Technique
Transcavum septum pellucidum interforniceal approach
for the colloid cyst of the third ventricle
Operative nuance
Erdener Timurkaynak, MD
a, Yusuf I˙zci, MD
b,4, Feridun Acar, MD
ca
Department of Neurosurgery, Ufuk University, 06520 Ankara, Turkey b
Department of Neurosurgery, Gu¨lhane Military Medical Academy, 06018 Ankara, Turkey c
Department of Neurosurgery, Pamukkale University, 20100 Denizli, Turkey Received 10 May 2005; accepted 8 March 2006
Abstract Background: Despite their unfavorable locations, lesions of the third ventricle can be successfully removed via an interhemispheric, transcallosal approach. In cases with normal ventricular anatomy, this approach requires unilateral or bilateral identification of the foramen of Monro.
Technique: However, in the presence of abnormal ventricular configuration such as cavum septum pellucidum (CSP), this basic knwoledge needs to be modified. After routine callosotomy, there may be a confusion while entering the CSP due to the invisualization of ventricular landmarks such as the foramen of Monro, thalamostriate vein, and choroid plexus. The floor of the CSP is formed by the fornices, and a direct approach to the interforniceal area is easier via the CSP. But the interforniceal approach is not a routine way to reach the third ventricle, which has higher risks than other modalities. Conclusion: This approach should be planned and used in selected cases of the CSP. Opening of the walls of CSP is recommended both to expose both the foramen of Monro and to gain safe access to the third ventricle before manipulating the interforniceal area.
D 2006 Elsevier Inc. All rights reserved.
Keywords: Cavum septum pellucidum; Interforniceal approach; Third ventricle; Tumor
1. Introduction
The third ventricle is one of the most surgically inaccessible areas in the brain. It is impossible to reach its cavity without incising some neural structures[11]. Various methods to reach the third ventricle through the interhemi-spheric-transcallosal approach include transforaminal,
trans-choroidal fissure and interforniceal exposures [1-3,5].
Anatomical and surgical studies on the transcallosal approaches well define this surgery in cases with normal
ventricular anatomy [7,10]. However, in the presence of
anatomical variation such as CSP and CV, entrance to the cavum may confuse the inexperienced surgeon in this region. Because of the anatomical orientation, the surgeon may decide to stay in the CSP and reach the floor to open
the interforniceal space [9]. This strategy needs to be
discussed. The interforniceal approach has the advantage of giving access to the central portion of the third ventricle behind the foramen of Monro by displacing, rather than transecting, the fibers in the fornix [6]. Before deciding on the interforniceal approach, all routes, such as the trans-foramen of Monro and transchoroidal fissure, should be eliminated meticulously.
The midline anatomical structures including the fornices can be distorted by a third-ventricle tumor. The presence of CSP or CV does not imply reaching the interforniceal region in the midline. A disorientation in the CSP or CV may cause forniceal damage, which may result in serious memory deficits[4]. This disorientation may also cause injury to the internal cerebral veins, which may lead to mortality[8]. The walls of the CSP (the septal leaves) should be opened bilaterally above the fornices to visualize both the ventricles and the foramina of Monro to ensure the pathology and anatomy-oriented midline.
0090-3019/$ – see front matterD 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.surneu.2006.03.033
Abbreviations: CSF, cerebrospinal fluid; CSP, cavum septum pellucidum; CV, cavum vergae; MRI, magnetic resonance imaging.
4 Corresponding author. Tel.: +90 312 304 53 18; fax: +90 312 304 53 00. E-mail address: [email protected] (Y. I˙zci).
Surgical Neurology 66 (2006) 544 – 547
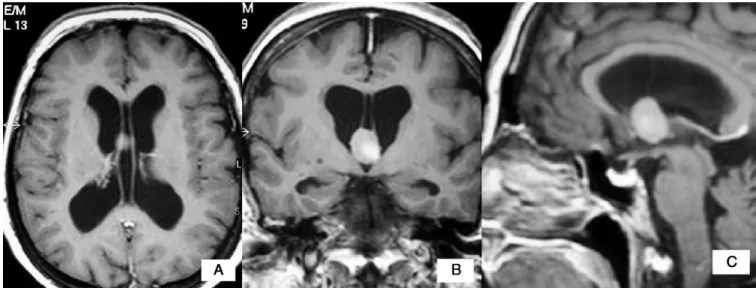
In this paper, the transcavum septum pellucidum interforniceal approach to the third ventricle of a 55-year-old female patient with colloid cyst is demonstrated using pictures and video recordings. She was referred to our department with the diagnosis of a mass lesion located in the third ventricle. She had the complaints of headache, nausea, vomiting, and dizziness, which started a week previously. The neurologic examination revealed no deficit. Magnetic resonance imaging with contrast showed a hyperintense, contrast-enhancing, cystic mass lesion in the third ventricle
in T1-weighted images (Fig. 1). There was a moderate
hydrocephalus with a CSP and CV variation. 2. Surgical procedure
2.1. Interhemispheric dissection, callosotomy, and exploration of the CSP
The bone flap was planned so that one third is posterior to the coronal suture and two thirds is anterior to it. Once the dura has been separated from the brain to the sagittal sinus, the leading edge of the hemisphere is retracted laterally away from the midline in a careful stepwise fashion. There were no bridging veins to the superior sagittal sinus. With gentle pressure, the retractor was placed on the cottonoid and advanced further forward into the interhemispheric fissure. After the interhemispheric dissection, we performed a 1- to 2-cm oval callosotomy. We did not observe any intraventricular structure after the callosotomy, and we understood that access to the CSP was achieved. There were CSF pulsations along the walls of the CSP (Fig. 2). The forniceal bodies were visible on the floor of the CSP. The forniceal prominences were lifted up by the pressure of mass lesion in the third ventricle. To obtain a better approach, we dissected and opened 2 septal leaves of CSP. Both lateral ventricles were observed and both foramina of Monro were visualized. The tumor tissue was not visible
through both foramina of Monro. We decided to make an interforniceal dissection to expose the tumor tissue. 2.2. Interforniceal dissection and tumor removal
Before starting the interforniceal approach, the attach-ments of septum pellucidum were cleared from the fornices to reveal the interforniceal raphe. It was thinned by tumor pressure and was dissected bluntly using a microdissector. Then, we opened the thin layer of interforniceal raphe using a microscissor. To avoid any damage to the fornices and hippocampal commissure, the separation was limited to 1.5 cm. After the interforniceal opening, the capsule of the third-ventricle colloid cyst was observed (Fig. 3). Most part of the cyst was located posterior to the foramen of Monro. The cyst wall was attached to the internal cerebral veins.
Fig. 1. Magnetic resonance imaging scan of the patient in axial (A), coronal (B), and sagittal (C) planes showing the hyperintense contrast-enhancing mass lesion in the third ventricle with enlarged lateral ventricles and CSP and CV variation.
Fig. 2. View of CSP and fornices before opening.
The cyst wall was opened, and the yellow-colored content of the cyst was removed totally in piecemeal fashion using biopsy forceps and microsuction tip. During the cyst removal, small cottonoids were placed between the cyst wall and the third ventricle to prevent blood leakage into the CSF pathways. The attachments have been removed by a microscissor and a microdissector. After the cyst removal, the third ventricle and internal cerebral veins were exposed (Fig. 4). Both lateral ventricles and the connections of bilateral foramina of Monro to the third ventricle were
easily visualized (Fig. 5). The postoperative period was uneventful, and the patient was discharged without any memory deficit.
3. Conclusion
Interforniceal approach is not a standard approach to the third ventricle and should not be performed by inexperi-enced surgeons. Preoperative planning is very important in the third-ventricle approach, but in some cases like this, it may be inadequate and the approach can be changed during surgery. Alternative surgical techniques, such as endoscope-assisted surgery or the use of neuronavigation and favorable surgical positioning, must also be considered preoperatively. Interforniceal approach should not be a routine method, as it can result in damage to the fornices, internal cerebral veins, and posterior medial choroidal arteries. In patients with CSP and/or CV, the interhemispheric, transcallosal, interforniceal approach may be considered, but is known to have higher risks for bilateral forniceal injury and for internal cerebral veins. It should be noted that other options should be strongly considered. If an interforniceal approach is considered preoperatively, the added risks inherent to this procedure should be discussed in the informed-consent process.
Transcallosal-interhemispheric approach to the lesions of the third ventricle requires a detailed knowledge of relevant anatomy. Orientation is essential. In normal anatomic conditions, the transforamen of Monro approach and trans-choroidal fissure approach are much safer methods for reaching the roof and anterior part of the third ventricle. In the presence of CSP variation, it may confuse the surgeon
Fig. 4. The third ventricle and vascular structures after splitting the body of fornix.
Fig. 5. View of both lateral ventricles and foramina of Monro after total removal of the colloid cyst.
Fig. 3. The colloid cyst is exposed between the 2 fornices.
E. Timurkaynak et al. / Surgical Neurology 66 (2006) 544 – 547 546
and make the intraventricular orientation difficult. Before deciding on the interforniceal approach, all possibilities (transforamen of Monro and transchoroidal fissure) should be checked carefully. Remaining in the CSP does not provide a safe interforniceal approach to the third ventricle. The walls of the CSP should be opened bilaterally to visualize both lateral ventricles and foramina of Monro for the decision of the approach and to prevent the prolapsus of septal leaves. The fornices must be dissected carefully from each other.
Appendix A. Supplementary data
Supplementary data associated with this article can
be found, in the online version, at doi:10.1016/j.surneu.
2006.03.033. References
[1] Apuzzo MLJ, Giannotta SL. Transcallosal interforniceal approach. In: Apuzzo MLJ, editor. Surgery of the third ventricle. Baltimore7 Williams & Wilkins; 1987. p. 354 - 80.
[2] Apuzzo MLJ, Chikovani OK, Gott PS, Teng EL, Zee C-S, Giannotta SL, Weiss MH. Transcallosal, interforniceal approaches for lesions affecting the third ventricle: surgical considerations and consequences. Neurosurgery 1982;10:547 - 54.
[3] Cossu M, Lubinu F, Orunesu G, Pau A, Sehrbundt Viale E, Sini G, Turtas S. Subchoroidal approach to the third ventricle: microsurgical anatomy. Surg Neurol 1984;21:325 - 31.
[4] D’Esposito M, Verfaellie M, Alexander MP, Katz DI. Amnesia following traumatic bilateral fornix transection. Neurology 1995; 45:1546 - 50.
[5] Lavyne MH, Patterson Jr RH. Subchoroidal trans-velum interpositum approach. In: Apuzzo MLJ, editor. Surgery of the third ventricle. Baltimore7 Williams & Wilkins; 1987. p. 381 - 97.
[6] Rhoton Jr AL. The lateral and third ventricles. Neurosurgery 2002;51(4 Suppl):207 - 72.
[7] Timurkaynak E, Rhoton Jr AL, Barry M. Microsurgical anatomy and operative approaches to the lateral ventricles. Neurosurgery 1986; 19(5):685 - 723.
[8] Ture U, Yasargil MG, Al-Mefty O. The transcallosal-transforaminal approach to the third ventricle with regard to the venous variations in this region. J Neurosurg 1997;87:706 - 15.
[9] Von Cramon DY, Mqller U. The septal region and memory. In: Cohadon F editor. Advances and technical standards in neurosurgery. New York7 Springer; 1998. p. 3 - 40.
[10] Winkler PA, Ilmberger J, Krishnan KG, Reulen HJ. Transcallosal interforniceal-transforaminal approach for removing lesions occupy-ing the third ventricular space: clinical and neuropsychological results. Neurosurgery 2000;46(4):879 - 88 [discussion 888-90].
[11] Yamamoto I, Rhoton Jr AL, Peace DA. Microsurgery of the third ventricle: Part I. Microsurgical anatomy. Neurosurgery 1981;8(3): 334 - 56.
Commentary
The surgical management of colloid cysts requires an in-depth understanding of third-ventricle anatomy and the
numerous surgical approaches to safely reach this area. Although the interforniceal approach is generally considered a higher risk procedure compared to others, this case demonstrates that it may be an appropriate choice in the setting of a CSP. The decision as to the optimal surgical approach for any given colloid cyst should be based on the location of the cyst, imaging characteristics of its contents, the size of the ventricles, and the surgeons’ experience and access to supportive technology. It is likely that this cyst could have been completely removed by other approaches requiring less brain retraction. This is an important technical note in that it reminds us that, in expert hands, the interforniceal approach provides an excellent exposure to the attachment point of the cyst to the tela choroidea and the procedure can be performed with minimal morbidity.
Marvin Bergsneider, MD Department of Neurosurgery, UCLA Los Angeles, CA 90095, USA
This manuscript describes a case with a colloid cyst in the third ventricle removed by the CSP interforniceal approach. The other approaches to the third ventricle include transforaminal, transchoroidal fissure and trans-lamina terminalis, the last of which the authors did not describe in this paper . The most important vital structures when approaching toward the third ventricle are the fornix and the internal cerebral vein.
If the foramen of Monro is enlarged by the lesion, the transforaminal approach to remove the lesion is feasible. The transchoroidal fissure approach is also recommended if the internal cerebral vein and the fornix in the ipsilateral side can be preserved. The interforniceal route has an advantage in that it can approach the third ventricle directly, but it also has a major risk of damaging the bilateral fornices. As the authors stressed, this approach should be used if other approaches are not favorable for the lesion in the third ventricle and it is most recommended in the case with the cavum septi pellucidi. On the other hand, if the lesion does not exist in the cepharad but exists in the anterior portion of the third ventricle, the translamina terminalis approach is the most favorable without the risk of damaging the fornix or the internal cerebral vein.
The authors are to be congratulated for their contribution to surgery of the lesion in the third ventricle without damaging the important structures of the fornix and the internal cerebral vein.
Tsuneyoshi Eguchi, MD Department of Neurosurgery Kameda General Hospital Kamogawa, Chiba 296, Japan