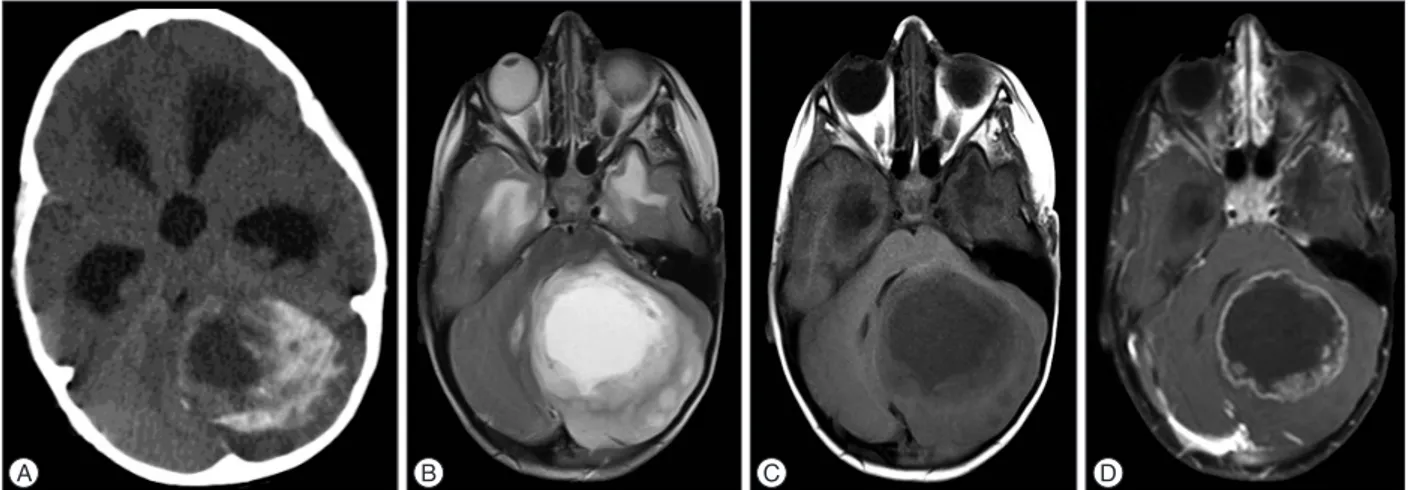
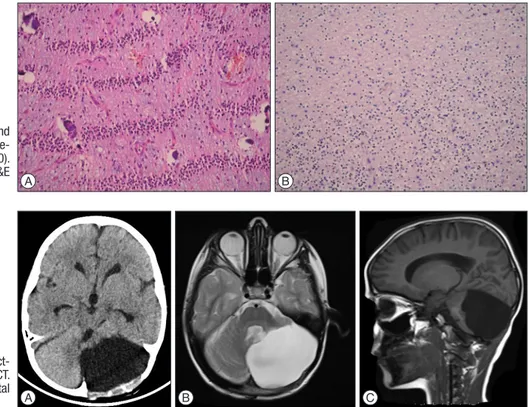
Massive Calcified Cerebellar Pilocytic Astrocytoma with Rapid Recurrence : A Rare Case
Tam metin
Şekil
Benzer Belgeler
Conducting poly- mers (CPs) have attracted considerable interest as electrochromic materials since ingenious modifications on the monomer can significantly alter the spectral
Comme on le sait, avec la propagation de l’islamisme,la miniature comme l’art de la calligraphie a trouvé son application dans l’illustration des livres en étant par
Lipomas are categorized as different subtypes, such as classic lipoma, lipomatosis, lipomatosis of the nerve, lipoblastoma, angiolipoma, myolipoma of the soft tissue,
Yapılan regresyon analizi sonucunda ise, sosyal sermaye değişkeninin alt boyutları olan yapısal sermaye, bilişsel sermaye ve ilişkisel sermaye boyutlarının örgütsel
In addition to this, the fact that the 25th World University Winter Games in 2011 and the European Youth Winter Festival in 2017 were in Erzurum has proved that the region has
Çe- kilen pozitron emisyon tomografisi/bilgisayarlı tomografi tetkikin- de sağ akciğer alt lob süperior segmentte, sağ akciğer orta ve alt lob bronşları komşuluğunda, her
Klinik uygulamada basýnç ülseri, yatak yarasý ya da dekübitus ülseri biçiminde adlandýrýlan bu lez- yonlar risk altýndaki kiþilerde çeþitli konumlarda ge- liþebileceði için
[r]
