Available
online
at
ScienceDirect
www.sciencedirect.com
Original
Article
Detection
of
cholesteatoma:
High-resolution
DWI
using
RS-EPI
and
parallel
imaging
at
3
tesla
O.
Algin
a,b,∗,
H.
Aydın
c,
E.
Ozmen
d,
G.
Ocakoglu
e,
S.
Bercin
f,
D.A.
Porter
g,
A.
Kutluhan
faDepartmentofRadiology,AtaturkTrainingandResearchHospital,06050Ankara,Turkey bNationalMRResearchCenter(UMRAM),BilkentUniversity,Bilkent,Ankara,Turkey cDepartmentofRadiology,Dr.AbdurrahmanYurtaslanOncologyHospital,AnkaraTurkey dDepartmentofRadiology,IstanbulUniversity,CerrahpasaMedicalSchool,Istanbul,Turkey eDepartmentofBiostatistics,UludagUniversity,MedicalFaculty,Gorukle,Bursa,Turkey
fOtorhinolaryngologydepartment,YıldırımBeyazıtUniversity,AtaturkTrainingandResearchHospital,Ankara,Turkey gSiemensAG,HealthcareSector,Erlangen,Germany
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Availableonline30June2017 Keywords: Readout-segmentedEPI RESOLVE Diffusion-weightedimaging Cholesteatoma Single-shotEPI
a
b
s
t
r
a
c
t
ThepurposeofthisstudyistoevaluatetheimpactofRS-EPI-DWIinthedetectionofcholesteatomaand tocomparewithsingle-shotecho-planarDWI(SS-EPI-DWI).Diffusion-weightedandapparent diffusion-coefficient(ADC)imageswereobtainedusingRS-EPIandSS-EPItechniquesin30patients.Presenceof cholesteatoma(3pointscale),amountofartefacts(4pointscale),visibility(4pointscale),andADC valuesofthelesionswereassessed.Theresultsofbothtechniqueswerecomparedwitheachotherand gold-standard(GS)testresults.LesionvisibilityandpresenceofartefactscoresofRS-EPI-DWIgroup weresignificantlydifferentfromthoseoftheSS-EPIgroup.RS-EPI-DWIimageshadfewerartefactsand highervisibilityscores.Thesensitivity,specificity,negative/positive-predictive,andoverall-agreement valuesofRS-EPI-DWItechniquewere100%,78%,100%,74%,and87%;respectively.Thesevaluesfor SS-EPI-DWItechniquewere91%,60%,88%,67%,and75%;respectively.Also,thesevalueswerehigher onaxialplanethancoronalplaneimagesforADCmeasurements.Basedongold-standardtestfindings, agreementvaluesweregood(=0.74)forRS-EPI-DWIandmoderateforSS-EP-DWI(=0.50)techniques (P<0.001forboth).TheRS-EPI-DWItechniqueallowsahigherspatial-resolutionandthistechniqueis lesssusceptibletoartefactswhencomparedwithSS-EPItechnique.
©2017ElsevierMassonSAS.Allrightsreserved.
Introduction
Surgical treatment of the cholesteatoma is more functional andconvenient whenit is diagnosed earlier[1–3].The surgery is less successful when the diagnosis is not clear and/or the size/locationofthelesionisnotexactlyknown[1–5].Otoscopy, oto-endoscopyandmicroscopyaresomeoftheclinicalprocedures usedforthediagnosisofcholesteatoma[1].High-resolution com-putedtomography(HRCT)anddiffusion-weightedimaging(DWI) arethemostcommonlyusedimagingtechniquesforthediagnosis ofthecholesteatoma[3–6].
∗ Corresponding authorat: Departmentof Radiology,AtaturkTraining and ResearchHospital,06050Ankara,Turkey.
E-mailaddresses:[email protected](O.Algin),
[email protected] (H. Aydın), [email protected] (E. Ozmen), [email protected] (G. Ocakoglu), [email protected] (S. Bercin), [email protected](D.A.Porter),[email protected](A.Kutluhan).
Single-shotecho-planarimaging(SS-EPI)basedDWIhas sev-eralweaknessesincludinglimitedspatialresolutionandgeometric distortion due tothesusceptibilityartefacts within the tempo-ralbones[7].Geometricdistortionmayleadtofalsenegativeor positive resultsby preventingtheoptimalevaluationof middle earcavityandthoseartefactsaremoreprominentat3tesla(T) devices[2,8].Newtechniqueshavebeendevelopedtoavoidthese artefactsincludingmulti-shotecho-planarimaging(EPI),non-EPI orperiodicallyrotatedoverlappingparallellineswith enhanced-reconstruction(PROPELLER)techniques[2,7,9,10].
Readout-segmentedecho-planarimagingbased(RS-EPI) tech-niquewasintroducedbyPorter etal.[8].Thismethodprovides imageswithlessartefactsandhigherresolutionfortheevaluation ofbrain,brainstemandthebreast[11–13].However,tothebest ofourknowledge,itseffectivenessintheevaluationofmiddle-ear cholesteatomahasnotbeenestablished,yet.
Theaimofthispreliminaryprospectiveresearchstudywasto evaluatetheefficacyofDWIobtainedwithRS-EPItechniqueat3T MRdeviceindetectingcholesteatomaandtocomparethis tech-niquewithSS-EPImethod.
http://dx.doi.org/10.1016/j.neurad.2017.05.006
Materialsandmethods StudypopulationandMRexams
This study was approved by the institutional review board andwrittenconsentwasobtainedfromeachofthepatients.For thestudy,49patientswiththeprediagnosisofcholesteatomaat otoscopyor HRCT wereevaluatedusing 3T MRmachine (Tim-Trio,Siemens,Erlangen,Germany)duringthree-yearperiodwith multi-channel birdcage head coil. All cases were scanned in a supinepositionwithoutpre-imagingpreparation. ThesameMR protocol was used for all subjects. Pregnant women and the patientswithcardiacpacemaker/metallicimplantor claustropho-biawereexcludedfromthestudy.Moreover,19patientsinwhom cholesteatomawasdetectedbyMRimagingat3T,wereexcluded sincetheydidnotacceptsurgicaltreatmentorhadco-morbidities thatmadethesurgeryimpossible.Asaresult,thefinalpatient num-berincludedinthestudywas30(medianage:42[12–65years]; 11male,19female).Medianageswere48(13–65)and42(12–63) yearsformalesandfemales,respectively.Nine(30%)ofthepatients includedinthestudyhadpreviousearsurgeryforcholesteatoma.
After sagittal plane three-dimensional (3D) T1 weighted (W) and T2W sequences with isotropic voxel sizes (<1mm3), axial/coronalplanesSS-EPIandRS-EPIsequenceswereperformed withcomparable imaging parameters (Table1).SS-EPI and RS-EPI techniqueswere used for obtainingimages from thesame anatomicregionswiththesameimagethicknessandarrangedto beparalleltothelinethatconnectedtheinternalacoustic chan-nels.ImageswereacquiredwithBvaluesof0,500,1000s/mm2and ADCimageswerecalculatedusingsoftwareprovidedbythe man-ufacturer.SequenceparametersanddetailsoftheMRIprotocolare presentedinTable1.Totalimagingtimeforthe3TMRimagingwas approximately30minutes.
Evaluationofpatients’data
AlloftheMRimagesweretransferredandevaluatedbytwo radiologistswithlong-standingexperience(>9years)intemporal bone imaging,who wereblindedtothepatients’ clinical infor-mation,previousimaging data,and/orsurgicalfindings, usinga Leonardoworkstation(Siemens,Erlangen,Germany).
ThefirstsessionwasdesignedastheSS-EPIsessionwhereall theimageswereobtainedexcludingtheRS-EPIimages,evaluated andscoredregardingthepresenceofcholesteatoma(3pointscale) andlesionvisibility(4pointscale)asexplainedbelow.
Cholesteatomascoring
Score0:normalmiddleearcavity(negativeresult). Score1:suspiciousfindings(indefinite).
Score2:definitivecholesteatoma(positiveresult). Lesionvisibility-conspicuityscores
Score0:lesionisnotvisible.
Score 1: suspicious lesion(s) is/are exist but cannot be dis-criminatedfromthesurroundingtissueoris/arenotseenclearly (inadequateorpoorvisibility).
Score2:discriminationisgood.
Score3:excellentlesionconspicuityorvisibility.
Inthesecondsession(theRS-EPIsession);thescoring proce-durementionedabovewasperformedalsoforRS-EPIimagesand T1W/T2Wimages.Inthissession,theSS-EPIsequenceswerenot evaluated.Toavoid biasthat mightbeoriginatedfrommemory effects,noneofthescoringsessionshad asimilarpatientorder whilstevaluating.
The diagnosis of cholesteatoma on MRI was based on the presenceof increasedsignalintensityonb value=1000s/mm2,
decreasedsignalintensityonADCandasoft-tissuemassseenon 3DT1WorT2Wimageswithoutevidenceofotherpathology(such ascholesterolgranuloma).Theintensityoflesionwasdecidedby comparingwiththeintensityofcerebellumonbothb1000andADC images.Incaseoftheexistenceofahyperintenselesiononb1000 images,wemeasuredthecorrespondingADCvaluesinaselected regionofinterest(ROI).For eachlesion,theROIwasdefinedto encompassthemaximalamountofthelesionwithoutexceeding thelesion’smargins.Thesizeofthelesionwasmeasuredinthe greatestdiametersonaxialandcoronalb1000images.
Inthesessionsmentionedabove;theartefactsonDWIandADC imageswerealsoevaluated.DuringtheseassessmentsofbothEPI techniques,theexistenceandamountofthemotionartefacts, geo-metricdistortions,andimageblurringadjacenttothemiddleear cavitywerescoredvisuallyasdescribedbelow.
Artefactscoring
Score 0:unacceptable(DWIquality severelydeterioratedby artefacts).
Score 1: acceptable (there are prominent artefacts however imagescanbeevaluatedproperly).
Score2:good(therearefewartefactsandthoseartefactsdonot preventimageevaluation).
Score3:excellent(artefact-freeimaging).
Forallscorings,thefinaldecisionswereobtainedwith consen-sus.
All patientswho had cholesteatoma on MRI were operated within 3 months following 3T MR examination. The surgical findings wereobtainedfromthe surgicalreports oftwo differ-entexperiencedotorhinolaryngologyteams.Surgicalresultswere acceptedasgold-standard(GS)testresults.However,mostofthe patientswhodidnothavecholesteatomaon3TMRexaminations had final diagnosis with clinical, temporal-bone CT, contrast-materialenhanced MRIwithdelayedimaging,and/orfollow-up (meanlengthoffollow-upis41-month)findingsbythesametwo radiologistsandotorhinolaryngologyteamswithconsensus,since those patientswere notoperatedon.Surgicalresultsor above-mentionedfinaldecisionswereanalysedandcomparedwithSS-EPI andRS-EPIfindings.
Statisticalanalysis
Continuous variables were expressed with median (minimum–maximum) values. Agreements between visibility, artefact,presenceofcholesteatomascoresandADCvalues were evaluated by using Cohen’s kappa and intra-class correlation coefficient(ICC).Between-groupcomparisons ofRS-EPI and SS-EPIvalues wereperformed byusingtheMann WhitneyU-test. ThediagnosticaccuracyoftheSS-EPIandtheRS-EPIsequences wasdescribedbysensitivity, specificityandpositive &negative predictivevalue(PPV&NPV).Cut-offpointsofADCvalueswere determined by using ROC (receiver operating curve) analysis. Areaunderthecurve,sensitivity,specificity,positiveandnegative predictivevalueswerealsoreportedasp-values.Inallstatistical analyses, thelevel of significancewas setto␣=0.05.Statistical analyseswereperformedwithSPSSsoftwareversion21.0(Chicago, IL,USA).
Results
Therewasnosignificantdifferencebetweenmalesandfemales in terms of age (P=0.226). According to the GS test results, cholesteatomawasdetectedin21patients.Twoofthesepatients havebilateralcholesteatomas(thesepatientshadsurgerydoneon both ears),whileunilateral diseasewasexisted intheother19 patients(Figs.1and2).Thus,cholesteatomawasdetectedin23
Table1
3teslaMRIprotocolofthestudy.
Sequences/parameters STIR 3D-MPRAGE 3D-SPACE SS-EPI RS-EPI TR/TE(ms) 5100/81 2100/2.36 3000/423 6500/111 5000/91–124
TI(ms) 150 1000 – – –
Slicethickness(mm) 3 0.66 0.78 3 3
FOV(mm) 180×180 210×210 200×200 218×218 236×236
Acquisitiontime(min.) 2 6 5 3 5
NEX 2 1 1 4 1
Numberofslices 16 256 208 30 30
Flipangle(◦) 120 8 Variant 180 180
Imagingplane Axial Sagittal Sagittal Axial-coronal Axial-coronal
Distancefactor(%) 10 – – 20 20
PATfactor 2 2 2 2 2
PATmode GRAPPA GRAPPA GRAPPA GRAPPA GRAPPA
Bvalues – – – 0,500,1000 0,500,1000
Fat-suppression – + – + +
Baseresolution 384 320 256 192 160
Phaseresolution(%) 80 100 100 100 100
3D-SPACE:T2-weighted(W)three-dimensional(3D)samplingperfectionwithapplication-optimisedcontrastsusingdifferentflipangleevolutions;3D-MPRAGE:3DT1W magnetization-preparedrapid-acquisitiongradient-echosequence;TI:timeofinversion;NEX:numberofexcitations;FOV:fieldofview;PAT:parallelacquisitiontechnique; GRAPPA:generalizedauto-calibratingpartiallyparallelacquisitions;STIR:short-tauinversionrecoverysequence;SS-EPI:single-shotecho-planarimaging;RS-EPI: readout-segmentedecho-planarimaging.
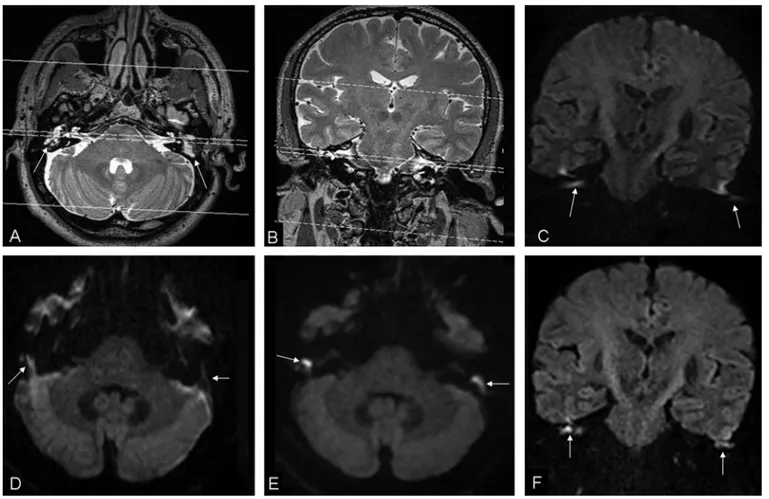
Fig.1. Reformattedaxial(A)andcoronal(B)3D-SPACEimagesofa48-yearoldmanshowsoft-tissueintherightandleftmiddleearcavities(arrowsinA).AllDWIimages wereobtainedtopassthroughtheinternalacousticcanalsasshownin3D-SPACEimages.BilateralclearhyperintensityoncoronalSS-EPI(C),axialSS-EPI(D),axialRS-EPI (E),andcoronalRS-EPI(F)imageswerecompatiblewithdiffusionrestrictionsecondarytoacholesteatoma.TheimagesachievedwithSS-EPItechniquehavemoreartefacts thantheimagesobtainedwithRS-EPItechnique(arrows).ThelesionontheleftsidecouldnotvisualizeclearlyonSS-EPIimages(arrows).
ears.Thelesionwashypointensein13 ears(57%),isointense in nineears(39%)andhyperintenseinoneear(4%)onSTIRimages.In theremainingninepatients,cholesterolgranuloma(1patient)and chronicotitismedia(8patients)werepresent.Themedian dimen-sionofthelesionsatthemiddleearcavitywas8mm(2–29mm).
There was a mild coherence between the presence of cholesteatomascoresofRS-EPIand SS-EPIimages(Table2).No correlationwasdetectedbetweenlesionvisibilityandpresenceof
Table2
Agreementvaluesbetweentheparameters.
ICC P-value RS-EPIvs.SS-EPI(artefactscores) – −0.086 0.060 EPIvs.SS-EPI(visibilityscores) – −0.064 0.278 RS-EPIvs.SS-EPI(coronalplaneADCvalues) 0.723 – <0.001 RS-EPIvs.SS-EPI(axialplaneADCvalues) 0.976 – <0.001 ICC:intra-classcorrelationcoefficient,:kappacoefficient.
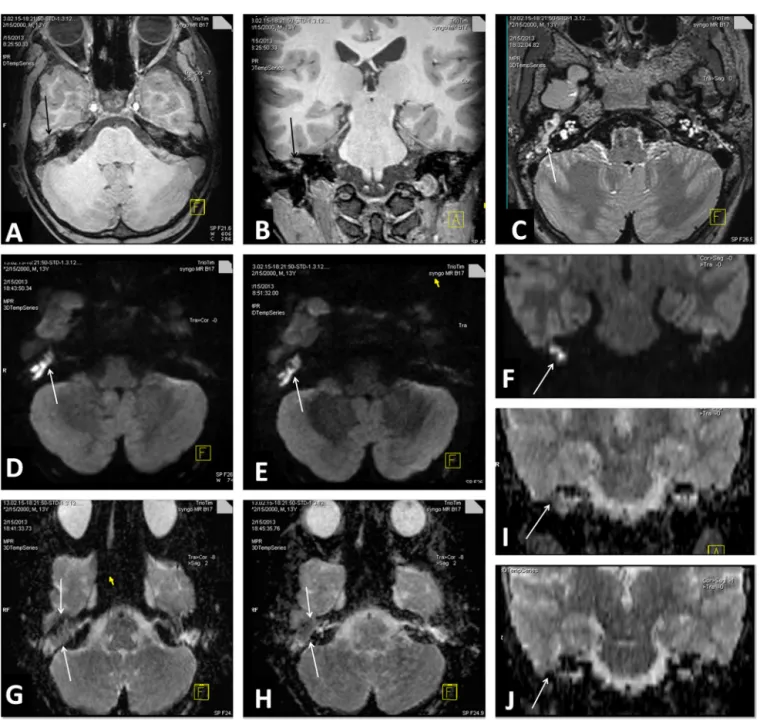
Fig.2.Reformattedaxial-coronalT2W3D-SPACE(A,B),andcoronalMPRAGE(C)imagesofa30-year-oldfemaleshowsoft-tissuethatfilledleftmiddleear(arrows).A hyperintenselesionrepresentingcholesteatomawiththesizeof6×7mmisseenonDWI(arrows,D-G).MoreartefactsexistonaxialandcoronalSS-EPIimages(D,G)when comparedwithaxialandcoronalRS-EPIimages(E,F).ItisalsodemonstratedthatthelesioncontourcanbevisualizedmoreclearlyonRS-EPIimages.Thelocalizationandthe relationwithadjacentstructuresofcholesteatomacanbeevaluatedbetteronaxial(T2W3D-SPACEplusDWI,H)andcoronal(MPRAGEplusDWI,I)fusedimages(arrows).
Table3
NumbersvisibilityandpresenceofartefactscoresofRS-EPIandSS-EPIgroups.
0 1 2 3 Na Total Visibilityscores RS-EPI – 1(2%) 17(28%) 25(42%) 17(28%) 60(100%) SS-EPI 1(2%) 18(30%) 24(40%) – 17(28%) 60(100%) Artefactscores RS-EPI 1(2%) 1(2%) 17(28%) 24(40%) 17(28%) 60(100%) SS-EPI 1(2%) 29(48%) 13(22%) – 17(28%) 60(100%)
Fig.3. MRimagesofcholesteatomaoftherightmiddleearina13-yearoldboy.Reformattedaxial-coronal3D-T1WMPRAGE(A,B)and3D-T2WSPACE(C)imagesshow soft-tissueintherightmiddleearcavity(arrows).AxialSS-EPI(D)andaxial-coronalRS-EPI(E,F)imagesobtainedwithabfactorof1000sec/mm2showmarkedlyhigh
signalintensityofthecholesteatoma(arrows).OnADCmapsfromSS-EPI(G,J)andRS-EPI(H,I)DWI,thecholesteatoma(arrows)ishypointensetocerebellumandbrain parenchyma.DelineationofcholesteatomaispooreronADCmapsobtainedfromSS-EPI(G,J).ADCvaluesofthecholesteatomaare407,417,380,and484m2/sonaxial
RS-EPI,coronalRS-EPI,axialSS-EPI,andcoronalSS-EPImaps,respectively.
artefactscoresofRS-EPIandSS-EPIgroups(P>0.05)(Table2). Arte-factscoresofRS-EPIimageswerelowerthanthoseofSS-EPIimages (Table3).Inaddition,thevisibilityscoresofthelesionsonRS-EPI imageswerehigherthanthoseonSS-EPIimages(Table3)(Fig.3). ThecomparisonbetweenGStestsandADCvaluesarepresented inTable4.ADCvaluesofGS=0(absenceofcholesteatoma)group wassignificantlyhigherwhencomparedwiththeADCvaluesof GS=1(presenceofcholesteatoma)group(P<0.05,Table4).
Thesensitivity,specificity,NPVand PPVvaluesof ADC mea-surementsobtainedwithRS-EPIandSS-EPItechniquesfordifferent cut-offvaluesaregiveninTable5.Areaundercurve(AUC)values wastendedtobehigherinaxialplanemeasurementsthanthosein coronalplanemeasurements(Table5).
DuringthestatisticalcomparisonofRS-EPIandSS-EPIwithGS testfindingsintermsofdetectingcholesteatoma,wenoticedthat theRS-EPItechniquewasmorecomparablewiththeGStestresults
(=0.74,P<0.001forRS-EPI;=0.5,P=0.001forSS-EPI)(Table6) (Fig.1).Usingthesurgicaloutcomeasthegoldstandard,the sen-sitivity,specificity,PPVandNPVofRS-EPIwerehigherthanSS-EPI (100%,78%,100%,and74%forRS-EPIversus91%,60%,88%,and67% forSS-EPI-DWI,respectively)(Table6).
Discussion
Cholesteatomaisabenigncondition,whichmayleadto seri-ouscomplicationsincludinghearingloss,labyrinthinefistulaand vestibulardysfunctionunlessitistreatedintime.Earlydiagnosis andtreatmentmayreducethecomplicationratesandprovidea betterprognosis.HRCTisthemostcommonlyusedtechniquefor scanningtemporalbone.AlthoughHRCTcanbeusefulforthe diag-nosisofthepatientswithoutmiddle-earsurgeryhistory,itisoften
Table4
Statisticalcomparisonsweredemonstratedbetweengoldstandard(GS)testresultsandADCvalues.ADCvaluesofalltechniquesweresignificantlydifferentincholesteatoma andnon-cholesteatomagroups.
GS=0(absenceofcholesteatoma) GS=1(presenceofcholesteatoma) P-value Median(min.–max.) Median(min.–max.)
RS-EPIADC(axial) 873(398–2200)m2/s 500(285–1178)m2/s 0.003
RS-EPIADC(coronal) 926(415–2200)m2/s 511(400–1281)m2/s 0.023
SS-EPIADC(axial) 960(491–2100)m2/s 500(285–1179)m2/s 0.001
SS-EPIADC(coronal) 920(600–1127)m2/s 503(320–1325)m2/s 0.003
Table5
Receiveroperatingcurve(ROC)analysisresultsofADCmeasurements.
AUC P-value Cut-offvalue Sensitivity Specificity PPV NPV RS-EPIADC(axial) 0.83 <0.001 ≤521 56.52 90.91 92.9 50 SS-EPIADC(axial) 0.86 <0.001 ≤500 56.52 90 92.9 47.4 SS-EPIADC(coronal) 0.83 <0.001 ≤503 52.38 100 100 50 RS-EPIADC(coronal) 0.81 <0.001 ≤511 52.17 90.91 92.3 47.6 RS-EPIADC(axial) 0.83 <0.001 ≤700 82.61 63.64 82.6 63.6 SS-EPIADC(axial) 0.85 <0.001 ≤705 86.96 60.00 83.3 66.7 SS-EPIADC(coronal) 0.83 <0.001 ≤706 71.43 60.00 78.9 50.0 RS-EPIADC(coronal) 0.81 <0.001 ≤700 73.91 63.64 81.0 53.8 AUC:areaundercurve;PPV:positivepredictivevalue;NPV:negativepredictivevalue.
insufficientforthediagnosisofsmallsizedcholesteatomalesions (especiallyinpatientswithmiddle-earsurgeryhistory)[14].
HRCT and DWI are usually combined for the diagnosis of cholesteatomaindailyroutinepractice.Althoughcholesteatomas showhighsignalintensity,granulation/fibroustissue,cholesterol granulomaandserousfluidshowlowsignalintensityonDWI[15]. Delayedphase gadoliniumenhanced T1Wimagingcanbeused forthediagnosisofcholesteatoma;howeverthereareconflicting dataaboutthismethodintheliterature.Althoughsomeauthors suggested that delayed phase post-contrast imaging is useful, othersindicatedthatdelayedphasepost-contrastimagingcould notprovideadditiveinformation[9,16].Theseconflictingresults werebelievedtoberelatedwiththedimensionofcholesteatoma
[16].Delayedphasepost-contrastT1Wimaging(45minutesafter intravenousgadoliniumadministration)hassomedisadvantages includingincreasedcost,thescanningtimeandriskofnephrogenic systemicfibrosis[14,17].Inaddition,somefalsepositive results couldbeseenatdelayedphasepost-contrastT1Wimagingsuch asretainedinflammatorysecretions,whichmaysimulatea non-enhancingcholesteatoma[18].
In cholesteatoma, patients’ geometric distortions and other artefactsareoftensevereonSS-EPIimagesoftemporalbone espe-ciallyat3TMRunits[19].Thelongdurationofreadoutand‘low bandwidthvalueperpixel in thephase-encodingdirection’are amongthereasonsof thiscondition[19].Althoughmany tech-niques(e.g.spin-echobasedsequencesorPROPELLERtechnique) wereexperimentedfordiminishingtheseartefacts,thereare sev-erallimitationsforeachtechniquesuchaslowresolutionorlong imagingtime[2,4–7,9,10].
RS-EPI-DWIisa noveltechniqueand notreportedfor imag-ingoftemporalboneintheliterature.Thebasicmethodologyfor Table6
Basedongold-standardtest findings;sensitivity,specificity,NPV, PPVvalues, overall-agreementandKstatisticresultsofRS-EPIandSS-EPItechniques.
RS-EPI SS-EPI Sensitivity(%) 100 91 Specificity(%) 78 60 NPV(%) 100 88 PPV(%) 74 67 Overallagreement(%) 87 75 Kvalue 0.74 0.50 P-value <0.001 <0.001
theRS-EPItechniquewasintroducedbyPorteretal.[8].Our pre-liminarystudyshowedthatRS-EPImethodcouldprovidehigher spatial-resolution and lesion-visibility with less distortion and artefactsthanSS-EPItechnique,whichisrelevantwithother stud-ies[19–21].Analysingthepresenceofcholesteatomascoresofour studyshowedthatRS-EPItechniquedifferssignificantlyfrom SS-EPItechniqueandcoulddetectcholesteatomainhighernumber ofpatients.Hence,RS-EPItechniquecansupplyamoreeffective evaluationforcholesteatomas.
AlthoughthesensitivityofSS-EPItechniqueisrelativelyhigh fordetectingthelesionsmorethan5mm,theeffectivenessofthis techniqueislowindetectinglesionsthatarelessthan5mm[18]. Wecouldnotvisualizethelesionclearlyandcouldnotmeasure ADCvalueincoronalplaneofSS-EPIinthreepatientsandinaxial planeofSS-EPIinonepatientamongourpatientgroup.Twooutof 4patientsthatmentionedabovewereoperatedforcholesteatoma previously.Themeanlesionsizewas7mm(range5–9.5)andthe lesionscouldbevisualised(clearlydepicted)andADC measure-mentscouldbeperformed,withRS-EPItechniqueinthosepatients. RS-EPImethodseemstobemoreusefulindetectionofsmalllesions and/orinevaluationofpostoperativepatients.
Accordingtotheliterature,theADCvaluesofcholesteatomas (700–1100m2/s)havebeenreportedtobeequalorlessthanthe brainparenchymawhilethosevaluesofabscess(400–570m2/s) have been reported to be significantly lower than the brain parenchyma[22,23].Howeverthereisnotareportedcut-offvalue relatedtoADCvaluesintheliterature.Similarly,acertaincut-off valuecouldnotbeindicatedinourstudyaswell.However,our findingsarecompatiblewiththeliteraturedata[3,16,18,22–24].
AnotherimportantoutcomeofourstudywasthatADC mea-surementsfromaxialimageshadbetterAUC,NPV,PPV,sensitivity andspecificityvalueswhencomparedwiththecoronalimageADC measurements.Thismaybeexplainedbythefactthatthecoronal planeDWIismoresensitivetothesusceptibilityartefacts.Thus, DWIimagesofmiddleearcavityshouldbeobtainedintheaxial plane.WethinkthatperformingT1andT2Wimagesinadditionto RS-EPIisnecessaryforaccuratedetectionoflocalization& exten-sionofthelesionsanddetection ofotherpathologicconditions oftheearsand/orcranium(such asfistulas,massesorabscess)
[14,17].Aswehaveexperiencedinourstudy,3Disotropic(voxel sizes<1mm)acquisitionofT1WandT2Wsequencesmightbe use-fulforevaluationofwholecraniumsimultaneously.Anoptimised androbustMRexaminationcanbeachievedonlyin15minutes
byaddingaxialRS-EPIDWIimagestosagittal3DT1WandT2W sequences(Table1).
Thepossibilityofmissingsmallsizecholesteatomadueto non-isotropic acquisition of DWI or relatively thick slices hasbeen reportedpreviously[14,24].Usually,muralcholesteatomasarenot visibleonDWI[18].Wedetectedrelativelyminimal susceptibil-ityrelateddistortion(especiallyoncoronalplaneimages)ofthe boneandairtransitionzoneinsomepatientsalthoughitwas sig-nificantlylessonRS-EPIimageswhencomparedwiththeSS-EPI technique.Mostlythoseartefactswerenotdetrimentalforthe diag-nosis.However,newandcomprehensivestudiesareneededforthe developmentofacompletelyartefact-freeDWItechnique.
Asalimitation,wedidnotcompareRS-EPI-DWIwitha non-EPIsequence,whichisoneofcurrentimagingtechniquesdueto timerestrictionoftheMRIacquisitions[25].Acomparisonbetween RS-EPI-DWIandanon-EPIsequencewouldbewelcome.Also,this studyonlyincludespatientswithaprediagnosisofcholesteatoma. Therefore,thisstudylackscriticalinformationofthepositive pre-dictivevalue of the test. Neither of thepatients withnegative testresultswhereoperated.Sinceclinicalandimagingfollow-up (range:1–5years)islessreliable.Thisfactorisariskofan under-estimationofthefalsenegativeresults.Finally,thereisastrong possibilityofincorporationbiasandreaderorderbias.Theseare difficulttoavoid.
Inconclusion,DWIwithRS-EPI,whichisarelatively artefact-freetechniqueandhasahigherresolutionthantheSS-EPImethod, providesamoreeffectiveassessmentforcholesteatomas.Also,the RS-EPItechniqueseemstobemoreefficientinthedetectionof smalllesionsand/orintheevaluationofpostoperativepatients. Disclosureofinterest
DAPisanemployeeandshareholderofSiemensAG.TwoUS patentshavebeenregisteredbyDAPforthediffusion-weighted readout-segmented EPI sequence used in this paper and are assignedtoSiemensAG.ThemethodisalsomarketedbySiemens AGasacommercialproductusingthename‘RESOLVE’.
Acknowledgement
WegratefullyacknowledgeDr.ElcinZanandDr.AliGüveyfor theirvaluablecontributions.
References
[1]AikeleP,Kittner T,OffergeldC, etal. Diffusion-weightedMR imagingof cholesteatomainpediatricandadultpatientswhohaveundergonemiddleear surgery.AJRAmJRoentgenol2003;181:261–5.
[2]IlicaAT,HidirY,Bulakbas¸iN,etal.HASTEdiffusion-weightedMRIforthe reli-abledetectionofcholesteatoma.DiagnIntervRadiol2012;18:153–8. [3]KhemaniS,SinghA,LingamRK,KalanA.Imagingofpostoperativemiddleear
cholesteatoma.ClinRadiol2011;66:760–7.
[4]AartsMC,RoversMM,vanderVeenEL,etal.Thediagnosticvalueof diffusion-weightedmagneticresonanceimagingindetectingaresidualcholesteatoma. OtolaryngolHeadNeckSurg2010;143:12–6.
[5]CimsitNC,CimsitC,BaysalB,etal.Diffusion-weightedMRimagingin post-operativefollow-up:reliabilityfordetectionofrecurrentcholesteatoma.EurJ Radiol2010;74:121–3.
[6]DeFoerB,VercruysseJP,PiletB,etal.Single-shot,turbospin-echo, diffusion-weighted imagingversusspin-echo-planar,diffusion-weightedimagingin thedetectionofacquiredmiddleearcholesteatoma.AJNRAmJNeuroradiol 2006;27:1480–2.
[7]Yamashita K, Yoshiura T, Hiwatashi A, et al. Detection of middle ear cholesteatoma by diffusion-weightedMR imaging:multishotecho-planar imagingcomparedwithsingle-shotecho-planarimaging.AJNRAmJ Neuro-radiol2011;32:1915–8.
[8]Porter DA, Heidemann RM. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensionalnavigator-basedreacquisition.MagnResonMed2009;62: 468–75.
[9]De FoerB, Vercruysse JP, Bernaerts A, etal. Middle ear cholesteatoma: non-echo-planardiffusion-weightedMRimagingversusdelayed gadolinium-enhanced T1-weighted MR imaging – value in detection. Radiology 2010;255:866–72.
[10]DremmenMH,HofmanPA,HofJR,StokroosRJ,PostmaAA.Thediagnostic accuracyofnon-echo-planardiffusion-weightedimaginginthedetectionof residualand/orrecurrentcholesteatomaofthetemporalbone.AJNRAmJ Neu-roradiol2012;33:439–44.
[11]Holdsworth SJ, Yeom K, Skare S, et al. Clinical application of readout-segmented-echo-planarimagingfordiffusion-weightedimaginginpediatric brain.AJNRAmJNeuroradiol2011;32:1274–9.
[12]BognerW,Pinker-DomenigK,BickelH,etal.Readout-segmentedecho-planar imagingimprovesthediagnosticperformanceofdiffusion-weightedMRbreast examinationsat3.0T.Radiology2012;263:64–76.
[13]NaganawaS,YamazakiM,KawaiH,etal.Anatomicaldetailsofthebrainstem andcranialnervesvisualizedbyhighresolutionreadout-segmentedmulti-shot echo-planardiffusion-weightedimagesusingunidirectionalMPGat3T.Magn ResonMedSci2011;10:269–75.
[14]VaidS,KambleY, VaidN,et al.Role ofmagnetic resonanceimagingin cholesteatoma:theIndianexperience.IndianJOtolaryngolHeadNeckSurg 2013;65:485–92.
[15]Dubrulle F,SouillardR, ChechinD,etal. Diffusion-weightedMRimaging sequenceinthedetectionofpostoperativerecurrentcholesteatoma.Radiology 2006;238:604–10.
[16]VenailF, BonafeA,PoirrierV,MondainM,Uziel A.Comparison of echo-planardiffusion-weightedimaginganddelayedpostcontrastT1-weightedMR imagingforthedetectionofresidualcholesteatoma.AJNRAmJNeuroradiol 2008;29:1363–8.
[17]DeFoerB,VercruysseJP,SpaepenM,etal.Diffusion-weightedmagnetic reso-nanceimagingofthetemporalbone.Neuroradiology2010;52:785–807. [18]Más-Estellés F, Mateos-Fernández M, Carrascosa-Bisquert B, et al.
Con-temporary non-echo-planar diffusion-weighted imaging of middle ear cholesteatomas.Radiographics2012;32:1197–213.
[19]MorelliJN,SaetteleMR,RangaswamyRA,etal.Echoplanardiffusion-weighted imaging:possibilitiesandconsiderationswith12-and32-channelheadcoils. JClinImagingSci2012;2:31.
[20]HoldsworthSJ,SkareS,NewbouldRD,etal.Readout-segmentedEPIforrapid highresolutiondiffusionimagingat3T.EurJRadiol2008;65:36–46. [21]Holdsworth SJ, Skare S, Newbould RD, Bammer R. Robust
GRAPPA-accelerateddiffusion-weightedreadout-segmented(RS)-EPI.MagnResonMed 2009;62:1629–40.
[22]ThiriatS,RiehmS,KremerS,MartinE,VeillonF.Apparentdiffusion coeffi-cientvaluesofmiddleearcholesteatomadifferfromabscessandcholesteatoma admixedinfection.AJNRAmJNeuroradiol2009;30:1123–6.
[23]KarandikarA,LokeSC,GohJ,YeoSB,TanTY.Evaluationofcholesteatoma:our experiencewithDWpropellerimaging.ActaRadiol2015;56:1108–12. [24]PennanéachA,GaretierM,OllivierM,OgnardJ,MarianowskiR,MeriotP.
Diag-nosticaccuracyofdiffusion-weightedMRimagingversusdelayedgadolinium enhancedT1-weightedimaginginmiddleearrecurrentcholesteatoma:a ret-rospectivestudyof39patients.JNeuroradiol2016;43:148–54.
[25]LincotJ,VeillonF,RiehmS,etal.Middleearcholesteatoma:compared diagnos-ticperformancesoftwoincrementalMRIprotocolsincludingnon-echoplanar diffusion-weightedimagingacquiredon3Tand1.5Tscanners.JNeuroradiol 2015;42:193–201.