CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports5(2014)500–504ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
jo u r n al ho me p a g e :w w w . c a s e r e p o r t s . c o m
An
unusual
stress
fracture:
Bilateral
posterior
longitudinal
stress
fracture
of
tibia
Melih
Malkoc
a,∗,
Ozgur
Korkmaz
a,
Tugrul
Ormeci
b,
Ismail
Oltulu
a,
Mehmet
Isyar
a,
Mahir
Mahirogulları
aaDepartmentofOrthopedicsandTraumatology,IstanbulMedipolUniversity,SchoolofMedicine,Turkey bDepartmentofRadiology,IstanbulMedipolUniversity,SchoolofMedicine,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received24April2014
Receivedinrevisedform2June2014 Accepted2June2014
Availableonline11June2014 Keywords:
Tibialstressfracture Longitudinaltibialfracture
a
b
s
t
r
a
c
t
INTRODUCTION:Stressfractures(SF)occurwhenhealthyboneissubjectedtocyclicloading,whichthe normalcarryingrangecapacityisexceeded.Usually,stressfracturesoccuratthemetatarsalbones, calcaneus,proximalordistaltibiaandtendstobeunilateral.
PRESENTATIONOFCASE:Thisarticlepresentsa58-year-oldmalepatientwithbilateralposterior longi-tudinaltibialstressfractures.A58yearsoldmalesufferingforpersistentleftcalfpainanddecreased walkingdistanceforlastonemonthandafterimagingstudiesposteriorlongitudinaltibialstressfracture wasdetectedonhislefttibia.Aftersixmonthsthepatientwasadmittedtoourclinicwiththesametype ofcomplaintsinhisrightleg.Allimagingmodalitiesandbloodcountswereperformedandasaresult longitudinalposteriortibialstressfracturesweredetectedonhisrighttibia.
DISCUSSION:Treatmentoftibialstressfractureincludesrestandmodifiedactivity,followedbyagraded returntoactivitycommensuratewithbonyhealing.Wehaveappliedthesametreatmentprotocoland ourresultswereacceptablebutourfollowuptimeshortforthisreasonourstudyisrestrictedforseparate stressfracturesoftheposteriortibia.
CONCLUSION:Althoughthemainlocalizationoftibialstressfractureswereunilateral,anteriorand trans-versepattern,rarely,likeinourcase,theunusualbilateralposteriorlocalizationandlongitudinalpattern canbeseen.
©2014TheAuthors.PublishedbyElsevierLtd.onbehalfofSurgicalAssociatesLtd.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/3.0/).
1. Introduction
Stress fractures (SF) occur when healthy bone is subjected to cyclic loading, which the normal carrying range capacity is exceeded.1,2SFmostlyseenathletesormilitaryrecruitsbecauseof
intensivephysicalexercise.2–4Usually,stressfracturesoccuratthe
metatarsalbones,calcaneus,proximalordistaltibiaandtendstobe unilateral.1,2Inthisstudy,weaimedtoreporta58-year-oldmale
patientwithbilateralposteriorlongitudinaltibialstressfractures.
2. Casepresentation
A58yearsoldmalesufferingforpersistentleftcalfpainand decreasedwalkingdistanceforlastonemonth.Hewas complain-ingtheprogressionofpainthroughonhisleftleg.Inhismedical historythere wasnochanges atthedailywalkingandexercise
∗ Correspondingauthorat:IstanbulMedipolUniversity,SchoolofMedicine, DepartmentofOrthopedicandTraumatology,TemAvrupaOtoyoluGoztepeCıkısi, No:1Bagcilar,34214Istanbul,Turkey.Tel.:+902124607777;fax:+902124607070.
E-mailaddress:[email protected](M.Malkoc).
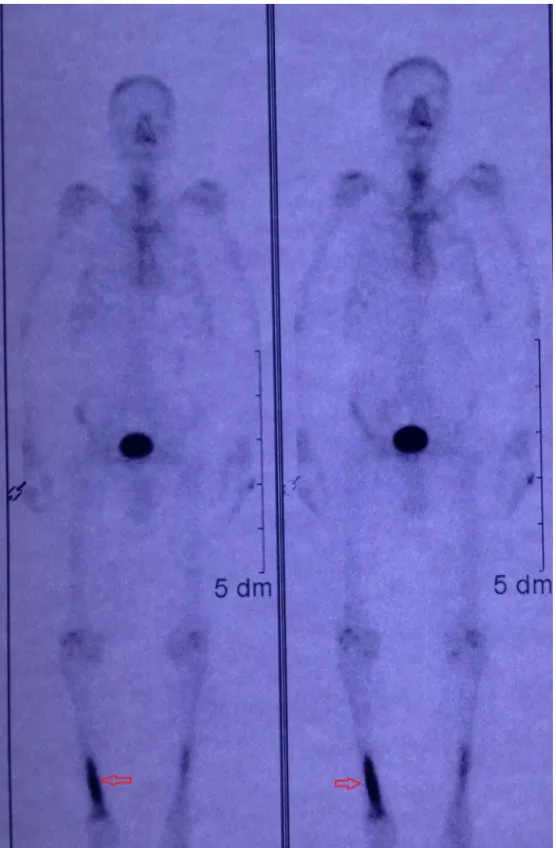
habits for last one year.Localization of theprogressive pain is mostly posterior of the wholeleg and culf. The pain he suffer was existing both with motionand rest. He was checked and hadatherapyforchronicosteomyelitisforthreemonthsandno recoveryhasbeenacquired.Thestandardlastinfectiontitleshave beenstudiedsuchassedimentationrates,C-reactiveprotein,ASO, rheumatoid factor,white blood cellvalue, redblood cellvalue. Allthevaluesofthetestswerenormal.X-ray(Fig.1)and mag-neticresonanceimaging(MRI)(Figs.4and5)havebeenobtained andthree-phasedbonescintigraphywasstudied(Fig.6).Especially withMRIandbonescintigraphyposteriorlongitudinaltibialstress fracturewasdetectedonhislefttibia.Thepatientwasinstructedto restrictactivitytononweight-bearingexerciseforfourtosixweeks, followedbyaperiodofgradualincreaseinweight-bearing activ-ityandanti-inflammatorytreatmentapplied.Aftersixmonthsthe patientwasadmittedtoourclinicwiththesametypeofcomplaints in his rightleg. Allimaging modalities and blood counts were performedandasaresultlongitudinalposteriortibialstress frac-turesweredetectedonhisrighttibia(Figs.2,3and7)Thepatient wasinstructedtorestrictactivitytononweight-bearingexercise forfourtosixweeks,followedbyaperiodofgradualincreasein weight-bearingactivityandanti-inflammatorytreatmentapplied http://dx.doi.org/10.1016/j.ijscr.2014.06.002
2210-2612/© 2014TheAuthors.Published byElsevier Ltd.onbehalf of SurgicalAssociatesLtd. Thisis an openaccessarticle underthe CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
Fig.1. Bilateralantero-posteriorX-raygraphyoftibias.
again.Attheendofsixweeks,patienthadpainlessandfree move-mentofthebothlowerextremity.14monthsoffollow-upperiod, patientgainedthepainfreeweight-bearingandfulloflegmotion. 3. Discussion
Sportsinjurieshavesignificantlyincreasedinfrequencyinthe pastfewyears,especiallyamongindividualswhoselevelofphysical fitnessisillsuitedtotheintensityortheverynatureofthe activ-ityundertaken.Althoughdataontheprevalenceofsportsinjuries seemtobedifficulttocollect,itisestimatedthatapproximately 6%ofthosewhoengageinsportsrequiremedicalcarefortheir injuries.5,6Themostcommonlocationsforstressfracturesarein
Fig.2.TransverseMRIsectionofrighttibia.
Fig.3.CoronalMRIsectionofrighttibia.
CASE
REPORT
–
OPEN
ACCESS
502 M.Malkocetal./InternationalJournalofSurgeryCaseReports5(2014)500–504
Fig.5. CoronalMRIsectionoflefttibia.
thetibia(23.6%),tarsalnavicular(17.6%),metatarsal(16.2%),fibula (15.5%), femur(6.6%), pelvis(1.6%), and spine (0.6%).7,8 A bone
scanisasensitivemethodforearlydiagnosisofafatiguefracture. Theradioactivetracerisincorporatedintothecellsresponsiblefor boneremodellingwithin24hfollowingthefracture.However,this techniqueisnotsufficientlyspecificbecauseboneturnovercanbe increasedinawidevarietyofothersconditionsincludingtumours, infectionsorinflammations.8–10At3-DCT-scan,thebonerepair
reactionappearsasbonysclerosissurroundingthelineoffracture. Insomestudies,thistechniqueisevenmoresensitiveandspecific
thanMRI.11,12Duetoitsmutiplanarcapabilitiesandhightissue
contrast,MRIistheimagingmodalityofchoicefordiagnosingan SF.MRIissensitiveandspecific,revealingintramedullaryoedema, theperiostealreactionandthefractureline.
Khyetal.reporteda35yearsoldpatientpresentingwithpain inthemedialaspectofbothknees.Ultrasonography(USG) appear-ance and with clinicalfindings together,suggested a diagnosis ofsimultaneousbilateralfatiguefracture.AnMRIconfirmedthe diagnosisand thepatient’s symptoms resolvedwith rest.They reportedUSGmaybeausefulimagingtoolinthediagnosisofstress fracture.13InourcasewedidnotperformedUSGtoourpatient.
Kilcoyneetal.wererandomizedthepatientswithtibialstress frac-tures topulsedultrasound orplacebo treatment.Theresultsof placeboversuspulsedultrasoundwerenodifferentwithrespectto healingtimeandreturntoduty.14Inourcase,restrictionof
weight-bearingandanti-inflammatorymedicationwerelimitedthepain andincreasedtherangeofmotion.Liimatainenetal.treated sur-gically49anteriormid-tibialstressfracturesin45patientsduring theyears1985–2005.Allthepatientswereathletes,mainly run-ners.Themeanageofthepatientswas26years.34ofthefractures occurredinmenand15inwomen.Thefirstmethodoftreatment, anteromedialandlateraldrilling,wasusedin20operationsand thesecondmethod,laminofixation,in29operations.Surgical treat-mentwithlaminofixationprovedtobesuperiortotibialfracture sitedrilling.15Wetreatedourcasewithoutsurgeryandallthetibial
stressfracturesaremidtibialinLiimatainenetal.studybutinour casethetibialstressfracturesarebilaterallyandintheposterior
Fig.7.Bonescanofrighttibia.
longitudinalformation.AccordingtovanderVelde’sstudythree patientssufferedfromexercise-relatedlowerlegpain,clinical fea-tures,andriskfactorsspecificforposteriortibialstressfracture. Diagnosiswasconfirmedforallthreeindividualsbyradiographic imaging.Treatmentincludedrestandmodifiedactivity,followed byagradedreturntoactivitycommensuratewithbonyhealing. Thisapproachwassuccessfulfortwooftheindividualsdiagnosed withposteriortibialstressfracture.Inthethirdindividual treat-mentrecommendationswerenot adheredto,resultingin three
separatestressfracturesoftheposteriortibiaover27months.16
Wehaveappliedthesametreatmentprotocolandourresultswere acceptablebutourfollowuptimeshortforthisreasonourstudyis restrictedforseparatestressfracturesoftheposteriortibia.
4. Conclusion
Althoughthemainlocalizationoftibialstressfractureswas uni-lateral,anteriorandtransversepattern,rarely,likeinourcase,the
CASE
REPORT
–
OPEN
ACCESS
504 M.Malkocetal./InternationalJournalofSurgeryCaseReports5(2014)500–504
unusualbilateralposteriorlocalization and longitudinalpattern canbeseen.Themajorityoftibialstressfracturesareeffectively managewithanappropriatebalanceofrelativerestandtherapy withoutanysurgery.
Conflictofinterest None.
Funding None.
Ethicalapproval
Writteninformedconsentwasobtainedfromthepatientfor publicationofthiscasereportandaccompanyingimages. Authorcontributions
MelihMalkoc:studydesign;TugrulOrmeci:datacollectionand figurepreparation;Ozgur Korkmaz:writing;IsmailOltulu:data collection; Mehmet Isyar: datacollection; Mahir Mahirogulları: analysis.
Keylearningpoint
• Unusualandbilateralplacementoftibialstressfracture.
References
1.MathesonGO,ClementDB,McKenzieDC,TauntonJE,Lloyd-SmithDR, Mac-IntyreJG.Stressfracturesinathletes.Astudyof320cases.AmJSportsMed 1987;15:46–58.
2.HulkkoA[Dissertation]Stressfracturesinathletes.Aclinicalstudyof368cases. Finland:ActaUnivOuluensis,SeriesD:Medica169,UniversityofOulu;1988.
3.DevasMB:.Stressfractureofthetibiainathletesor“shinsoreness”.JBoneJoint Surg1958;40B:227–39.
4.HallelT,amitS,SegalD.Fatiguefracturesoftibialandfemoralshaftinsoldiers. ClinOrthop1976;118:35–43.
5.DreinhöferKE,ReichelH,KäferW.Strategiesforpreventionandmanagement ofmusculoskeletalconditions.Lowerlimbpain.BestPractResClinRheumatol 2007;21:135e52.
6.PerisP.Stressfractures.BestPractResClinRheumatol2003;17(6):61–1043.
7.BruknerP,BradshawC,KhanKM,WhiteS,CrossleyK.Stressfractures:areview of180cases.ClinJSportMed1996;6(2):85–9.
8.MathesonGO,ClementDB,McKenzieDC,TauntonJE,Lloyd-SmithDR, Mac-IntyreJG.Stressfracturesinathletes.Astudyof320cases.AmJSportsMed 1987;15(1):46–58.
9.SofkaC.Imagingofstressfractures.ClinSportsMed2006;25:53e62.
10.SoubrierM,DubostJJ,BoisgardS,SauvezieB,GaillardP,MichelJ,etal. Insuffi-ciencyfracture.Asurveyof60casesandreviewoftheliterature.JointBoneSpine 2003;70:209e18.
11.GaetaM,MinutoliF,ScribanoE,AscentiG,VinciS,BruschettaD,etal.CTandMR imagingfindingsinathleteswithearlytibialstressinjuries:comparisonwith bone.Scintigraphyfindingsandemphasisoncorticalabnormalities.Radiology 2005;235:553e61.
12.GaniyusufogluAK,OnatL,KaratoprakO,EnercanM,HamzaogluA.Diagnostic accuracyofmagneticresonanceimagingversuscomputedtomographyinstress fracturesofthelumbarspine.ClinRadiol2010;65:902e7.
13.KhyV,WyssaB,BianchiS.Bilateralstressfractureofthetibiadiagnosedby ultrasound.Acasereport.JUltrasound2012;15:130e134.
14.KilcoyneKG,DickensJF,RueJP.Tibialstressfracturesinanactiveduty popula-tion:long-termoutcomes.JSurgOrthopAdv2013;22(1):50–3.
15.LiimatainenE,SarimoJ,HulkkoA,RanneJ,HeikkiläJS.Oravaanterior mid-tibialstressfractures.Resultsofsurgicaltreatment.ScandJSurg2009;98: 244–9.
16.GabrielleM,vanderVeldeDC,WilliamS,HsuDC.Posteriortibialstressfracture: areportofthreecases.JManipulativePhysiolTher1999;22(June(5)):341–6.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.