beam computed tomography
Kaan Orhan, DDS, PhD,a,bBayram U. Sakul, PhD,cUlas Oz, DDS, PhD,dand Burak Bilecenoglu, DDS, PhD,eAnkara and Mersin, Turkey
UNIVERSITY OF ANKARA, NEAR EAST UNIVERSITY, ANKARA UNIVERSITY, AND UFUK UNIVERSITY
Objective. This study consists of anatomic research of the pterygoid hamulus (PH) using 3D cone beam computed tomography (CBCT) images reconstructed from a volumetric rendering program.
Study design. Three hundred ninety-six sides in the CBCT scans of 198 (115 men and 83 women) patients were retrospectively analyzed. DICOM data of the patients were transferred to a surface-rendering software so as to generate 3D hard tissue surface representations of PHs. The width, length, angle, and the distance between posterior nasal spine and tip of the PH were measured. In addition, the inclinations of PHs were also evaluated in sagittal and coronal planes of the 3D images. Pearson2and Student t test were performed for statistical analysis among age, localization, and measurements (P⬍ .05).
Results. The mean PH measurements of left and right sides were 1.72 (SD 0.94) and 1.87 (SD 1.17)-mm width, and the lengths were 5.48 (AD 1.94), and 5.40 (SD 2.0) mm, respectively, with no significant difference (P⬎ .05). All PHs were inclined toward the lateral side in the coronal plane, whereas PHs tended to incline toward the posterior rather than anterior in the sagittal plane (⬃78%). The results showed no statistically significant differences among age, localization, and measurements of PHs (P⬎ .05).
Conclusions. Knowledge about the morphology of these structures is helpful for the interpretation of imaging and provides valuable information in the differential diagnosis of untraceable pains in the oral cavity and pharynx. Because of potential problems owing to PH morphology and elongation, oral and maxillofacial radiologists should assess the radiographic images thoroughly. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;112:e48-e55)
A broad definition of pterygoid hamulus (PH) is a hooklike projection at the inferior end of each medial plate of the pterygoid process. The medial pterygoid plate of the sphenoid bone curves laterally at its lower extremity into a hooklike process, the PH, around which the tendon of the tensor veli palatini (TVP) muscle glides. Although the PH is, because of its bi-zarre shape, a striking feature of the skull base, it is still an unexplored region on the anatomical map.1,2Only a few studies have been conducted on the morphology of PH1-4; however, because of its close relationship to the
maxilla and oropharynx, it is of interest to all disci-plines that are involved with this region.1
The position, length, and inclination of PHs are of great importance for the function of several muscles: tensor veli palatini, palatopharyngeus, and upper part of the upper pharyngeal constrictor, pars pterygopharyn-gea. These muscles contribute to the separation of the oral from the nasal cavity during sucking and swallow-ing durswallow-ing growth and development and into adult-hood.2,3
Elongation of PH was also associated with a rare syndrome of PH that shows various and complex symp-toms in the palatal and pharyngeal regions and also causes pain and discomfort especially during swallow-ing. The term pterygoid hamulus syndrome was first used to describe a pain in the palatal and pharyngeal regions caused by an abnormally shaped PH by Hjørt-ing-Hansen et al.5,6 in 1987 with about 40 cases re-ported in the literature.4-15
Several studies were conducted on the position and morphology of PH in different populations. According to those studies, the length of the PH was found to be within the range of 4.9 to 7.2 mm.1-4,10 Putz and Kroyer1also reported the sagittal and transverse diam-eter of PH as 1.4 mm and 2.3 mm, respectively, whereas Sasaki et al.10also reported an elongated PH of
aAssociate Professor, Department of Oral, Tooth and Jaw Radiology, University of Ankara, Faculty of Dentistry, Ankara, Turkey. bAssociate Professor, Department of Oral, Tooth and Jaw Radiology, Near East University, Faculty of Dentistry, Mersin, Turkey. cProfessor, Department of Anatomy, Ankara University, Faculty of Dentistry, Ankara, Turkey.
dAssistant Professor, Department of Orthodontics, Near East Univer-sity, Faculty of Dentistry, Mersin, Turkey.
eAssistant Professor, Department of Anatomy, Ufuk University, Fac-ulty of Medicine, Ankara, Turkey.
Received for publication Oct 16, 2010; returned for revision Feb 17, 2011; accepted for publication Feb 22, 2011.
1079-2104/$ - see front matter © 2011 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2011.02.038
13 mm. Recently, it was found that the length increased in adult age and then decreased significantly again in the elderly population. Moreover, all studies reported that the positions of PHs are inclined laterally in the coronal plane.1-2
This information is important especially in tracing an unusual pain in the soft palate and pharyngeal region. Such a symptom in that area may be forming a complex that can include hearing disorders, difficulties in swal-lowing, headache, pain and clicking in the temporo-mandibular joints (TMJs), uncontrolled movements of the facial muscles, impacted teeth, trigeminal and glos-sopharyngeal neuralgia, stylo-hyoid ligament calcifica-tion, stylo-mandibular ligament inflammacalcifica-tion, tumors, cysts, herpes simplex, infection, otitis media, and so forth; thus, consideration of the PH as a pain-inducing factor should be included in the diagnosis.4,8,11 There-fore, it is important to know the average length, shape, and morphology of PHs for the population that guided us to conduct this research.
The detection of this area can be achieved by radi-ography (cephalometric radiradi-ography, submentovertex, Waters view, and so forth); however, identification of these structures by conventional radiography is exceed-ingly difficult because of superimposition and distor-tion. Today, computed tomography (CT) can be per-formed in axial and coronal planes with 3-dimensional (3D) views for diagnosis and treatment.8The 3D CT avoids superimposition and problems owing to magni-fication and offers visualization of the craniofacial structures with more precision than the 2D conven-tional methods.16-19
Despite various studies that were conducted on shape, length, and position of the PH, the anatomical relations of PH and the surrounding structures are rarely investigated.1-4Moreover, no studies were found
on cone beam computed tomography (CBCT) imaging with generated 3D skull representations using a sur-face-rendering program to identify and investigate PH. Thus, this study consists of anatomic research of PH using 3D CBCT images reconstructed form a volumet-ric rendering program.
MATERIAL AND METHODS
In the case that guided us to this research, a 26-year-old female was referred to our outpatient clinic because of painful and burning sensations in the soft palate and pharynx of 9 months’ duration. The patient’s history revealed that the symptoms started after traumatic re-moval of the right maxillary third molar. For this pain, she stated that she was referred to 10 to 15 different consultants, including ear, nose, and throat and maxil-lofacial surgeons, and various diagnoses were made, such as temporomandibular disorder (TMD) and glos-sopharyngeal neuralgia. The patient received nonsteroi-dal anti-inflammatory drugs and also an occlusal splint for TMD. However, the painful sensation was not re-solved during the 9 months.
Initial panoramic radiography of the patient showed neither a carious lesion nor any root fragment in the extraction site (Fig. 1) with slight degeneration on the left TMJ condyle. Intraorally, pain and a firm swelling were noted in palpation of the region. A decision was made to perform CBCT to obtain a more precise view of the region. Axial CBCT scan did not demonstrate any abnormality; however, coronal sections showed elongated PH in the right side. The 3D reconstructed CBCT images also showed an elongated PH (9.7 mm in length) with a sickle shape (Fig. 2). Infiltration of local anesthesia to the PH subsided pain; however, the symp-toms returned after the anesthetic was metabolized. A diagnosis of hamular pain was made. The patient was Fig. 1. Panoramic radiography of the patient showing no abnormality except flattening of left TMJ condyle.
referred for surgery of elongated PH. Following this case, we decided to conduct further research regarding PH morphology in our population.
For this purpose, 396 sides of 198 subjects (115 men and 83 women) ranging in age from 22 to 75 years (mean: 35.54) who had craniofacial CBCT scans were retrospectively investigated. CBCT images were taken for various purposes, such as preimplant imaging, para-nasal sinus examinations, or orthodontic purposes. The study’s protocol was carried out according to the prin-ciples described in the Declaration of Helsinki, includ-ing all amendments and revisions. Only the investiga-tors had access to the collected data. The institutional review board of the faculty reviewed and approved informed consent forms. There was no preference about gender regarding sample choice, however only Turkish patients were included in the study. Only high-quality scans were included. Images of low quality, such as scattering or insufficient accuracy of bony borders were excluded.
CBCT scans were made with a Newtom 3G (Quan-titative Radiology s.r.l., Verona, Italy). The imaging protocol used a 9-inch field of view to include the mandibular and maxillary anatomy. X-ray parameters of kV and ma are automatically determined from scout
views by the NewTom 3G. Depending on the size of the patient and the extent of beam attenuation, a vari-ation in exposure of up to 40% was possible.
The axial slice thickness was 0.3 mm, and the voxels were isotropic. The axial images were exported as a 512⫻ 512 matrix in DICOM file format and then were imported in Maxilim software version 2.3.0 (Medicim, Mechelen, Belgium). All constructions and measure-ments were performed on a 21.3-inch flat-panel color active matrix TFT medical display monitor (Nio Color 3MP, Barco, Belgium) with a resolution of 2048 ⫻ 1536 at 76 Hz and 0.2115-mm dot pitch operated at 10 b. A consultant experienced in 3D imaging made high-quality 3D hard tissue surface representations com-puted from the patients’ CBCT data set in several stages similar to previous studies20-22and examined all
images.
First, the bone and soft tissue surfaces were seg-mented by applying a threshold on the acquired image volume of radiographic densities. An attempt was made to reduce noise without reducing actual osseous anat-omy. The skulls were rendered as high-quality 3D hard tissue surface representations that were computed from the patients’ CBCT data set. The axial, sagittal, and Fig. 2. a, Axial CBCT scan showed no abnormality, whereas in b and c, coronal CBCT images showed elongated PH on the right side (arrows) with a normal PH on the left side (arrowhead). d, e, 3D reconstructed CBCT images also showed elongated PH (9.7 mm in length) with a sickle shape (arrow).
coronal CT radiographic slices were also superimposed over reconstructed 3D images (Fig. 3).
Measurements of 3D images were located and marked on the 3D surface-rendered volumetric image
study.1 First a line was drawn from the junction of medial pterygoid plate and PH parallel to the horizontal plane. Following the identification of the midpoint of this line, the length was measured starting from this point to the tip of the PH. The width of the PH was measured as the distance between the most prominence points of the PH in the coronal plane (Fig. 3, c).
In addition, the inclinations of PHs were evaluated in sagittal and coronal planes of the 3D images. The average degrees of inclinations in the sagittal and cor-onal planes were also calculated by means of the soft-ware according to horizontal plane following Putz and Kroyer’s study1(Fig. 4). The inclinations in the sagittal plane were also classified visually as anterior and pos-terior (Fig. 5), whereas inclinations in the coronal plane were classified as lateral or medial. All measurements were done 3 times by the same observer and the mean of these measurements were noted for analysis. The observer also performed the study 2 times with an interval of 2 weeks so as to detect intraobserver vari-ability.
Statistical analyses were carried out using the SPSS 12.0.1 (SPSS, Chicago, IL) software program. To as-sess intraobserver reliability, Wilcoxon matched-pairs signed-ranks test was used for repeated measurements of the observer. Pearson 2 and Student t test were performed for statistical analysis among age, localiza-tion, and measurements (P⬍ .05).
RESULTS
Repeated measurement of CBCTs indicated no sig-nificant intraobserver difference (P ⬎ .05). Intraob-server consistency was rated at 95% between 2 mea-surements. A total of 396 left and right sides of PHs were measured in 198 3D CBCT images. The findings are presented inTable I. The mean measurements of both left and right sides were 1.72 (SD 0.94) and 1.87 (SD 1.17)-mm width, respectively whereas the lengths were 5.48 (SD 1.94) and 5.40 (SD 2.0) mm, respec-tively without any significant difference (P ⬎ .05). There were also no statistically significant differences between left and right measurements between posterior nasal spine and tip of the PH of sides (P⬎ .05).
In the coronal plane, it was found that all PHs were inclined toward the lateral side (Fig. 3). However, in Fig. 3. a, b, Figure showing the measurements performed in
the study that were made on a generated 3D image from volumetric rendering software with superimposed coronal slices over reconstructed 3D image taken from CBCT data. c, Cropped image showing the length and width measurement in detail. w, width; l, length.
the sagittal plane, 43 (21.7%) PHs were inclined toward the anterior whereas 155 (78.3%) PHs tended to posterior on the left side. Similarly, on the right side, 45 (22.7%) PHs were inclined toward the an-terior, whereas 153 (77.3%) PHs tended to the pos-terior (Fig. 5).
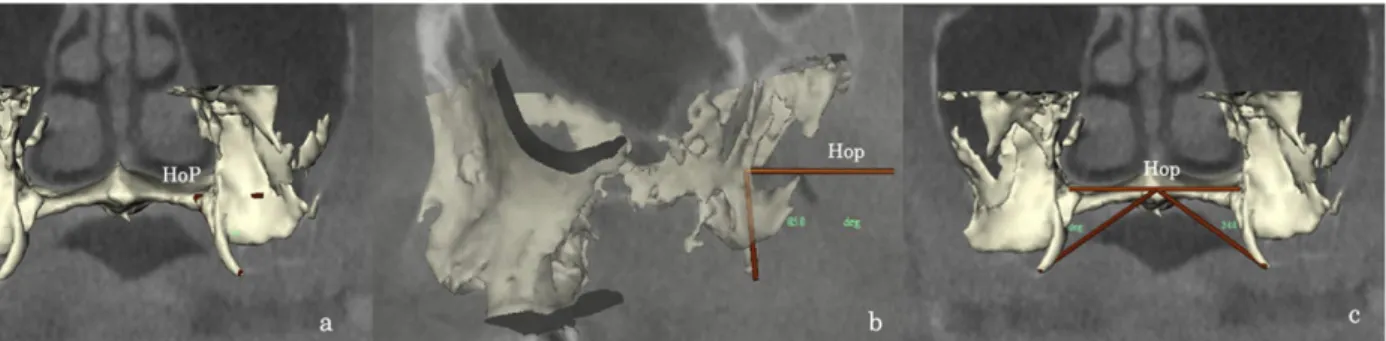
The average inclination in the sagittal plane and in the coronal plane showed no statistically significant difference (P ⬎ .05) (Table I). The angles between posterior nasal spine and tip of the PH were also mea-sured. The average degree for the left was 33.4° (SD 2.34) and 34.3° (SD 2.18) for right. Overall results also Fig. 4. a, 3D images showing angle and orientation of PH in the coronal plane, b, in the sagittal plane, and c, the angle between the posterior nasal spine and tip of the PH. HoP indicates horizontal plane.
Fig. 5. 3D reconstructed images showing a, anterior inclination and b, posterior inclination of PH (arrows).
Table I. Measurements of PH (mm) and standard deviations (SD) together with inclination of PH in coronal and
sagittal planes Measurements (mean⫾ SD) Left Right Total (mean⫾ SD) Male (mean⫾ SD) Female (mean⫾ SD) Total (mean⫾ SD) Male (mean⫾ SD) Female (mean⫾ SD) Width of the PH in coronal plane 1.72⫾ 0.94 1.73⫾ 0.83 1.70⫾ 1.07 1.87⫾ 1.17 1.93⫾ 1.44 1.79⫾ 0.60 Length of the PH 5.48⫾ 1.94 5.49⫾ 1.95 5.45⫾ 1.91 5.40⫾ 2.00 5.38⫾ 1.99 5.43⫾ 2.01 Posterior nasal spine to tip of PH 21.35⫾ 2.45 21.46⫾ 2.47 21.19⫾ 2.42 21.18⫾ 3.09 21.3⫾ 3.35 21.02⫾ 2.70 The average inclination in
coronal plane
52.5°⫾ 2.57° 53.2°⫾ 2.18° 51.9°⫾ 1.96° 53.9°⫾ 2.01° 54.1°⫾ 2.33° 53.8°⫾ 2.16° The average inclination in
sagittal plane 82.6°⫾ 3.08° 82.8°⫾ 3.19° 82.4°⫾ 2.90° 81.9°⫾ 3.25° 81.8°⫾ 3.40° 82.0°⫾ 2.99° Number of inclinations of PH in coronal plane Lateral Lateral 198 115 83 198 115 83 Medial Medial 0 0 0 0 0 0 Number of inclinations of PH in sagittal plane Anterior Anterior 43 (21.7%) 21 (18.3%) 22 (26.5%) 45 (22.7%) 28 (24.3%) 17 (20.5%) Posterior Posterior 155 (78.3%) 94 (81.7%) 61 (73.5%) 153 (77.3%) 87 (75.7%) 66 (79.5%) PH, pterygoid hamulus.
showed no statistically significant differences among gender, localization, and measurements of PHs (P ⬎ .05).
As a further evaluation, we divided the study group into 2 age groups, 22 to 55 and older than 55 years, so as to detect any differences according to age group.
Table II shows the data according to age group. The length of PH differed among the age groups. The pa-tient group older than 55 had shorter PH length than the 22- to 55-year-olds (P⫽ .054) (Table II). No further statistically significant difference was found among age and all measurements (P⬎ .05).
DISCUSSION
Anatomically, the PH and the edge of the medial pterygoid plate immediately superior to the PH, give rise to the origin of the superior constrictor muscle of the pharynx. The palate pharyngeus muscle originates in layers from the PHs, as well as from the border of the hard palate, and from fibers of the levator veli palatine muscle (LVP). It is generally stated that the lowest and most anterior fibers of LVP arise from the base of the pterygoid process and reach up to and a little beyond the base of the PH. In addition, TVP originating from the scaphoid fossa, the spine of palatal aponeurosis, and the lateral wall of the cartilaginous auditory tube winds its tendon around the PH in a groove with a synovial bursa between the tendon and the bone, inserts soft palate. The separation of the oral from the nasal cavity is accomplished by the elevation of soft palate with constriction of these muscles.3,8,22,23 As the ten-don of the TVP winds around the PH, a synovial bursa is situated between the tendon and the bone. This bursa
LVP contraction and Tubar part of TVP for stretching the palatal aponeurosis.2,7,8TVP also produces tension and elevation of soft palate, which the Tubar part is fixed to the hamulus. The position and morphology of PH are closely related to TVP function, which directly affects the width of the hard plate during swallowing. The inclination of the PH is also responsible for better tension of palatal apounerosis.2 Krmpotic´-Nemanic´ et al.2pointed out that if the hamulus remains short as in newborns, the surrounding muscles do not have firm support, which leads to uncontrolled narrowing of the upper pharynx, thus causing snoring and sleep apnea.
Besides, the elongated PH can also be the reason for pain and discomfort in the soft palate and pharynx.10Such cases have been previously reported. Gores15was the first to report the presence of pain caused by a long PH. The term pterygoid hamulus syndrome was then used to de-scribe a pain in the palatal and pharyngeal regions with about 40 cases reported in the literature.4-14
There is no consensus for the etiology of this syndrome. Previously, several etiologic factors stated bursitis of TVP or an osteophyte,4,9-12,14elongation of PH,4,10or consis-tent minimal trauma to the overlying structure.13 The trauma from swallowing a large bolus of food or from an overextended denture, anesthesia intubations, trauma dur-ing tooth brushdur-ing, bulimic patients, and “fellatio” in child abuse seem to be the cause of this syndrome.10,11In our case, the patient had her third molar extracted and the symptoms started after this operation.
Patients suffering from this syndrome have clinical signs, including pain and sensation of strangeness, burning and swelling of the hard/soft palate, elevated noise sensitivity, dysphagia, dysfunction of muscles, and difficulty in swallowing. Clinically, the PH region usually appears erythematous; sometimes the PH can be palpated as firm swelling or recognized as an en-largement under the mucosa of the soft palate.9-11 Fur-ther, the PH may have tenderness to palpation, which will be eliminated after anesthetic infiltration of the area. In our case, no erythematous appearance was seen; however, a firm swelling was noted and pain subsided after anesthetic infiltration.
The differential diagnosis of pain in the hard/soft palate and pharynx should include tumors, cysts, infec-tions, foreign bodies, elongated styloid syndrome, third
coronal plane
The average inclination in sagittal plane 82.8°⫾ 2.99° 81.7°⫾ 3.05° Number of inclinations of PH in coronal plane Lateral Lateral 166 32 Medial Medial 0 0 Number of inclinations of PH in sagittal plane Anterior Anterior 39 4 Posterior Posterior 127 28
molar eruption, TMJ diseases, muscular dysfunction, and also elongated PH.4,10,11
Several studies were conducted on the morphology of PH in different populations. Eyrich et al.4found the mean length of the left hamulus to be 5 mm and the right to be 4.9 mm. Putz and Kroyer1reported the
average length to be 7.2 mm and the sagittal and transverse diameter to be 1.4 mm and 2.3 mm, respec-tively. Sasaki et al.10 also reported an average PH length of 6.8 mm (SD 1.4 mm). Our results showed the mean length of PHs for left and right sides were 5.48 (SD 1.94) and 5.40 (SD 2.0) mm, respectively which is similar to other studies.1,4,10 There was no significant
difference according to gender and location. Sasaki et al.10 reported an elongated PH case of 13 mm. Our longest PH case was 10.9 mm in a male patient.
Recently Krmpotic´-Nemanic´ et al.2 conducted an extensive study on PH. They investigated the PH among 3 age groups: children (0-9), adults (21-59), and elderly (60-100). They found that children had the shortest PH length, on average 3.6 mm. The length increased in adults (6.9 mm) and then decreased sig-nificantly again to 5.0 mm in the elderly group. They also found no statistical difference for gender and for left and right sides.
Although no statistically significant difference was observed between the age groups, the P value was .054. From a numerical point of view, it can be concluded that older patients had shorter PH length than the younger patients. This is in line with Krmpotic´-Nemanic´ et al.’s2study, but does not coincide with Putz and Kroyer’s1 study, which reported that the PH in-creases in length to the beginning of adulthood, and thereafter remains unchanged throughout life.
There was only one study regarding the width and the inclination of the PH.1Putz and Kroyer1measured the sagittal diameter of PH as 1.4 mm, which is con-sistent with our width (sagittal diameter) measure-ments: 1.72 (SD 0.94) and 1.87 (SD 1.17) mm for left and right, respectively. The inclinations in their study were 75° in the sagittal plane and 58° in the coronal plane, which is also similar to our results (Table II). Each hamulus in this study was inclined laterally, as in previous studies.1-2The results showed no statistically significant differences among gender, localization, and measurements of PHs (P⬎ .05).
The elongated PH can be responsible for atypical pain in the soft palate and pharynx region. Radiographs of the PH and pterygomaxillary region should be ob-tained for the findings of osteophytes or hamular frac-ture or for any other abnormality. The detection of this area can be achieved by radiography (cephalometric radiography, Submentovertex, Waters view, conven-tional tomography). However, identification of these
structures by conventional radiography is exceedingly difficult because of superimposition and distortion. To-day, CT can be performed in axial and coronal planes with 3D views for diagnosis and treatment of this region.7-8,24The 3D CT avoids the superimposition and problems owing to magnification and offers visualization of the craniofacial structures with more precision than the 2D conventional methods.17-19,25 Despite these advan-tages, the effective dose of CT is much higher than the conventional radiographs and also expensive procedures and scanners are not easily accessible.19,26,27
In the past decade, CBCT was proposed for maxillo-craniofacial imaging.28-31The advantages of this imag-ing modality are the followimag-ing: lower radiation dose than traditional CT, the possibility of individualized overlap-free reconstructions, and DICOM data can be imported and exported for other applications.28Dental CBCT can be recommended as a dose-sparing tech-nique compared with alternative standard medical CT scans for common oral and maxillofacial radiographic imaging tasks. Effective dose (ICRP 2007) from a standard dental protocol scan with the traditional CT was from 1.5 to 12.3 times greater than comparable medium field of view dental CBCT scans.32It was also stated that effective dose and dose to the main portions of the head and neck were higher for traditional CT than for CBCT. Image quality of CBCT was judged to be equivalent to that of traditional CT for visualizing the maxillofacial structures.33-37
From the radiation point of view, CBCT examina-tions can be used instead of CT to evaluate this region. When 3D imaging is required to visualize anatomic structures, such as processes of sphenoid bone, hard/ soft palate, and oropharynx, CBCT should be preferred over a CT image.
CONCLUSIONS
Knowledge about the morphology of these structures is helpful for the interpretation of imaging and provides valuable information in the differential diagnosis of untraceable pains in the oral cavity and pharynx. Be-cause of potential problems owing to PH morphology and elongation, oral and maxillofacial radiologists should assess the radiographic images thoroughly. Sim-ilar studies will provide useful information to better understand the anatomy and diseases regarding the PH. REFERENCES
1. Putz R, Kroyer A. Functional morphology in the pterygoid hamulus. Ann Anat 1999;181:85-8.
2. Krmpotic´-Nemanic´ J, Vinter I, Marusic´ A. Relations of the pterygoid hamulus and hard palate in children and adults: ana-tomical implications for the function of the soft palate. Ann Anat 2006;188:69-74.
3. Abe M, Murakami G, Noguchi M, Kitamura S, Shimada K, Kohama GI, et al. Variations in the tensor veli palatini muscle
8. Shankland WE 2nd. Bursitis of the hamular process. Part II: diagnosis, treatment and report of three case studies. Cranio 1996;14:306-11.
9. Kronman JH, Padamsee M, Norris LH. Bursitis of the tensor veli palatini muscle with an osteophyte on the pterygoid hamulus. Oral Surg Oral Med Oral Pathol 1991;71:420-2.
10. Sasaki T, Imai Y, Fujibayashi T. A case of elongated pterygoid hamulus syndrome. Oral Dis 2001;7:131-3.
11. Ramirez LM, Ballesteros LE, Sandoval GP. Hamular bursitis and its possible craniofacial referred symptomatology: two case re-ports. Med Oral Patol Oral Cir Bucal 2006;11:E329-33. 12. Salins PC, Bursitis BGP. A factor in the differential diagnosis of
orofacial neuralgias and myofascial pain dysfunction syndrome. Oral Surg Oral Med Oral Pathol 1989;68:154-7.
13. Charbeneau TD, Blanton PL. The pterygoid hamulus. A consid-eration in the diagnosis of posterior palatal lesions. Oral Surg Oral Med Oral Pathol 1981;52:574-6.
14. Fu Y, Peng J, Chen W. The pterygoid hamulus syndrome with the main discomfort of pharynx. Lin Chuang Er Bi Yan Hou Ke Za Zhi 2004;18:134-5.
15. Gores RJ. Pain due to long hamular process in the edentulous patient. Lancet 1964;84:353-54.
16. Baumrind S, Frantz RC. The reliability of head film measure-ments. 1. Landmark identification. Am J Orthod 1971;60:111-27. 17. Baumrind S, Frantz RC. The reliability of head film measure-ments. 2. Conventional angular and linear measures. Am J Or-thod 1971;60:505-17.
18. Kumar V, Ludlow JB, Mol A, Cevidanes L. Comparison of conventional and cone beam CT synthesized cephalograms. Den-tomaxillofac Radiol 2007;36:263-69.
19. Sandler PJ. Reproducibility of cephalometric measurements. Br J Orthod 1988;15:105-10.
20. Swennen GR, Schutyser F, Barth EL, De Groeve P, De Mey A. A new method of 3-D cephalometry part I: the anatomic Carte-sian 3-D reference system. J Craniofac Surg 2006;17:314-25. 21. Periago DR, Scarfe WC, Moshiri M, Scheetz JP, Silveira AM,
Farman AG, et al. Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod 2008;78:387-95. 22. Ludlow JB, Gubler M, Cevidanes L, Mol A. Precision of
cephalo-metric landmark identification: cone-beam computed tomography vs conventional cephalometric views. Am J Orthod Dentofac Or-thop 2009;136:312-13.
23. Moore KL, Agur MRA, editors. Essential clinical anatomy. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2007. p. 553. 24. Curtin HD, Som PM, Braun FI, Nadel L. Skull base. In: Som PM, Curtin HD, editors. Head and neck imaging. 3rd ed. St. Louis: Mosby; 1996. p. 1250.
computed tomography and digital cephalometric radiography. Am J Orthod Dentofac Orthop 2005;128:803-11.
28. Moreira CR, Sales MA, Lopes PM, Cavalcanti MG. Assessment of linear and angular measurements on three-dimensional cone-beam computed tomographic images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:430-6.
29. Farman AG, Scarfe WC. Development of imaging selection criteria and procedures should precede cephalometric assessment with cone-beam computed tomography. Am J Orthod Dentofac Orthop 2006;130:257-65.
30. Brown AA, Scarfe WC, Scheetz JP, Silveira AM, Farman AG. Linear accuracy of cone beam CT derived 3D images. Angle Orthod 2009;79:150-7.
31. Mozzo P, Procacci C, Tacconi A, Martini PT, Bergamo IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 1998;8:1558-64. 32. Ludlow JB, Ivanovic M. Comparative dosimetry of dental CBCT
devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:106-14. 33. Carrafiello G, Dizonno M, Colli V, Strocchi S, Pozzi-Taubert S,
Leonardi A, et al. Comparative study of jaws with multislice computed tomography and cone-beam computed tomography. Radiol Med 2010;115:600-11.
34. Loubele M, Bogaerts R, Van Dijck E, Pauwels R, Vanheusden S, Suetens P, et al. Comparison between effective radiation dose of CBCT and MSCT scanners for dentomaxillofacial applications. Eur J Radiol 2009;71:461-8.
35. Silva MA, Wolf U, Heinicke F, Bumann A, Visser H, Hirsch E. Cone-beam computed tomography for routine orthodontic treat-ment planning: a radiation dose evaluation. Am J Orthod Dento-fac Orthop 2008;133:e1-5.
36. Suomalainen A, Kiljunen T, Käser Y, Peltola J, Kortesniemi M. Dosimetry and image quality of four dental cone beam computed tomography scanners compared with multislice computed to-mography scanners. Dentomaxillofac Radiol 2009;38:367-78. 37. Roberts JA, Drage NA, Davies J, Thomas DW. Effective dose
from cone beam CT examinations in dentistry. Br J Radiol 2009;82:35-40.
Reprint requests: Kaan Orhan, DDS, PhD
Department of Oral, Teeth and Jaw Radiology University of Ankara
Faculty of Dentistry Ankara, Turkey [email protected]