Original
article
Video
game-based
therapy
for
the
non-dominant
hand
improves
manual
skills
and
grip
strength
Effets
de
la
the´rapie
base´e
sur
les
jeux
vide´o
pour
la
main
non
dominante
sur
les
compe´tences
manuelles
et
la
force
de
pre´hension
H.
Bostanci
a,*
,
A.
Emir
a,
D.
Tarakci
a,
E.
Tarakci
baDivisionofErgotherapy,FacultyofHealthSciences,IstanbulMedipolUniversity,Kavacik,EkincilerCd.No:19,34810Istanbul,Beykoz,Turkey bDivisionofPhysiotherapyandRehabilitation,FacultyofHealthSciences,IstanbulUniversity-Cerrahpasa,Zuhuratbaba,DoktorTevfikSag˘lamCd.No.25,
34147Istanbul,Bakirko¨y,Turkey
ARTICLE INFO
Articlehistory:
Received2December2019
Receivedinrevisedform13February2020 Accepted20February2020
Availableonline2April2020 Keywords: Manualskills Non-dominanthand Virtualreality Upperextremity Occupationaltherapy Motscle´s: Compe´tencesmanuelles Mainnondominante Re´alite´ virtuelle Extre´mite´ supe´rieure Ergothe´rapie
SUMMARY
Thestudywasdesignedtoinvestigatetheeffectofvirtualreality-supportedtrainingonmanualskills and grip strength in the non-dominant hand in healthy participants. Thirty participants were randomizedintotwogroups:ErgoActivegroup(n=15)andcontrolgroup(n=15).TheErgoActivestudy groupreceived8weeksoftrainingwithleapmotioncontroller-basedvirtualrealitygames.Thetraining wasdone1dayperweekfor30min.Theparticipants’handfunctionwasevaluatedusingtheJebsen TaylorHandFunctionTest(JTHFT),whilegripstrengthwasevaluatedwithaJamarHandDynamometer andPinchmeter.After8weeks,theErgoActiveandcontrolgroupshadsignificantlydifferentJTHFT, JamarandPinchmeterresults(P<0.05).Whenleapmotioncontroller-basedvirtualrealityapplications areused,healthysubjectshaveincreasedmanualskillsandgripstrengthintheirnon-dominanthand. Thesevirtualrealitygamesareaneffectiveandfunwayofimprovingpatients’handfunctions.
C 2020SFCM.PublishedbyElsevierMassonSAS.Allrightsreserved.
RE´ SUME´
L’e´tudee´taitconc¸uepoure´tudierl’effetdesformationsbase´essurlare´alite´ virtuellesurlescompe´tences manuellesetlaforcedepre´hensiondanslede´veloppementdefonctionsdelamainnondominantechez desparticipantsenbonnesante´.Trenteparticipantsonte´te´ randomise´sendeux groupes:groupe d’entraıˆnementetgroupete´moin.L’e´tudeae´te´ re´alise´eavecdesjeuxdere´alite´ virtuellebase´ssurLMCet legroupete´moinae´te´ e´value´ a` desintervallesdehuitsemaines.Legroupedeformationae´te´ entraıˆne´ un jourparsemainependanthuitsemainesetlesse´ancesduraient30min.Lesfonctionsdesmainsdes individusonte´te´ e´value´esparletestdefonctiondelamainJebsenTaylor(JTHFT),laforcedepoigneavec ledynamome`treet laforcede pinceaveclepinchme`tre Jamar.Apre`s laformation, ilyavaitune diffe´rencesignificativedanslesre´sultatssurlesJTHFT,JamaretPinchmeterentrelegroupeentraıˆne´ etle groupecontroˆle(p<0,05).Enconse´quence,lesapplicationsdere´alite´ virtuellebase´essurLMCutilise´es pourame´liorerlesfonctionsdesmainsavaientaugmente´ ladexte´rite´ manuelleetlaforcedepre´hension desmainsnondominantesdesujetssains.Lesjeuxdere´alite´ virtuellebase´ssurLMCpeuventeˆtre conside´re´scommeunmoyenefficaceetamusantd’ame´liorerlesfonctionsmanuellesdupatient.
C 2020SFCM.Publie´ parElsevierMassonSAS.Tousdroitsre´serve´s.
* Correspondingauthor.
E-mailaddress:[email protected](H.Bostanci).
Available
online
at
ScienceDirect
www.sciencedirect.com
https://doi.org/10.1016/j.hansur.2020.02.011
Introduction
Virtual reality (VR) canbedefined asa computer-generated environment,realorimaginary,thatisexperiencedand manipu-latedthroughamulti-sensorycomputerinterface[1].VRsystems offerbenefitssuch asinstant feedback, stimulus-basedcontrol, stimulus adjustment from simpler to more complex, easy recordingofindividuals’progressandasafelearningenvironment. Anotherimportantfeatureisonlinefeedback,whichcanimprove theeffectiveness of learning-based educationby detecting and correctingmotorerrors[2].Themostimportantcharacteristicof VRforrehabilitationisitsabilitytoaddressmultiplekeyfeatures for a variety of different client populations. One of these key features,especiallyforoccupationaltherapy,ispersonalizedand customizedinterventions[3].
Thevirtualimageoftheupperextremitiescanbecreatedona computerscreenwhereindividualswillhavetomakemovements accordingtotheirintendedactivities.Thesemethods,whichare alsousedtoimprovehandandupperextremityfunction,arecalled VR-supportedrehabilitation.
Overuse,injuryandgeriatriccomplicationscanallcontributeto handdysfunction,total orpartial,whichdirectly diminishesthe qualityoflife.Insomecases,itrequireslong-termtherapytofully restorethe hand’s function, which is sometimes a very intense processforpatients.VRgameshavebeen showntobeusefulin improvingupperlimbfunctionandactivitiesofdailylifewhenused asanadjuncttonormaldailytreatment[4].ACochrane review concludedthatVRwasaneffectivetreatmentforrecoveryofupper extremitymotorfunctionandactivitiesofdailylivingafterstroke, when compared to conventional rehabilitation therapy [5]. To achieveupperextremityrehabilitationgoals,variousvideogames havebeen createdtofulfillthe differentobjectivesproposedby healthprofessionals. Video game-basedrehabilitation integrates individuals’dailylifeactivitiesandmotivatedindividualsbeginto usethesegamingexperiencesintheirdailylives.
VRsystemsaredevelopedbasedonsensortechnologies.Many sensorscanbeusedforVRsystems.Themostpopularoftheseare NintendoWiiTMandMicrosoftKinectTM.However,thesedevices focusonallbodyfunctionsandareinadequatetodetectfinehand skills [6]. The leap motion controller (LMC) is a commercially availabledevicethatisalow-cost,low-flexibility,optoelectronic system embedded in a semi-immersive VR system capable of trackinghandmovements[7].Itcanbeusedtoimproveone’shand functionasitcanbeeasilychangedbasedontheperson’sneeds.It isperceivedasentertainingandmotivatingand providesmotor learning.
Considering this information, the aim of this study was to investigate the effect of VR games on manual skills and grip strengthinthenon-dominanthand.Thefirstgoalwastoincrease ourunderstandingoftheavailabilityofVRrehabilitationgamesfor healthyindividuals.Thesecondgoalwastoevaluatetheusability ofgamesdevelopedforgripskillsinrehabilitationandtoobtain preliminarydata for expectations and preferences about video game-based training in hand rehabilitation. This study was initiatedbecauseVRiseasytoapply,providesreal-timeevaluation duringplayandprovidesfeedbackinhandrehabilitationthatisnot possiblewithconventionaltreatments.
Materialandmethods Participants
Participants were recruited between April 2016 and July 2017 to participate in this study at Medipol University. All participantssignedinformedconsentforms.Ethicalapprovalfor
thisstudywasobtainedfromtheResearchEthicsCommitteeof IstanbulMedipol University(No.: 108400987-275).Thisproject was supported by the Scientific and Technological Research CouncilofTurkey(projectnumber:1919B011800515).
Inclusioncriteriaconsistedofbeingagedbetween18–24and being able to use both upper extremities. Participants were excludedfromthestudyiftheyhadahistoryofupperextremity surgery or neurological and orthopedic problems affecting the upper extremity’s function. Participant demographics are pre-sentedinTable1.
Studydesign
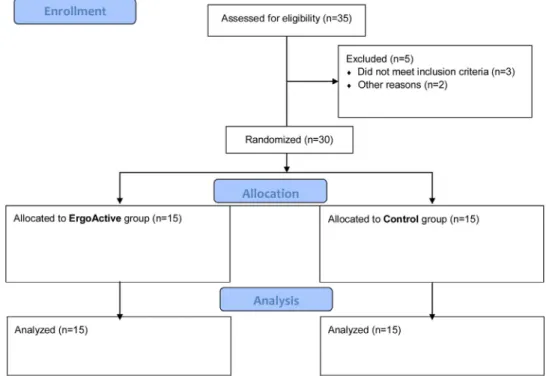
Thisstudywasconductedasa randomizedcontrolled study, withrandomizationperformedbycomputerprogram.Participants wererandomizedintotwogroups:ErgoActivegroup(n=15)who received 8 weeks of non-dominant hand training based on VR gamesdesignedbytheresearchteam,usingtheLMCsystem,anda controlgroup(n=15)whoreceivednotraining,onlyevaluations. AflowdiagramofthestudydesignispresentedinFig.1. Outcomes
Theparticipants’ non-dominanthand wasassessedwiththe JebsenTaylor HandFunctionTest(JTHFT)while gripand pinch strength were assessed with pinchmeter and Jamar hand dynamometer. All measurements were performed at baseline andafter8weeks.
JebsenTaylorHandFunctionTest(JTHFT)
Manualskillswerethemainoutcome.TheJTHFTwasusedto evaluatethebroadaspectsofhandfunctioncommonlyperformed in dailyactivitiesand toprovidequantitativemeasurements of standard activities [8]. JTHFTconsists of seventimed subtests: writing,cardturning,pickingupsmallcommonobjects,simulated feeding,stackingcheckers,movinglightobjectsandmovingheavy objects[9].Thetime tocompleteeach subtestwasrecordedin seconds.Thetimeforeachsubtestwasdeterminedalongwiththe totaltimetocompletealltasks.
Jamar1
handdynamometer
Handgrip strength was evaluated with a Jamar1 hand dynamometer,whichmeasuresisometricmusclecontractionfor dominantandnon-dominanthands.Measurementsweremadeas recommendedbytheAmericanSocietyforHandTherapists,with theparticipantseated,shoulderinadduction,elbowflexedat908, forearminneutralposition[10].
Pinchmeter
Apinchmeterwasusedtomeasure fingergripstrength.Three typesofgripswereevaluatedwithapinchmeterinthenon-dominant hand:fingertipgripstrengthwiththeendportionsofthe1stand2nd
Table1
Demographicfeaturesoftheparticipants. Demographicfeatures ErgoActivegroup
n=15 Controlgroup n=15 P Sex,n(%) 0.550 Female 13(86.7) 1(6.7) Female 2(13.3) 14(93.3) Age(years) 19.86(1.45) 19.73(1.16) 0.310 Mean(SD) 0.148 Dominantside,n(%) Right 11(73.3) 14(93.3) Left 4(26.7) 1(6.7) SD:standarddeviation
fingers,keygripstrengthwiththetipofthe1stfingerandthelateral aspectofthe2ndfinger,triplegripstrengthwiththetipportionsof the1st,2ndand3rdfingers.Thetestwasrepeatedthreetimes.The averagevalueinthesethreegriptypeswasrecordedasakilogram force[11].
Intervention
ThetrainingprogramfortheErgoActivegroupconsistedof one30-minutesessiononceaweekfor8weekswiththe non-dominant hand. Researchers developed two rehabilitation
games:‘‘Masterchef’’and‘‘Hold-and-Put’’usingLMCaspartof aresearchproject(Fig.2).Thegamesweredevelopedonasingle platform called ErgoActive. The aim of these games was to develop manualskills andfinemotor skills(supportedby the Scientific and Technological Research Council of Turkey with project number: 1919B011800515). Manual skills are trained duringthesegames,whichincludemanytypesofgrip,suchas light circumferential flexion grip and standard grip. The participants trainedon thesegamesduring each session.The way to play the games and the performance criteria were explainedindetailtotheparticipants.
Fig.1.Flowdiagramsummarizingthestudydesign.
Statisticalanalysis
TheSPSSstatisticalpackage(version21;SPSSInc,Chicago,IL) wasusedfordataanalysis.Thedatanormalitywasdetermined usingthe Shapiro-Wilkstest (P<0.05).The Wilcoxontest was usedtocomparethescorechangebetween baselineandthe 8-weekvisit in bothgroups. TheMannWhitneyU testwasused comparetheoutcomesbetweenthegroupsafter8weeks. Results
The ErgoActive grouphad significantly betterresultson the JTHFTtasksofwriting,cardturning,lightobjectliftingandheavy object lifting after 8 weeks of VR training than at baseline (P<0.05).TheErgoActivegroupwasfasterinthewriting,moving lightobjectsandmovingheavyobjectstasksafterVRtrainingthan thecontrolgroup(P<0.05).Whenthechangesintotalscorewere examined,therewasasignificantdifferencebetweengroupsafter 8weeks (P<0.005). JTHFTscoresbefore and aftertraining are presentedinTable2.
Handgrip strength was significant better in the ErgoActive groupafter their8 weeksof training(P<0.05).The ErgoActive groupalsohadstatisticallybettergripstrengthafterVRtraining thanthecontrolgroup(P<0.01).
AfterVRtraining,thetipgripandtriplegripwerestatistically improvedintheErgoActivegroup(P<0.05).Thetipgripandtriple gripevaluationsweresignificantlybetterintheErgoActivegroup than the control group (P<0.05). However, there was no significantdifferencebetween groupsinthekeygrip(P>0.05). Gripstrengthscoresbeforeandaftertrainingwerepresentedin
Table3.
Discussion
The aim of this study was to determine whether training performed on VR games would beeffective at improving non-dominanthandskillsandgripstrengthinhealthyindividuals.In
particular,thefirstobjectivewastoprovetheeffectivenessofVR gamesonhandfunctioninhealthyindividualsandtoincreaseour understanding of theusabilityof this type of training toguide future clinical use. The second objective was to evaluate the usabilityofgamesdevelopedforgripskillsinrehabilitationandto obtainpreliminarydataforexpectationsandpreferencesaboutVR gamesinhandrehabilitation.
Chiu et al. compared groups at 6 weeks and 12 weeks to determinetheshort-andlong-termeffectsofVRgamesonhand function.Nosignificantdifferencewasfoundbetweengroupsafter 6weeksand12weeks[12].Hence,the8-weektrainingperiodin ourstudyisconsistentwiththistimeframe.
Tarakcietal.conductedarandomizedcontrolledtrialevaluating theeffectivenessofthe8-weekLMC-basedtherapy(LMCBT)upper extremityrehabilitationprogram,comparingconventional rehabil-itationtoVR-basedtraininginchildrenwithphysicaldisabilities. Theyfoundsignificantimprovementinupperextremityfunctions in all LMCBT and conventional rehabilitation groups [13]. The methodsandsensorsusedinourstudyweresimilartothatstudy. Also, games aimed at manual skills used in the two training methods are similar. In both studies, JTHFT was found to be significantlyfasterthanthetotaltimeatbaselinefortheErgoActive group,andindividualswereabletocompleteactivitiesinlesstime. Gonzalezetal.designedarandomizedcontrolledtrialinvolving 23Parkinson’spatientsthatcomparedLMC-basedVRtrainingwith conventionaltherapy.Whiletherewerenoimprovementsingrip strength,significantimprovementsinfunctionalabilitieswiththe BoxandBlocksTestandthePurduePegboardTestwereobserved afterVRtraining[14].Thesefindingsandourssuggestthat LMC-basedVRtraininghasapositiveeffectonhandgripstrength.
Luna-Olivaetal.conductedastudyofhemiplegicanddiplegic cerebralpalsypatientsbetweentheagesof4and11whowere giventwo30-minuteVRsessionsperweekfor8weeks.Intheir studyusingtheXboxOneKinect,JTHFTdecreasedinallsubtests exceptformovingheavyobjects[15].Consideringthissignificant difference,thepositivechangeinJTHFTsupportsusingLMC-based VRgamestoimprovemanualskills.
Table2
JTHFTscoresbeforeandafterVRtraining. ErgoActivegroup n=15
Controlgroup n=15
Pb
Before After Pa Before After Pa
JTHFT,total 74.99(12.68) 61.93(7.59) 0.001 67.44(9.0) 65.87(7.91) 0.733 0.003 Writing 31.69(8.92) 24.17(6.36) 0.002 28.87(7.89) 27.41(6.65) 0.427 0.012 SPT 5.71(1.34) 4.70(0.72) 0.017 4.81(0.85) 4.99(0.92) 0.348 0.17 PO 8.20(1.57) 8.06(1.03) 0.733 7.39(1.12) 8.0(1.51) 0.173 0.254 SF 15.92(5.76) 14.27(2.91) 0.496 15.22(2.62) 14.38(1.94) 0.281 0.983 SC 3.72(1.10) 3.29(1.32) 0.222 3.09(0.56) 3.02(0.65) 0.394 0.372 MLO 4.93(0.73) 3.745(0.46) 0.001 4.01(0.43) 3.98(1.0) 0.427 0.001 MHO 4.80(0.61) 3.66(0.490) 0.001 4.06(0.43) 4.05(0.42) 0.426 0.000 JTHFT:JebsenTaylorHandFunctionTesttotalscore;SPT:simulatedpageturning;PO:pickingupsmallcommonobjects;SF:simulatedfeeding;SC:stackingcheckers;MLO: movinglightobjects;MHO:movingheavyobjects.
a
Intragroupcomparison(Wilcoxontest).
b
Intergroupcomparison(MannWhitneyUtest).
Table3
GripstrengthbeforeandafterVRtraining.
ErgoActivegroup Controlgroup Pb
Before After Pa Before After Pa Handgrip 24.60(6.38) 28.26(7.36) 0.001 20.26(6.54) 20.93(6.49) 0.025 0.001 Tipgrip 2.26(0.72) 3.13(1.17) 0.001 2.76(0.65) 2.63(0.78) 0.339 0.000 Keygrip 5.10(1.32) 5.70(1.29) 0.10 4.86(0.97) 5.23(0.82) 0.19 0.451 Triplegrip 3.73(1.26) 4.56(1.38) 0.003 3.66(0.83) 3.40(0.82) 0.33 0.000 a
Intragroupcomparison(Wilcoxontest).
b
Studieshave reported a relatively highaccuracy of LMC for determining finger and hand positions and movements
[16].Thankstothis sensitivity,participantsreported thatfinger and hand movements could be transferred into daily living activitiesthatrequiredifferenttypesofgrip.
Itishighlyrestrictivetopurchasevariousmaterialsneededfor theseVRenvironmentsinclinicalsettings.However,anLMC-based VRsystemiscost-effectiveandportable.Italsooffersindividualsan environmentwherethey canperformsafeactivitiesduringtheir training sessions. It is important that participants who are successful in VRactivities cantransfer these performances toa realenvironmentsuchashome.Goodoccupationaltherapytraining canbeachievedbytransferringthelearnedactivitiestodailylife. It is assumed that the VR-based training protocol on the RehabilitationGamingSystem(RGS)createsconditionsthathelp recoverythroughthehumanmirrorneuronsystem.IntheirRGS study,Prochnowetal.soughttotestthishypothesisbyidentifying theareasofthebraininvolved incontrollingthecaptureofthe approaching colored balls in the virtual RGS environment. In agreementwiththeirworkinghypothesis,thesefindingsshowed theengagementofbrainareasbelievedtorepresentthehuman mirrorneuronsystem[17].
Intheirstudy,Moseleyetal.soughttotestwhetherthemirrors fortreatingpaincanbeusedtoinduceincreasedneckorother spinemovements,andwhetherthisillusioncanbeachievedusing VR.TheyshowedthatVRcouldproducemovementssimilartothe bodyillusionunderlyingmirrortherapyforimaginarylimbpain andchronicpain.Thestatisticalsignificancealsoconfirmedthis
[18].In ourstudy,wesuggest thattheseperceivedmovements couldbeusedinhandrehabilitation.
We observed good motivation, which is one of the biggest advantages of the VR system used, as evidenced by the high percentageofadhesiontothetraining.Oneparticipantstatedthat aftershestartedtheVR-supportedpractice,shefrequentlyused hernon-dominanthandwhileapplyingmakeupandstartedtodo sowithoutrealizingit.
TheresultsoftheVRtrainingsupportourhypothesis.Webelieve thatLMCtechnologywillbeusefulbecauseofitscompactsize,high performanceandprecision,andbecauseitofferstheopportunityto implementhuman-machine interaction training into dailyliving activities. In accordance with our philosophy, this system will continuetobedesignedtotrainessentialmovementsfor rehabili-tationandprovideperformancefeedbacktousersandclinicians.
Basedonourfindings,itcanbesaidthatLMC-basedVRgames canbeusedasaneffectiveandfuntrainingmethodforimproving non-dominant hand function that can be integrated in the rehabilitationprotocol.
Somelimitationsofthestudyarethesmallsamplesizeandthe low intensity of the training sessions. Follow-up evaluations shouldbemadeafterthetraining and useropinions shouldbe recorded. Further studies should also investigate whether the resultsobtainedwithVRgamescanbemaintained over along periodoftime. Alargersamplegroupshouldbeusedinfuture studiestoconfirmthepreliminaryresultsofthisstudy.
Conclusion
ThisstudyquantitativelydemonstratedthatVRgamescouldbe effective at improving non-dominant hand function. These VR
games provided a stimulating and fun environment, using the interestsandmotivationsoftheparticipantandworkingwithtask and activity-based techniques. LMC-based VR is easy to use, portableandinexpensiveforoccupationaltherapysessions.
Disclosureofinterest
Theauthorsdeclarethattheyhavenocompetinginterest.
Acknowledgments
We would like to thank all participants who agreed to participate in the study. This project was supported byThe Scientific andTechnologicalResearchCouncilofTurkey(Project Number:1919B011800515).
References
[1]Holden MK. Virtualenvironmentsfor motor rehabilitation.Cyberpsychol Behav2005;8:187–211.
[2]ChiviacowskyS,WulfG.Feedbackaftergoodtrialsenhanceslearning.ResQ ExercSport2007;78:40–7.
[3]ProffittR,ForemanM.Low-costvirtualrealityandgame-basedtechnologiesin rehabilitation.TechnolSpecInteresSectQ2014;24:1–3.
[4]AlimanovaM,BorambayevaS,KozhamzharovaD,KurmangaiyevaN, Ospa-novaD,TyulepberdinovaG,etal.Gamificationofhandrehabilitationprocess usingvirtualrealitytools:usingleapmotionforhandrehabilitation.FirstIEEE IntConfRobotComput2017;1:336–9.
[5]LaverK,GeorgeS,ThomasS,DeutschJE,CrottyM.Virtualrealityforstroke rehabilitation.Stroke2012;43:e20–1.
[6]IosaM,MoroneG,FuscoA,CastagnoliM,FuscoFR,PratesiL,etal.Leapmotion controlledvideogame-basedtherapyforrehabilitationofelderlypatientswith subacutestroke:afeasibilitypilotstudy.TopStrokeRehabil2015;22:306–16. [7]SmeragliuoloAH,HillNJ,DislaL,PutrinoD.Validationoftheleapmotion controller using markered motion capture technology. J Biomech 2016;49:1742–50.
[8]PramodhaM,TilakFrancisTG.Dexteritymeasurementacrosstheagespan(3– 25years)withJebsenHandFunctionTest–anobservationalstudy.IndianJ PhysiotherOccupTher2017;11:144–7.
[9]SearsED,ChungKC.ValidityandresponsivenessoftheJebsen-Taylorhand functiontest.JHandSurgAm2010;35:30–7.
[10]ConsolaroA,BovisF,PistorioA,CimazR,DeBenedettiF,MiniaciA,etal.The ItalianversionoftheJuvenileArthritisMultidimensionalAssessmentReport (JAMAR).RheumatolInt2018;38:1311–3.
[11]LamNW,GohHT,KamaruzzamanSB,ChinAV,PoiPJH,TanMP.Normative dataforhandgripstrengthandkeypinchstrength,stratifiedbyageand genderforamultiethnicAsianpopulation.SingaporeMedJ2016;57:578–84. [12]ChiuHC,AdaL,LeeHM.UpperlimbtrainingusingWiiSportsResortTMfor childrenwithhemiplegiccerebralpalsy:arandomized,single-blindtrial.Clin Rehabil2014;28:1015–24.
[13]TarakciE,ArmanN,TarakciD,KasapcopurO.Leapmotioncontroller–based trainingforupperextremityrehabilitationinchildrenandadolescentswith physicaldisabilities:arandomizedcontrolledtrial.JHandTher2019.1-8. [14]Ferna´ndez-Gonza´lezP,Carratala´-TejadaM,Monge-PereiraE,Collado-Va´zquez
S,Sa´nchez-HerreraBaezaP,Cuesta-Go´mezA,etal.Leapmotioncontrolled videogame-based therapyfor upperlimbrehabilitationinpatients with Parkinson’sdisease:afeasibilitystudy.JNeuroengRehabil2019;16:133. [15]Luna-OlivaL,Ortiz-Gutie´rrezRM,Cano-delaCuerdaR,Pie´drolaRM,
Alguacil-Diego IM,Sa´nchez-CamareroC, et al.KinectXbox360 asa therapeutic modalityforchildrenwithcerebralpalsyinaschoolenvironment:a prelimi-narystudy.NeuroRehabil2013;33:513–21.
[16]KimJJ,GonzalezDA,MintzA,RoyEA,TungJY.Motorcontrolassessmentusing leap motion: filteringmethods and performance in indoorand outdoor environments.In:JaffrayDA,editor. IFMBEproceedingsTorontoCanada, 51.2015.p.1150–4.
[17]ProchnowD,Bermu´deziBadiaS,SchmidtJ,DuffA,BrunheimS,KleiserR,etal. Afunctionalmagneticresonanceimagingstudyofvisuomotorprocessingina virtualreality-basedparadigm:rehabilitationgamingsystem.EurJNeurosci 2013;37:1441–7.
[18]HarvieDS,SmithRT,HunterEV,DavisMG,SterlingM,MoseleyGL.Using visuo-kineticvirtualrealitytoinduceillusoryspinalmovement:theMoOVi illusion.PeerJ2017;5:e3023.