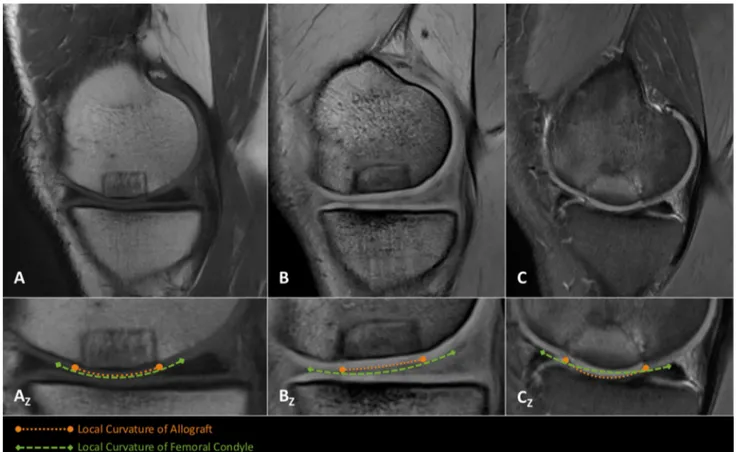
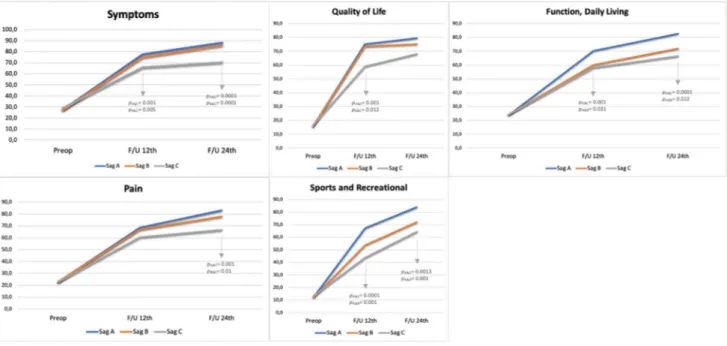
Local curvature mismatch may worsen the midterm functional outcomes of osteochondral allograft transplantation.
Tam metin
Şekil
Benzer Belgeler
Erlich ve Davis otopsi ~ah:;;maslile 20 serebral gli- oblastomah olgurmn 5'inde spinal leptomeningeal me- tastaz gosterdiler (5).Yung 53 serebral glioblastomah olgunun 9'unda
Aşağıdaki sözcüklerden hangisinin Aşağıdaki sözcüklerden hangisinin ünlü harf sayısı, ünsüz harf sayı- ünlü harf sayısı, ünsüz harf sayı- sından fazladır?.
(2011), they conducted a survey in Pamukkale university Turkey, to examine the level of hopelessness and related factors among medical students and residents,
The study addresses six main issues: what methods teachers use to correct the written work of the students, how often teachers provide students with feedback about their written
The phenolic acid is either gallic acid, in the case of gallotannins, or else hexahydroxydiphenic acid (=HHDP) and its oxidized derivatives(dehydrohexahydroxydiphenic acid
THE MEASUREMENT OF THE PERCEIVED SERVICE QUALITY IN THE LOCAL TOURS CRITICAL INCIDENTS TECHNIQUE (CIT).. Şule
In 1845, he began building a small house on Emerson's land on the shore of Walden Pond, where he spent more than two years "living deep and sucking out all the marrow of
Demographic and clinical data such as age, gender, vascular risk factors, antithrombotic or anticoagulant use, presence of symptomatic cSAH or intracerebral
