231
The importance of electrophysiologic support for
carpal tunnel syndrome diagnosis in the elderly
Bilgin Öztürk1 , Akçay Övünç Özön2
1Clinic of Neurology, Gülhane Training and Research Hospital, Ankara, Turkey 2Clinic of Neurology, İstinye University Liv Hospital, Ankara, Turkey
Abstract
Objective: Carpal Tunnel Syndrome (CTS) is the most common entrapment neuropathy that is more common in women and
increases with age. The diagnosis is made clinically and electrophysiological tests contribute diagnosis. The first options in treat-ment include physical therapy programs, pharmacological agents and surgery. In this study, we aimed to investigate the rela-tionship between the diagnosis of CTS and electromyography (EMG) and age.
Methods: In this study, we compared the age of patients with only CTS without muscle weakness or atrophy. A total of 59
patients (group 1 aged <50 years n=30, group 2 aged >65 years n=29) were included in the study. Age, sex, Tinel sign, Phalen sign, carpal compression test, and EMG results were evaluated. In light of the data obtained from the patient records, patients with other diseases that caused their symptoms and those with disorders other than CTS electrophysiologically were excluded from the study.
Results: In the evaluation of EMG results, EMG positivity was found to be higher in older patients and there was no difference
in terms of clinical symptoms. Also, the Tinel sign was correlated with EMG significance in both old and young individuals.
Conclusion: We believe that EMG will give more guidance in older patients than younger individuals in the presence of
sus-pected clinical suspicion of CTS.
Keywords: Carpal tunnel syndrome, elderly, electromyography, Tinel sign, trap neuropathy
INTRODUCTION
Carpal tunnel syndrome (CTS) is the neuropathy of the median nerve trapped in the carpal tunnel. It is more fre-quently seen in women. It is the most common peripheral nerve entrapment neuropathy (1). The pathophysiology of CTS is multifactorial (2). The pressure increase in intracarpal area plays an important role in the development of CTS (3). Although its estimated prevalence varies according to societies, it ranges from 1-5% (4-6). Risk factors for CTS are female sex, obesity, genetic predisposition, aromatase inhibitor use, diabetes, pregnancy, rheumatoid arthritis, hypothyroidism, and connective tissue diseases (7-12).
When the clinical features are examined, it is known that the symptoms usually occur at night. Common symptoms include pain, paresthesia, tingling, numbness, and thenar atrophy in areas that fit the median nerve distribution. These symptoms can only be on the wrist or spread over the entire hand. In some cases, sensory symptoms spread to the forearm and shoulder, but do not affect the neck. Although the symptoms are usually unilateral, it is not un-common to detect them bilaterally. The clinical course may be remission and exacerbation. CTS starts with sensory symptoms and then motor symptoms are added later. These motor symptoms manifest themselves as difficulties in handling activities such as holding objects, knitting, and key turning. In the neurologic examination, provocative maneuvers such as Phalen’s sign, Tinel’s sign, and manual carpal compression tests (CT) contribute to the diagnosis of pain and paresthesia in areas with median nerve innervation.
Carpal tunnel syndrome is diagnosed clinically. Electrodiagnostic tests help confirm the diagnosis of CTS. The general opinion for the diagnosis of CTS is through validation of clinical symptoms and findings by
electrodiag-Corresponding Author: Bilgin Öztürk E-mail: [email protected] Submitted: 28 May 2019 Accepted: 1 September 2019
You may cite this article as: Öztürk B, Övünç Özön A. The importance of electrophysiologic support for carpal tunnel syndrome diagnosis inthe
232
nostic tests. The main electrodiagnostic tests are nerve con-duction studies (NCS). The compression of the median nerve damages the myelin sheath, which results in electrophysio-logically delayed distal latencies and slower velocities. Sen-sory fibers are more sensitive to compression than motor fibers. Therefore, sensory conduction changes are detected in the early period. In some cases, needle electromyography (EMG) support may be required. In addition to validating CTS, electrodiagnostic tests are useful in measuring the se-verity of median nerve stiffness, assisting decisions related to surgical intervention, and monitoring treatment efficacy. The results obtained in electrodiagnostic studies should be compared with other nerves on the same side or contralat-eral hands with age-related normal values. Abnormalities of the ulnar and radial nerves outside the median nerve should also be examined. Therefore, other common causes of neu-ropathy are excluded.
Conservative treatment options should be considered in the treatment of CTS. Among these, the most preferred treat-ments are splinting, steroid injections, oral glucocorticoids, physical treatment methods, and non-steroidal anti-inflam-matory drugs (13-16). In addition, treatment of concomitant systemic diseases (obesity, diabetes, rheumatoid arthritis, other connective tissue diseases and hypothyroidism) may also be effective in relieving CTS symptoms. Surgical treat-ment options can also be used depending on the severity of CTS and the comorbid condition of the patient. The goal of all treatment options is to reduce the pressure on the median nerve and also to eliminate inflammation and edema. Population-based studies have indicated that CTS is common in two different periods, aged 50-54 and 75-84 years (17). It is stated that the clinical and electrophysiologic features of CTS are not well established in the elderly population (18). The aim of this study was to investigate the relationship be-tween age and the association of CTS diagnosis with EMG. Secondly, to determine the clinical and electroneuromyo-graphic characteristics of CTS in the elderly population and to help determine the appropriate treatment options in this age group with correct diagnostic approaches.
METHODS
In this study, a total of 522 patients with CTS who were admit-ted to our Gülhane Training and Research Hospital Neurolo-gy Outpatient Clinic between February 2016 and December 2018 were evaluated. Age, sex, duration of symptoms, neu-rologic examination findings of Tinel sign, Phalen sign, and carpal CT results, and EMG test results were recorded. Patients with wrist trauma/fracture/surgery history, concomitant poly-neuropathy, plexopathy, cervical radiculopathy, diabetes, hy-pothyroidism, connective tissue diseases, and carpal tunnel mass were excluded from the study. Patients aged 50-65 years were not included in the study in order to reveal more
age-re-lated changes. Patients with muscular atrophy and abductor pollicis brevis (APB) muscle weakness were excluded from the study because the muscle atrophy in older individuals may not be related to CTS alone, regardless of the cause. The diag-noses of all patients in the study were accepted as mild CTS because of the absence of thenar atrophy and weakness of APB muscles (19).
According to the exclusion criteria, 59 patient files were in-cluded out of 522 files. Thirty patients were aged under 50 years (group 1) and 29 patients were aged over 65 years (group 2). The duration of symptoms (months), age, sex, ex-amination findings (Tinel sign, Phalen sign, carpal CT) and EMG findings (median nerve motor and sensory latency, am-plitude and velocity) were compared in both groups. In the EMG tests, patients with CTS and concurrent disorders were excluded from the study.
All EMG examinations were performed in the same center using the same device and same procedure. A Medelec Syn-ergy (Viasys, Ireland, 2008) EMG device was used to perform NCS. Distal motor latency (DML) (ms), compound muscle ac-tion potential, amplitude (mV), sensory nerve acac-tion poten-tial (SNAP), amplitude (µV), and velocity (ms) were evaluated. Skin temperature was kept above 31°C. The median and ulnar nerve were stimulated at the wrist using the same distanc-es from the active electrode. Our laboratory’s normal valudistanc-es were: median nerve DML <4.4 ms (7 cm distance), amplitude >4 mv, median sensorial potential amplitude >20 µv, and ve-locity >50 ms (calculated from the onset of the SNAP). Normal ulnar nerve responses were accepted as additional criteria for CTS diagnosis. In patients aged over 65 years, a 10% reduction in velocities and a 10% delay in latencies were considered as normal values for this study.
Carpal tunnel syndrome was diagnosed on EMG by the pres-ence of delayed or abspres-ence median nerve sensory response or a prolonged DML (>4.5 ms).
This study was approved by Gülhane Training and Research Hospital local ethics committee (2018/14-18/315). Patient consent was not obtained because the study was designed as a retrospective study.
Statistical Analysis
The data of the study were analyzed using the SPSS (Statistical Package for the Social Sciences IBM Corp.; Armonk, NY, USA) 22 package program. In the analysis of the variables obtained from the study, mean and standard deviation were used for numerical variables and number and percentage expres-sions were used for categorical variables. In the comparative analysis of categorical variables, the Chi-square test was per-formed. Pearson’s correlation test was performed to evaluate the relationship between variables. p<0.001 was regarded as statistically significant.
233
RESULTSThe mean age of the patients included in the study was 39.17±6.25 (range, 27-48) years, and 71.93±5.27 (range,
65-83) years for groups 1 and 2, respectively. No statistically significant difference was found between the two groups in terms of sex (Table 1).
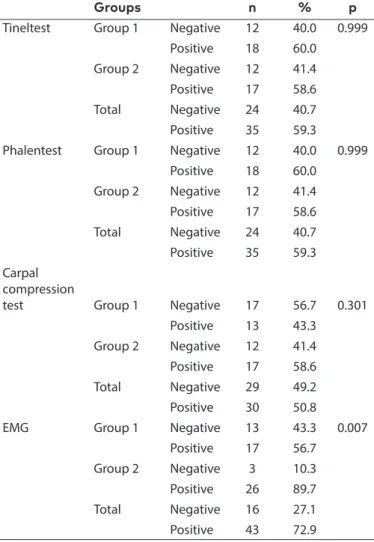
There was no statistically significant difference between the groups in the comparison of frequency and positivity of Tinel and Phalen tests for physical examination methods used for the diagnosis of CTS (p>0.005). There was no statistical differ-ence between the groups in terms of carpal CT. In the evalua-tion of EMG results, EMG positivity was significantly higher in the older age group. There was no statistically significant dif-ference in the clinical evaluation of the study according to the age groups, but the laboratory evaluations were significantly higher in group 2 (Table 2).
When we compared the relationship between the variables in terms of clinical significance, there was a statistically significant and positive correlation between EMG results and Tinel sign results and carpal CT in group 1 (p=0.036, r=0.384, and p=0.006, r=0.493, respectively). In group 2, the correlation between EMG results and Tinel sign results was statistically significant and moderate (p=0.030, r=0.404). However, the same correlation was not statistically signifi-cant between EMG and other examination tests (Phalen and Carpal CT).
DISCUSSION
In this study, individuals with pure CTS were compared ac-cording to age and it was shown that clinical and electro-physiologic results were affected by age. Electroelectro-physiologic abnormalities in older adults with CTS were higher than those of young adults, and they were more supportive of clinical CTS diagnosis. In subgroup analysis, it was seen that CTS was more frequent in both groups. The results of this study show that electrophysiologic tests support that the clinical diagno-sis is higher in the detection of CTS in the elderly population. It has been demonstrated that CTS can be elicited early in electrophysiologic studies in older patients by exclusion of patients with muscle atrophy, which is considered as a severe CTS indicator.
Some features of peripheral nerves such as demyelination, loss of myelinated and unmyelinated fibers, and delayed re-generation have been shown to be significantly affected by the expression of major myelin proteins in aging. The diag-nosis should be confirmed through electrodiagnostic studies. Electrodiagnostic parameters are different in older age and false-negative and false-positive results are encountered (20). Hand function is important in daily life activities, especially in older people with many limitations. It is very important to diagnose compression of the median nerve, which is respon-sible for hand skills, early and correctly. Although electrodiag-nostic studies are widely used as diagelectrodiag-nostic reference meth-ods, deficiencies in the diagnosis of CTS have led physicians to seek alternative methods (20).
Age p Group 1 (n=30) Mean 39.17 <0.001 Median 40.00 Group 2 (n=29) Mean 71.93 Median 70.00 Total (n=59) Mean 55.27 Median 48.00 Sex n % Group 1 (n=30) Female 17 56.7 0.999 Male 13 43.3 Group 2 (n=29) Female 16 55.2 Male 13 44.8 Total (n=59) Female 33 55.9 Male 26 44.1
Table 1. Demographic distribution of patients (group 1: aged <50 years, group 2: aged >65 years)
Groups n % p
Tineltest Group 1 Negative 12 40.0 0.999 Positive 18 60.0 Group 2 Negative 12 41.4
Positive 17 58.6 Total Negative 24 40.7
Positive 35 59.3 Phalentest Group 1 Negative 12 40.0 0.999
Positive 18 60.0 Group 2 Negative 12 41.4 Positive 17 58.6 Total Negative 24 40.7 Positive 35 59.3 Carpal compression
test Group 1 Negative 17 56.7 0.301 Positive 13 43.3 Group 2 Negative 12 41.4
Positive 17 58.6 Total Negative 29 49.2
Positive 30 50.8 EMG Group 1 Negative 13 43.3 0.007
Positive 17 56.7 Group 2 Negative 3 10.3 Positive 26 89.7 Total Negative 16 27.1 Positive 43 72.9 EMG: electromyography
Table 2. Clinical symptoms and EMG evaluation between young and older patients (group 1: aged <50 years, group 2: aged >65 years)
234
Older patients with CTS tend to have advanced symptoms. It also affects aging, axonal integrity, and the myelination of fibers, reducing nerve conduction velocity in EMG in symp-tom-free individuals and causing a slight abnormality. The contribution of parameters such as age, sex, body mass index, and hand used in the development of symptoms in patients with CTS is important. It is very important to have a sensitive and accurate screening method that helps diagnose and treat the elderly as soon as possible (20).
The relation between age and clinical presentation of CTS and electrodiagnostic technique is not clear because of the differences in technique, expert experience, and electrodiag-nostic criteria. In one study, it was reported that the incidence in male patients increased with age, and peaked between 45-54 years of age in female patients (21). In a study by Seror, paresthesia and symptom duration were found to be more frequent in patients aged over 70 years (22). In another study, a positive relationship was found between age and hand function symptoms, but there was no positive relationship between age and severity of symptoms (23).
In a study conducted by Blumenthal et al., CTS in the elderly was examined in detail. They reported that electrophysiologic abnormalities were 3.2 times higher in younger patients aged over 65 years compared with older patients with mild CTS symptoms (18). They also stated that clinical findings were more common in the elderly. We consider that the inclusion of patients with severe CTS had a role in this study because we found no significant difference between the elderly and young individuals in terms of clinical symptoms in patients with only mild CTS in our study. In the same study, it was not-ed that atherosclerosis was more frequent in older individuals. In our study, the presence of Tinel sign showed parallel to electrophysiologic confirmation in both older and young in-dividuals. A similar effect was not observed in the Phalen sign. When Blumenthal et al. evaluated the Tinel and Phalen signs, they found no difference between the elderly and young peo-ple (18).
In conclusion, we planned to exclude the clinical manifesta-tions or electrophysiologic disorders that might occur due to aging or other comorbidities, especially in patients with only mild CTS. In older patients, age-related developing muscle at-rophy may lead to errors in the diagnosis of CTS. In contrast, CTS-induced muscle atrophy can even be accidentally eval-uated by the patient and may lead to a delay in diagnosis. In this way, only the relationships of CTS with age were revealed. Our study procedure was well defined and we used common-ly used clinical and electrodiagnostic criteria to identify CTS. Accurate detection of CTS in the elderly will make treatment management easier and more effective. In this way, unnec-essary or incorrect drug use of patients will be prevented.
Electrophysiologic findings in older patients were found to be more common even in the early period than in younger patients. The electrophysiologic evidence of CTS, which we see as changing according to age, should be developed by prospective, multicenter, and controlled studies.
Ethics Committee Approval: Ethics committee approval was
re-ceived for this study from the ethics committee of Gülhane Training and Research Hospital local ethics committee (2018/14-18/315).
Informed Consent: Due to the retrospective design of the study, informed consent was not taken.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept – B.Ö.; Design – B.Ö.; Supervision – A.Ö.Ö.; Resources – B.Ö.; Materials – A.Ö.Ö.; Data Collection and/ or Processing – A.Ö.Ö.; Analysis and/or Interpretation – A.Ö.Ö.; Liter-ature Search – B.Ö.; Writing Manuscript – B.Ö.; Critical Review – B.Ö.
Conflict of Interest: The authors have no conflicts of interest to
declare.
Financial Disclosure: The authors declared that this study has
re-ceived no financial support. REFERENCES
1. Middleton SD, Anakwe RE. Carpal tunnel syndrome. BMJ 2014;
349: g6437. [CrossRef]
2. Kozak A, Schedlbauer G, Wirth T, Euler U, Westermann C, Nien-haus A. Association between work-related biomechanical risk factors and the occurrence of carpal tunnel syndrome: an over-view of systematic reover-views and a meta-analysis of current
re-search. BMC Musculoskelet Disord 2015; 16: 231. [CrossRef]
3. Kubo K, Zhou B, Cheng YS, et al. Ultrasound elastography for car-pal tunnel pressure measurement: A cadaveric validation study.
J Orthop Res 2018; 36: 477-483. [CrossRef]
4. Atroshi I, Englund M, Turkiewicz A, Tägil M, Petersson IF. In-cidence of physician-diagnosed carpal tunnel syndrome in the general population. Arch Intern Med 2011; 171: 943-944. [CrossRef]
5. Gelfman R, Melton LJ 3rd, Yawn BP, Wollan PC, Amadio PC, Ste-vens JC. Long-term trends in carpal tunnel syndrome.
Neurolo-gy 2009; 72: 33-41. [CrossRef]
6. Pourmemari MH, Heliövaara M, Viikari-Juntura E, Shiri R. Carpal tunnel release: Lifetime prevalence, annual incidence, and risk
factors. Muscle Nerve 2018; 58: 497-502. [CrossRef]
7. Padua L, Coraci D, Erra C, et al. Carpal tunnel syndrome: clinical features, diagnosis, and management. Lancet Neurol 2016; 15:
1273-1284. [CrossRef]
8. Shiri R, Pourmemari MH, Falah-Hassani K, Viikari-Juntura E. The effect of excess body mass on the risk of carpal tunnel syn-drome: a meta-analysis of 58 studies. Obes Rev 2015; 16:
1094-1104. [CrossRef]
9. Jackson R, Beckman J, Frederick M, Musolin K, Harrison R. Rates of Carpal Tunnel Syndrome in a state workers’ compensation information system, by industry and occupation - California, 2007-2014. MMWR Morb Mortal Wkly Rep 2018; 67: 1094-1097. [CrossRef]
235
10. Mediouni Z, de Roquemaurel A, Dumontier C, et al. Is carpal tunnel syndrome related to computer exposure at work? A re-view and meta-analysis. J Occup Environ Med 2014; 56: 204-208. [CrossRef]
11. Shiri R. Hypothyroidism and carpal tunnel syndrome: a
me-ta-analysis. Muscle Nerve 2014; 50: 879-883. [CrossRef]
12. Sestak I, Sapunar F, Cuzick J. Aromatase inhibitor-induced carpal tunnel syndrome: results from the ATAC trial. J Clin Oncol 2009;
27: 4961-4965. [CrossRef]
13. Akarsu S, Karadaş Ö, Tok F, Levent Gül H, Eroğlu E. Single versus repetitive injection of lignocaine in the management of carpal tunnel syndrome--a randomized controlled trial. J Hand Surg
Eur Vol 2015; 40: 179-183. [CrossRef]
14. Atroshi I, Flondell M, Hofer M, Ranstam J. Methylpredniso-lone injections for the carpal tunnel syndrome: a randomized, placebo-controlled trial. Ann Intern Med 2013; 159: 309-317. [CrossRef]
15. Page MJ, Massy-Westropp N, O’Connor D, Pitt V. Splinting for carpal tunnel syndrome. Cochrane Database Syst Rev 2012; 7:
CD010003. [CrossRef]
16. Horng YS, Hsieh SF, Tu YK, Lin MC, Horng YS, Wang JD. The com-parative effectiveness of tendon and nerve gliding exercises in
patients with carpal tunnel syndrome: a randomized trial. Am J
Phys Med Rehabil 2011; 90: 435-442. [CrossRef]
17. Bland JD, Rudolfer SM. Clinical surveillance of carpal tunnel syn-drome in two areas of the United Kingdom, 1991-2001. J Neurol
Neurosurg Psychiatry 2003; 74: 1674-1679. [CrossRef]
18. Blumenthal S, Herskovitz S, Verghese J. Carpal tunnel syndrome
in older adults. Muscle Nerve 2006; 34: 78-83. [CrossRef]
19. Bland JD. A neurophysiological grading scale for carpal tunnel
syndrome. Muscle Nerve 2000; 23: 1280-1283. [CrossRef]
20. Salman Roghani R, Hashemi SE, Holisaz MT, Gohari F, Delbari A, Lokk J. The diagnostic accuracy of median nerve ultrasonogra-phy in elderly patients with carpal tunnel syndrome: sensitivity and specificity assessment. Clin Interv Aging 2018; 13:
1953-1962. [CrossRef]
21. Nakasato YR. Carpal tunnel syndrome in the elderly. J Okla State Med Assoc 2003; 96: 113-115.
22. Seror P. Carpal tunnel syndrome in the elderly. “Beware of severe
cases”. Ann Chir Main Memb Super 1991; 10: 217-225. [CrossRef]
23. Padua L, Padua R, Lo Monaco M, Aprile I, Tonali P. Multiper-spective assessment of carpal tunnel syndrome: a multicenter study. Italian CTS Study Group. Neurology 1999; 53: 1654-1659. [CrossRef]