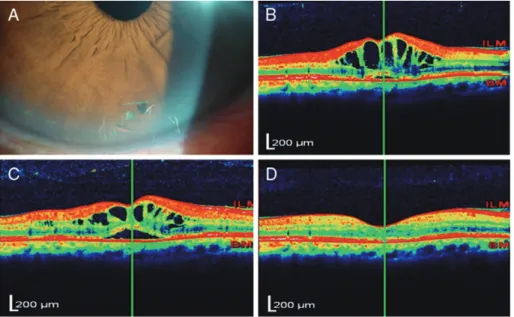
Refractory cystoid macular oedema due to intraocular lens haptic perforating the iris
Tam metin
Şekil
Benzer Belgeler
Çalışmamızın verilerine göre kronik sisplatin uygulaması (10 mg/kg/hafta, 5 hafta bo- yunca) sıçanların plazma ACTH ve CORT seviyelerinde kontrol grubuna kıyasla herhangi
Wayne Booth’un ironiyle ilgili daha önce yazılmış olan The Concept of Irony (Kierkegaard), The Com- pass of Irony (D.C. Muecke), The Word ‘Irony’ and Its Contexts: 1500-1755
Introduction: To evaluate the visual and refractive outcomes after implantation of a monofocal aspheric yellow chromophore intraocular lens (Eyecryl Plus ASHFY600, Biotech
This is a case report of a 29-year-old pregnant woman with bilateral serous macular detachment following cesarean section due to severe preeclampsia.. The patient applied with
Spectral domain optical coherence tomography: retinal folds affecting the neural retina in particular, without involvement of the RPE-choroid band and macular cystoid lesions
Materials and Methods: This retrospective study included 19 vitrectomized eyes and 11 non-vitrectomized eyes that underwent dislocated IOL extraction and secondary anterior
Conclusion: In eyes with DME, CMD can be defined as the largest cyst within 1000 μm of the foveal center having a horizontal diameter of ≥450 μm and vertical diameter ≥300
This study was designed to evaluate the postoperative outcomes, such as visual acuity improvement, refractive changes, myopic shift, complications, and additional surgical
