. 12-Lead elec-trocardiography (Marquette Case I; Marquette, Milwaukee, WI), blood pressure, and breath-by-breath analysis of respiratory gases (Vmax29, Sensormedics, Yorba Linda, CA) were recorded during the exercise test. Each subject’s peak oxygen consumption was determined from the VO2-time plots (ml/kg/min). The exercise test duration and the MET levels were also recorded.
Statistical evaluation
Data were analyzed using SPSS-9.0 statistical package. The sociodemographical characteristics of the groups were eval-uated by Chi-square test. The effectiveness of the treatments in the groups before the treatment, after the treatment and at 1 month follow-up was compared by means of the multiple comparison tests using the Friedman bi-directional variance analysis [33]. In case of statistically significant differences, comparison pairs were analyzed by means of the Wilcoxon test. The level of the significance was accepted as p<0.05 for all tests, but since there were three groups, the p significance value was calculated to be 0.017 for the comparisons. The matched samples of the pre-treatment and the post-treatment aerobic capacity measurements were compared by the Wilcoxon test. The differences between the groups for the assessed parameters were analyzed by means of the Kruskal Wallis variance analysis [34].
Results
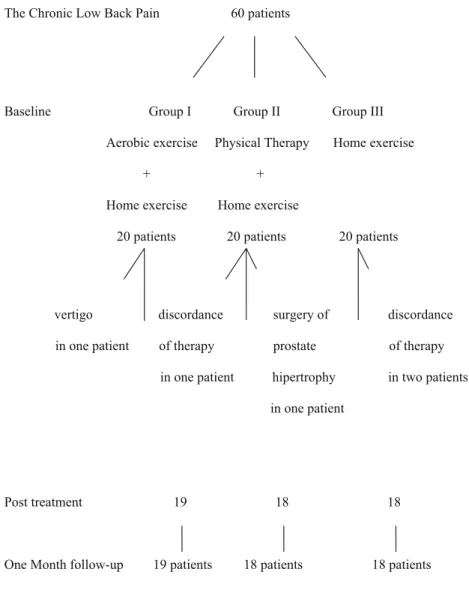
There were 60 patients, 45 female and 15 male with a mean age of 40.2±8.4 years (min, 25; max, 59), with chronic low back pain included in the study. The average duration of the symptoms was 53.6±66.4 months (min, 3; max, 240). One patient from group 2, and two patients from group 3 were dropped out because of the poor compliance to the treatment. One patient from group 1 could not complete the treatment program due to vertigo and one patient from
group 2 was dropped out because of the surgery performed with the diagnosis of benign prostate hyperthropy. A total of 55 patients (43 female and 12 male) have completed the treatment (Figure 1). The sociodemographic characteristics of the patients are shown in Table 1. No significant differences were observed between the groups regarding age, gender, occupation, education, and disease duration.
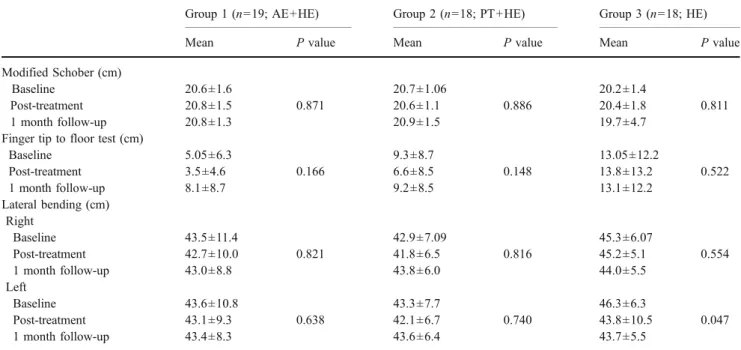
No statistically significant difference was found within and between groups regarding the spinal mobility over time (Table 2).
In group 1 (aerobic exercise + home exercise), there was a statistically significant improvement in the pain severity and GHQ scores at 1-month follow-up when compared to the pre-treatment levels ( p=0.002, p=0.053, respectively; Table 3). The statistically significant improvement was observed in the fitness level, which was assessed by means of the exercise test duration and MET levels ( p=0.000, p=0.000, respec-tively). There was an increase in the VO2peak, which did not reach to the level of the statistical significance ( p=0.087).
In group 2 (physical therapy + home exercise), a statistically significant improvement was observed in the patient’s pain severity and BDI scores, and a statistically significant increase was observed in the fitness level, as compared to the baseline, when assessed by the exercise test duration and the MET levels at post-treatment evalu-ation. At 1 month follow-up, the pain severity, and the scores of GHQ and RMDQ decreased significantly when compared to the baseline ( p=0.001, p=0.010 and p=0.010, respectively; Tables3 and4).
In group 3 (home exercise only), there was a significant improvement in the pain severity ( p=0.006), and a sig-nificant increase in the fitness level, which was assessed by means of the exercise test duration and MET levels ( p= 0.001 and p=0.001), but not a statistically significant increase in the VO2peak at post-treatment evaluation. At 1-month follow-up, a significant improvement was ob-served in the pain severity ( p=0.001; Tables3 and4).
There were no significant differences between three groups in the pain severity, disability, and psychologic status before and after the treatment, and at 1-month follow-up. Post-treatment benefits were still observed 1 month after the treatment.
Discussion
Chronic low back pain is a serious health problem in Turkey just as it is in the other countries. While low back pain persisting more than 3 months was accepted as chronic low back pain [4, 9–13] previously, this period has been reduced to as low as 6 weeks currently [21, 35]. Chronic low back pain leads significant loss of physical and psychosocial functions of the individuals. This condition,
which generally occurs when the individual is supposed to be most productive, causes loss of labor force and gives rise to the economic losses. The diagnostic methods used and the multiple treatments administered greatly contribute to the economic losses also.
The goal of the treatment in the chronic low back pain is to alleviate the pain, to enhance mobility, to prevent both the physical and the mental disability, and to improve the life quality and the physical functions. To attain these goals, various treatment programs are suggested. Medical treat-ment, physical therapy, massage, manipulation and traction, and therapeutical exercises are the frequently administered therapies. The physical therapy modalities are generally used in combinations together with the exercises. The effects of the physical therapy modalities on the chronic low back pain have been demonstrated with uncontrolled studies [11]. There are few randomized controlled studies investigating the effect of these modalities and there is no consensus on which treatment methods are more effective [11,20–22].
Table 1 The sociodemographical characteristics of the patients Group 1 (n=19) (AE1+HE2) Group 2 (n=18) (PT3+HE) Group 3 (n=18) (HE) P value Age (year) 37.1±6.5 41.5±8.3 42.1±9.5 0.13 Sex Female (n, %) 15 (78.9) 14 (77.8) 14 (77.8) 0.9 Male (n, %) 4 (21.1) 4 (22.2) 4 (22.2) Disease duration (month) 38.8±56.7 62.6±81.0 59.4±61.5 0.5 Work status Hard (%) 2 (10.5) 6 (33.3) 3 (16.7) Moderate (%) 8 (42.1) 8 (44.4) 4 (22.2) 0.11 Low (%) 9 (47.4) 4 (22.2) 11 (61.1)
Values given are mean (standard deviation). Groups were evaluated by Chi-Squared test and the level of significance was accepted as p<0,05. AE, aerobic exercise; HE, home exercise; PT, physical therapy
The Chronic Low Back Pain 60 patients
Baseline Group I Group II Group III Aerobic exercise Physical Therapy Home exercise
+ + Home exercise Home exercise
20 patients 20 patients 20 patients
vertigo discordance surgery of discordance in one patient of therapy prostate of therapy
in one patient hipertrophy in two patients in one patient
Post treatment 19 18 18
One Month follow-up 19 patients 18 patients 18 patients
Fig. 1 The flow chart of the study sample
In this study, the effects of three different treatment approaches consisting of aerobic exercise, physical therapy and home exercise on the spinal mobility, pain, disability, psychological status, and aerobic capacity were investigated in the patients with chronic low back pain. While in some studies [17] the efficacy of the treatment was demonstrated in comparison with the placebo group, in this study, there
was no placebo group because it was considered to be unethical to use a placebo group in such design.
In the patients with the low back pain, limitation and tension occur in soft tissues and joints. In some studies, it was demonstrated that the exercising improved spinal mobility in chronic low back pain [11, 12, 36, 37]. In a study by Mannion et al., the efficacy of three different
Table 3 The spinal mobility measurements of the patients
Group 1 (n=19; AE+HE) Group 2 (n=18; PT+HE) Group 3 (n=18; HE) Mean P value Mean P value Mean P value VAS (mm) Baseline 57,05±24,5 0.002 61,2±20,5 0.0001 56,0±19,9 0.001 Post-treatment 34,9±30,8 38,9±23,4 40,0±21,8 1 month follow-up 34,1±27,6 28,8±28,1 33,6±24,3 RMDQ (0-24) Baseline 11,9±5,4 0.083 11,9±5,9 0.011 13,6±7,4 0.81 Post-treatment 8,9±6,8 8,9±6,0 13,6±6,6 1 month follow-up 9,2±7,3 8,3±5,8 13,3±7,3 GHQ (0-36) Baseline 15,1±6,8 0.027 14,3±5,9 0.01 12,8±7,5 0.65 Post-treatment 11,6±7,3 9,7±4,8 11,5±7,5 1 month follow-up 11,7±8,1 8,8±6,06 12,2±6,6 BDI (0-63) Baseline 14,1±9,2 0.179 12,2±8,7 0.044 12,8±9,2 0.743 Post-treatment 14,2±10,5 8,6±7,01 13,3±9,8 1 month follow-up 12,7±9,8 8,5±7,6 12,5±8,06
Values given are mean (standard deviation). Friedman bi-directional variance analysis was used and the level of significance was accepted as p<0,05. AE, aerobic exercise; HE, home exercise; PT, physical therapy; VAS, visual analog scale; RMDQ, Roland-Morris disability questionnaire; GHQ, general health questionnaire; BDI, Beck depression inventory.
Table 2 The spinal mobility measurements of the patients
Group 1 (n=19; AE+HE) Group 2 (n=18; PT+HE) Group 3 (n=18; HE) Mean P value Mean P value Mean P value Modified Schober (cm)
Baseline 20.6±1.6 20.7±1.06 20.2±1.4
Post-treatment 20.8±1.5 0.871 20.6±1.1 0.886 20.4±1.8 0.811 1 month follow-up 20.8±1.3 20.9±1.5 19.7±4.7
Finger tip to floor test (cm)
Baseline 5.05±6.3 9.3±8.7 13.05±12.2 Post-treatment 3.5±4.6 0.166 6.6±8.5 0.148 13.8±13.2 0.522 1 month follow-up 8.1±8.7 9.2±8.5 13.1±12.2 Lateral bending (cm) Right Baseline 43.5±11.4 42.9±7.09 45.3±6.07 Post-treatment 42.7±10.0 0.821 41.8±6.5 0.816 45.2±5.1 0.554 1 month follow-up 43.0±8.8 43.8±6.0 44.0±5.5 Left Baseline 43.6±10.8 43.3±7.7 46.3±6.3 Post-treatment 43.1±9.3 0.638 42.1±6.7 0.740 43.8±10.5 0.047 1 month follow-up 43.4±8.3 43.6±6.4 43.7±5.5
treatment methods, that is, the physical treatment, the strengthening body muscles, and exercises performed using conditioning tools to strengthen body muscles and aerobic exercises were compared. The evaluation carried out after 6 months showed that the groups doing the aerobic exercises or the strengthening exercises exhibited more improvement than the physical therapy group [11]. In our study, no change occurred in the spinal mobility in comparison with the baseline in any of the treatment groups.
In the individuals with the chronic low back complaint, the muscular strength decreases and the muscle group of body extensors are more influenced than the flexor group [10,16,24,38]. In a study, the authors showed an increase in the muscle strength after an exercise program of 15 days [10]. The similar results were also reported after the exercise and the active rehabilitation programs [17,38]. Patients with low back pain limit their physical activities with the fear of worsening their pain, and restrictions in daily activities lead to disability. The therapeutic exercises suggested for the low back pain are also effective in both diminishing the pain severity and the disability [11,12,17,18].
In our study, while significant decrease in the pain severity was observed in all groups, the decreased disability was detected only in the group 2. This result can be attributed to the stronger faith of the Turkish population in the effectiveness of physical therapy. In their study on the effect of trust in treatment to low back pain and disability in patients with low back pain, Goldstein et al. have reported that trust in treatment is higher when physical treatment is included in medical treatment and that there is a significant decrease in pain and disability in this patient group [39]. Another study showed the efficacy of the physical therapy in diminishing the level of disability although the physical therapy modalities were not standardized [21]. Additional-ly, differing attitude of groups against disability can be their habituation of the patients to the disabling effects of pain.
Kankaanpa et al. compared two treatment programs, the active rehabilitation program consisting of exercises in-cluding stretching, relaxation, muscle strengthening and coordination, and a placebo treatment consisting of only massage and superficial heat application on 59 patients with chronic low back pain. A significant decrease in the pain and the disability was observed in the treatment group in the third month, where there was no change in the placebo group and the difference became more significant in the follow-ups carried out at sixth month and first year [17]. In our study, although home exercise program is similar to that of Kankaanpa et al.’s, the only change observed was in the pain severity, not in disability. The difference in the findings of two studies may be because of the fact that the exercise program was not supervised.
Bensten et al. compared the efficacy of two exercise treatments in their randomized research. The first group was given a program consisting of strengthening exercises of the low back and the back muscles administered in a fitness centre and home exercises of flexion and extension for 3 months. The second group was given a program consisting of only home exercises. At the end of the treatment, both groups displayed a significant decrease in the disability. At the end of the first year, the first group demonstrated a better improvement and at 3 years follow-up, no significant difference could be determined between the groups. However, the compliance rate was lower in the home exercise group. It was concluded that the effect of the treatment depended on the motivation and the compliance of the patient rather than the intensity of the exercises [20]. Hartigan et al. questioned the exercise compliance of the patients with the chronic low back pain at the third month following an intensive rehabilitation program. In this process, significant decreases in the severity of pain and disability levels were found; the decrease was maintained at the 12th month also [36]. In our study, although the pain
Table 4 The aerobic capacity of the patients before and after the treatment
Group 1 (n=19; AE+HE) Group 2 (n=18; PT+HE) Group 3 (n=18)
Mean P value Mean P value Mean P value Test duration (min)
Baseline 9,7±2,5 0.0001 8,3±2,9 0.0001 9,3±2,8 0.0001 Post-treatment 12,1±2,2 9,8±2,5 9,9±2,9 MET level Baseline 11,3±2,7 0.0001 9,7±2,9 0.0001 10,8±2,9 0.0001 Post-treatment 14,2±2,6 11,3±3,08 11,6±3,09 VO2peak (ml/kg/min) Baseline 2,3±0,6 0.087 2,2±0,5 0.586 2,1±0,6 0. 868 Post treatment 2,5±0,8 2,1±0,6 2,0±0,5
Values given are mean (standard deviation). Measurements were compared by using Wilcoxon test. AE, aerobic exercise; HE, home exercise; PT, physical therapy
severity has decreased in all three groups, which can be taken as an indicator that the patients’ compliance to the treatment was good, a decrease in disability was demon-strated only in group 2 (physical therapy + home exercise). In a study comparing two different home exercise programs, one group was administered a customized exercise program based on the initial evaluation findings. The other group was suggested flexion, extension, mobilization and stretching exercises. While both groups exhibited an im-provement in the extensor muscle power, a significant improvement was determined only in the groups that customized exercises were suggested. It was concluded that the short and individualized exercises are more effective in decreasing the pain and the disability than the standard exercises [3]. In our study also, the suggested home program consists of flexion, extension, mobilization and stretching exercises. Lack of programming the exercises in an individual fashion explains the lack of improvement in group that home program was suggested.
The decreased physical activity due to the prolonged persistent pain leads to anxiety, and depression. Such psychological changes and pain contribute to disability, which in return give rise to constraints imposed on the social activities of the individual. In a study performed on 221 patients with the low back pain, it was demonstrated that 71 patients had depression and somatic disorders (33%) and disability rates were found to be higher in this group [6].
Several studies discussed the effect of exercise on the psychosocial changes in the patients with the chronic low back pain and observed improvements in the depression scores following the exercise treatment [11,12,16]. In our study, a significant decrease was observed in the BDI scores in group 2 (physical therapy + home exercise) when compared to the baseline. One month after the treatment, there was a statistically significant decrease in the GHQ scores in group 1 (aerobic exercise + home exercise) and group 2 (physical therapy + home exercise). Although the baseline pain severity was not very high in our study, significant decreases both in pain severity and psychologi-cal parameters were found in these groups. Therefore, both treatment modalities are effective in providing improve-ment in psychological status.
In a study where a 12-week active exercise program was administered for the chronic low back pain, a decrease in pain severity, disability, and depression was attained. At 14-month follow-up following rehabilitation, it was deter-mined that there was less severe pain and less drug use in the group, which continued exercises after the end of the treatment. It was concluded that the continuing exercises after active rehabilitation made great contributions to maintain the gains obtained by the active rehabilitation [12].
The patients with the chronic low back pain avoid much physical activity with the fear of pain. The vicious circle of
decreased muscle power and the cardiac capacity due to the low activity level, decreased the metabolic activity and the fatigue as well as the tendency to the muscle spasms, leads to the deconditioning syndrome. It is believed that the pain leads to deconditioning and contributes to the development of chronic pain [24, 40–42]. The relationship between the increase in aerobic capacity and the improvement of pain and disability has been reported in some studies [18,24,43].
Van der Velde administered a 6-week active rehabilita-tion program consisting of aerobic exercise, strengthening exercises for lower and upper extremity muscles and stretching exercises to the patients with the chronic low back pain, and compared the pain severity, the disability and the aerobic capacity with those of the control group. Aerobic capacities of the patients were found to be low before the treatment. Significant improvement was ob-served in aerobic capacity with decreased pain and disability after the treatment. They concluded that the improvement in the aerobic capacity is clinically and statistically correlated to the decrease in the pain and the disability [18]. In our study, regarding the parameters of the aerobic capacity, significant increases in the exercise test duration and the MET levels in all three groups and not significant increase in the V02peak in group 1 was observed with the treatment.
In the study of Sculco et al., aerobic exercise was administered as the sole treatment and its effects on pain, depression, and anxiety were investigated. However, the aerobic capacity measurements of the patient and the control groups were not taken into consideration [44].
Oldervoll divided the hospital employees with the prolonged low back pain into the groups of endurance exercises, muscle strengthening exercises, and a control group to compare pain severity and aerobic capacity before and after the treatment. Similar to our study, decreased pain was observed in all of the groups. However, the aerobic capacity increased only in the endurance exercises group, it did not change in the muscle strengthening exercise group, and decreased in the control group [23]. This study, suggesting that increase in aerobic capacity is not required for a decrease in the intensity of pain, which is also similar to our findings since the VO2peak did not increase in all of the groups.
Low number of patients included is a limitation of this study which should be an argue that decreased the effect of statistical analysis.
In conclusion, three different treatment approaches are found to be effective in decreasing the pain in patients with the chronic low back pain. This study showed that the patients should absolutely be recommended home exercise programs, which is the lowest cost alternative. However, the home exercise program alone did not have any effect on the disability and the psychological state, whereas physical
therapy plus home exercise program provides improvement in disability and psychological condition. There is a cor-relation between the increased fitness level and the decreased pain or vice versa.
References
1. Sinaki M, Mokri B (2000) Low back pain and disorders of the lumbar spine. In: Braddom RL (ed) Physical Medicine and Rehabilitation. WB Saunders Comp, Philadelphia, pp 853–893 2. Weinstein SM, Herring SA (1993) Rehabilitation of the patient
with low back pain. In: Delisa JA, Gans BM (eds) Rehabilitation Medicine Principles and Practice. J.B. Lippincott Company, Philadelphia, pp 996–1017.
3. Descarreaux M, Normand MC, Laurencelle L et al (2002) Evaluation of a specific home exercise program for low back pain. J Manipulative Physiol Ther 25:497–503
4. Wheeler AH (1995) Diagnosis and management of low back pain and sciatica. Am. fam. phys 52(5):1333–1341
5. Phillips K, Ch’ien APY, Norwood BR et al (2003) Chronic low back pain management in primary care. The Nurse Practitioner 28 (8):26–31
6. Lahad A, Malter AD, Berg AO et al (1994) The effectiveness of four interventions for the prevention of low back pain. JAMA 272 (16):1286–1291
7. Helewa A, Goldsmith CH, Lee P et al (1999) Does strengthening the abdominal muscles prevent low back pain – a randomized controlled trial. J Rheumatol 26:1808–1815
8. Frank AO, Souza LD (2001) Conservative management of low back pain. Int J Clin Pract 55(1):21–31
9. Liddle SD, Baxter GD, Gracey JH (2004) Exercise and chronic low back pain: what works? Pain 107:176–190
10. Bayramoğlu M, Akman MN, Kılınç Ş et al (2001) Isokinetic measurement of trunk muscle strength in women with chronic low back pain. Am J Phys Med Rehabil 80:650–655
11. Mannion AF, Müntener M, Taimela S et al (2001) Comparison of three active therapies for chronic low back pain: results of a randomized clinical trial with one-year follow-up. Rheumatol 40: 772–778
12. Taimela S, Diederich C, Hubsch M (2000) The role of physical exercise and inactivity in pain recurrence and absenteeism from work after active outpatient rehabilitation for recurrent or chronic low back pain. Spine 25:1809–1816
13. Tulder MV, Malmivaara A, Esmail R et al (2000) Exercise therapy for low back pain. Spine 25:2784–2796
14. Saridoğan ME (2000) Bel ağrısı nedenleri ve epidemiyolojisi. In: Kutsal YG (ed) Modern Tıp Seminerleri. Ankara pp 19–29 15. Özcan E (2002) Bel ağrılı hastaların konservatif tedavisi. In:
Özcan E, Ketenci A (eds) Bel Ağrısı Tanı ve Tedavi. Nobel Kitabevi,İstanbul, pp 187–219
16. Rainville J, Hartigan C, Martinez E et al (2004) Exercise as a treatment for chronic low back pain. Spine J 4:106–115 17. Kankaanpaa M, Taimela S, Airaksinen O et al (1999) The efficacy
of active rehabilitation in chronic low back pain. Spine 24:1034– 1042
18. Van der Velde G, Mierau D (2000) The effect of exercise on percentile rank aerobic capacity, pain, and self-rated disability in patients with chronic low-back pain: a retrospective chart review. Arch Phys Med Rehabil 81:1457–1463
19. Chatzitheodorou D, Kabitsis C, Malliou P et al (2007) A pilot study of the effects of high-intensity aerobic exercise versus passive interventions on pain, disability, psycgological strain, and serum cortisol concentrations in people with chronic low back pain. Phys Ther 87(3):304–312
20. Bensten H, Lindgarde F, Manthorpe R (1997) The effect of dynamic strength back exercise and/or a home training program in 57 year old women with chronic low back pain. Spine 22:1494–1500
21. Ross MD (2002) Physical therapy and changes in disability for patients with low back pain. Military Medicine 167:662–665 22. Brosseau L, Milne S, Robinson V et al (2002) Efficacy of the
transcutaneous electrical nerve stimulation for the treatment of chronic low back pain. Spine 27:596–603
23. Oldervoll LM, Ro M, Zwart JA (2001) Comparison of two physical exercise programs for the early intervention of pain in the neck, shoulders and lower back in female hospital staff. J Rehabil Med 33:156–161
24. Carpenter DM, Nelson BW (1999) Low back strengthening for the prevention and treatment of low back pain. Medicine and science in sports and exercise 31(1):18–24
25. Macrael IF, Wright V (1969) Measurement of back movement. Ann Rheum Dis 28:584
26. Gatchel RJ, Mayer TG, Capra P et al (1986) Quantification of lumbar function. Part 6: the use of psychological measures in guiding physical functional restoration. Spine 11:36–42 27. Roland M, Morris R (1983) A study of the natural history of back
pain. Spine 8:141
28. Kucukdeveci AA, Tennant A, Elhan AH et al (2001) Validation of the Turkish version of the Roland Morris Disability Questionnaire for use in low back pain. Spine 26(24):2738–2743
29. Goldberg DP, Williams P (1988) A user’s guide to the General Health Questionnaire. NFER/Nelson, Windsor, CA
30. Kılıc C (1996) Genel Sağlık Anketi; güvenirlik ve geçerlik çalışması. Türk Psikiyatri Dergisi 7:3–9
31. Beck AT (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571
32. Hisli N (1989) Beck Depresyon Envanterinin üniversite öğrencileri içi geçerliği, güvenirliği. Psikoloji Dergisi 7:3–13
33. Siegel S, Castellan NJ (1988) The case of k related samples, section 7,2: The Friedman two-way analysis of variance by Ranks. In: Siegel S, Castellan NJ (eds) Nonparametric Statistics for the Behavioral Sciences. Mc Graw Hill Inc, New York, pp 174–183 34. Conover WJ (1980) Some methods based on Ranks, section 5,2
several independent samples. In: Conover WJ (ed) Practical Non-parametricİstatistics. John Wiley and sons, pp 229–239 35. Jacobsson L, Lindgarde F, Monthorpe R (1989) The commonest
rheumatic complaints of over six weeks’ duration in a twelve month period in a defined Swedish population: prevalences and relationships. Scand J Rheumatol 18:353–360
36. Hartigan C, Rainville J, Sobel JB et al (2000) Long term exercise adherence after intensive rehabilitation for chronic low back pain. Medicine and science in sports and exercise 32(3):551–557 37. Rainville J, Jouve CA, Hartigan C et al (2002) Comparison of
short and long term outcomes for aggressive spine rehabilitation delivered two versus three times per week. The Spine Journal 2:402–407
38. Handa N, Yamamoto H, Tani T et al (2000) The effect of trunk muscle exercises in patients over 40 years of age with chronic low back pain. J Orthop Sci 5:210–216
39. Goldstein MS, Morgenstern H, Hurwitz EL et al (2002) The impact of treatment confidence on pain and related disability among patients with low back pain: results from the University of
California, Los Angeles, low back pain study. The Spine Journal 2:391–401
40. Wittink H, Michel TH, Wagner A et al (2000) Deconditioning in patients with chronic low back pain. Spine 25:2221–2228 41. Hoch AZ, Young J, Press J (2006) Aerobic fitness in women with
chronic discogenic nonradicular low back pain. Am J Phys Med Rehabil 85(7):607–613
42. Smeets RJ, Wittink H, Hidding A et al (2006) Do patients with chronic low back pain have a lower level of aerobic fitness than
healthy controls?: are pain, disability, fear of injury, working status, or level of leisure time activity associated with the difference in aerobic fitness level. Spine 31(1):90–97
43. Cunha IT, Simmonds MJ, Protas EJ et al (2002) Back pain, physical function and estimates of aerobic capacity. Am J Phys Med Rehabil 81:913–920
44. Sculco AD, Paup DC, Fernhall B et al (2001) Effects of aerobic exercise on low back pain patients in treatment. The Spine Journal 1:95–101