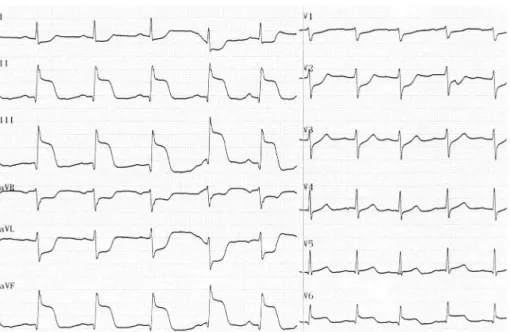
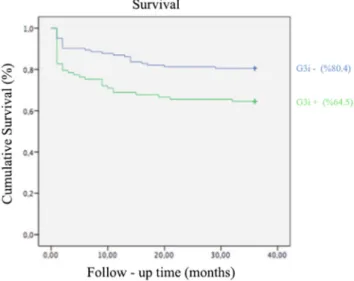
Long-term prognostic significance of terminal QRS distortion on patients with stemi and its correlation with the GRACE scoring system
Tam metin
Şekil

Benzer Belgeler
In this study, among patients with moderate or high car- diovascular risk who underwent moderate-risk surgical opera- tions, approximately one third had postoperative
It has been clearly established that coin- ciding renal function impairment additionally increases the risk mortality and nonfatal adverse events during short- and long- Objective:
In fact, a recent study showed that CMR performed dur- ing index hospitalization with MVO assessment provides bet- ter prognostic stratification of STEMI patients who underwent
Objective: The present study aims to investigate whether the addition of homocysteine level to the Global Registry of Acute Coronary Events (GRACE) risk score enhances its
(17) study with longer follow-up period, we reported an admission PTX3 level as a significant inde- pendent predictor for 5-year adverse cardiac outcomes including
We evaluated the relationship between fQRS and poor coronary collateral circulation and the diagnostic ability of fQRS for myocardial scar detection in patients with chronic
In this study, we examined the expression levels of miRNA related to cardiac diseases in circulating blood among STEMI patients versus a control group to identify miRNA
Presence of fQRS being relation with Tei index and no relation with other parameters being identified suggests that subclinical myocardial injury may be widespread in this
