Başlık: The Role of FDG PET/CT in a Patient with Larynx Cancer Who Developed Necrotizing Fasciitis Secondary to Tracheostomy Which is a Rare ComplicationYazar(lar):BAYAR, Ebru; BURAL, GoncaCilt: 70 Sayı: 1 Sayfa: 067-070 DOI: 10.1501/Tipfak_0000000966 Yay
Tam metin
Şekil
Benzer Belgeler
In conclusion, although the definitive diagnosis of lung cancer is established by histopathological analysis, positron emission tomography/computed
Operasyon bulgularına ve patolojik incelemeye bağlı olarak tedavisi appendektomiden sağ hemikolektomiye kadar uzanır.Bu yazıda; karın ağrısı ile tarafımıza başvuran,
As being a functional imaging technique PET is a very sensitive and whole body imaging technique when compared to anatomical imaging modalities like CT, MRI, and
Sarcoid-Like Reaction Mimicking Nodal Spread of Lung Cancer in a Silica-Exposed Patient on Positron Emission Tomography/Computed Tomography: A Case Report | Şen et al.. 15
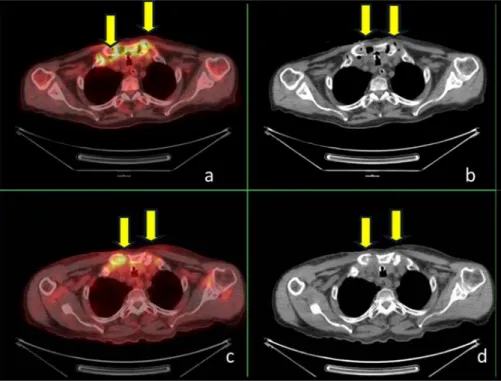
Axial slices of computed tomography (CT) (A), F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT fusion (B) and F-18 FDG PET (C) images of a 64-year-old
The results of the present study (97.93%) corroborates with these three studies in terms of vocabulary coverage, and it means that the model predicting the equation
Araştırmamızda bebeklerin gestasyon yaşlarına ve doğum kilolarına göre ebeveynlerin YYBÜ Anne Baba Stres Ölçeğinden aldıkları puan ortalamaları arasında
Our results reveal that plasma-cleaned titanium surfaces provide a clean and reproducible starting condition for further plasma treatments to form well-controlled surface
