Abstract
Background: Fasting during the holy month of Ramadan is a religious obligation for all Muslims who represent 1.8 billion of the world population (24%). This study explores the effect of Ramadan fasting on the blood glucose, glycated hemoglobin (HbA1c), lipid profile, sleeping quality, and essential lifestyle parameters and also explores the safety of fasting for a whole month among diabetic patients. Aim: The aim of the present study was to assess the impact of Ramadan fasting on the blood glucose, HbA1c, lipid profile, sleeping quality, and lifestyle parameters among patients with type 2 diabetes mellitus (T2DM) in Turkey. Subjects and Methods: A total of 1780 diabetic patients were approached, and 1246 (70%) participated in this cross-sectional study carried out during the period from May 27, 2017, to June 24, 2017. Data analysis comprised sociodemographic features, lifestyle habits, blood pressure measurements, serum lipid profiles, serum calcium, Vitamin D 25-hydroxy, uric acid, and HbA1c at before 4 weeks and after 12 weeks from Ramadan. Results: Out of 1246 patients, 593 (47.6%) were male and 653 (52.4%) were female. The mean ± standard deviation age of the patients was 50.39 ± 15.3 years. Males were significantly older than females (51.53 ± 12.56 vs. 49.26 ± 14.4; P = 0.003, respectively). Significant differences were found in Vitamin D, blood glucose, HbA1c level, creatinine, bilirubin, albumin, total cholesterol, triglycerides, high-density lipoprotein-cholesterol (female), low-density lipoprotein-cholesterol (male), uric acid, and systolic and diastolic blood pressure after and before the holy month of Ramadan (P < 0.05 for each). HbA1c (P < 0.001), physical activity (P < 0.001), hours of sleeping (P < 0.001), systolic blood pressure (BP) (mmHg) (P = 0.007), BMI (P = 0.016), diastolic BP (mmHg) (P = 0.018), family history (P = 0.021), and smoking (P = 0.045) were identified as significantly associated with Ramadan fasting as contributing factors. Conclusion: In one of the largest studies of its kind, we show that Ramadan fasting has positive effects on T2DM patients as it reduces their blood pressure, blood glucose, HbA1C, and BMI. Furthermore, there are improvements in the duration of sleep and physical activity, the role of Ramadan fasting in diabetes therapy has been confirmed.
Keywords: Body mass index, diabetes mellitus, glycated hemoglobin, Ramadan fasting, sleeping quality
Access this article online
Quick Response Code:
Website:
www.annalsafrmed.org DOI:
10.4103/aam.aam_63_17
Address for correspondence: Prof. Abdülbari Bener,
Department of Biostatistics and Medical Informatics, Cerrahpasa Faculty of Medicine, International School of Medicine, Istanbul University and Istanbul Medipol University, 34098 Cerrahpasa, Istanbul, Turkey. E‑mail: [email protected] This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
How to cite this article: Bener A, Al-Hamaq AO, Öztürk M, Çatan F,
Haris PI, Rajput KU, et al. Effect of ramadan fasting on glycemic control and other essential variables in diabetic patients. Ann Afr Med 2018;17:196-202.
Effect of Ramadan Fasting on Glycemic Control and other
Essential Variables in Diabetic Patients
Abdülbari Bener1,2,3, Abdulla O. A. A. Al‑Hamaq4, Mustafa Öztürk3, Funda Çatan1,5, Parvez I. Haris6, Kaleem U. Rajput7, Abdülkadir Ömer3
1Department of Biostatistics and Medical Informatics, Cerrahpasa Faculty of Medicine, Istanbul University, 3Department of Endocrinology, Regenerative and Resorative Medicine Research Centre, International School of Medicine, Istanbul Medipol University, Istanbul, 5Department of Computer Education and Instructional Technologies, Faculty of Education, University of Kastamonu, Kastamonu, Turkey, 2Department of Evidence for Population Health Unit, School of Epidemiology and Health Sciences,
The University of Manchester, Manchester, 6Department School of Allied Health Sciences, Faculty of Health and Life Sciences, De Montfort University, Leicester, 7 Department of Biomedical Science, Faculty of Medicine, Health Care and Social Sciences, St George’s University of London, London, UK, 4Qatar Diabetic Association
and Qatar Foundation for Research, Doha, Qatar
Résumé
Contexte: Le jeûne pendant le mois sacré du Ramadan est une obligation religieuse pour tous les musulmans qui représentent 1,8 milliard de personnes dans le monde population (24%). Cette étude explore l’effet du jeûne du Ramadan sur la glycémie, l’hémoglobine glyquée (HbA1c), le profil lipidique, qualité de sommeil, et les paramètres essentiels de style de vie et explore également la sécurité du jeûne pour un mois entier chez les patients diabétiques. But: Le but de la présente
étude était d’évaluer l’impact du jeûne du Ramadan sur la glycémie, l’HbA1c, le profil lipidique, le sommeil paramètres de qualité et de style de vie chez les patients atteints de diabète sucré de type 2 (DT2) en Turquie. Sujets et méthodes: Un total de 1780 patients diabétiques ont été approchés, et 1246 (70%) ont participé à cette étude transversale réalisée au cours de la période Du 27 mai 2017 au
I
ntroductIon
Ramadan fasting is one of the five main pillars of Islam that is
practiced by over one and a half billion people.
[1-3]Fasting during
Ramadan is a mandatory duty for all healthy sane Muslims, and
they should endure without food, drink, oral medications, smoking,
and other sensual pleasures from break of dawn to sunset.
[1-7]Numerous studies have mentioned the biochemical alterations
while fasting among both in nondiabetic patients and diabetic
patients.
[1-7]The population-based Epidemiology of Diabetes
and Ramadan 1422/2001 study performed among 12,243
people in 13 Islamic countries and reported that approximately
43% of Muslims with type 1 diabetes and 79% of Muslims with
type 2 diabetes fast during Ramadan.
[2]Furthermore, more than
50 million Muslims who have diabetes fast during Ramadan.
[2]Diabetes mellitus
[1,5]and cardiovascular diseases
[3,8-10]are
reaching epidemic proportions worldwide and lead to
important public and personal burden.
[2]Furthermore, diabetes
mellitus is a primary reason of mortality and morbidity in
many developed and developing countries.
[7-9]Ramadan fasting
change lifestyle of Muslims for one lunar month that may
have an impact on diabetic and cardiac patients
[2-4,10,11]because
during the Ramadan Muslims eat meals before dawn and after
sunset. The alteration in meal schedule has an effect on sleep
habit, lifestyle properties, and diabetes complications.
[11-16]The
aim of the present study was to assess the impact of Ramadan
fasting on the blood glucose, glycated hemoglobin (HbA1c),
lipid profile, sleeping quality, and lifestyle parameters among
patients with type 2 diabetes mellitus (T2DM) in Turkey.
s
ubjects
and
M
ethods
This cross-sectional study was conducted among Turkish adult
patients with T2DM in the Medipol Hospitals. Institutional
Review Board ethical clearance for this study was given by the
International School of Medicine, Istanbul Medipol University.
The study comprised patients with T2DM who treated at the
Medipol International Hospital at the time of the study. The
diagnosis of DM was assigned by the documentation in the
patient’s previous or current medical records.
[15-17]The study design was a nonrandomized interventional
controlled from May 27, 2017 to June 24, 2017 in two periods
as follows: first period (4 weeks before Ramadan) and the
second period (4 weeks after Ramadan). The exclusion
criteria of the current study were serious comorbidities
such as renal diseases, alertness problems, newly diagnosed
T2DM (18 months), hospitalization a short time ago,
unawareness of hypoglycemia, and partially or completely
nonfasting during the month of Ramadan.
The sample size calculation was based on previous studies that
determined the prevalence of T2DM and MetSyn in Turkey
[16,18]to be between 16.2%, with the 99% confidence level and
with 2.5% error of estimation, the minimum sample size for
the current study was 1780. Patients were recruited by the
systematic 1-in-2 sampling procedure. Although 1780 patients
were approached, 1246 (70%) patients agreed to participate in
this study. One hundred patients were used to determine content
validity, face validity, and reliability of the questionnaire. The
questionnaire has a high level of validity and a high degree of
repeatability (κ = 0.86).
Data collection methods: Questionnaire
This research comprised sociodemographic and lifestyle
characteristics such as age, gender, marital status, level
of education, occupation, Body Mass Index (BMI),
physical activity, the frequency of fast food consumption,
and smoking habits, clinical data including systolic and
diastolic blood pressures (DBP). Laboratory investigations
were performed to examine blood glucose, HbA1c,
high-density lipoprotein-cholesterol (HDL-C), low-density
lipoprotein-cholesterol (LDL-C), cholesterol, triglyceride,
urea, creatinine, bilirubin, albumin, calcium, Vitamin D
25-hydroxy (25-OH), and uric acid before and after Ramadan.
BMI was calculated as the ratio of weight (kilogram) to
the square of height (meters). The patient was classified as
obese if the value of BMI was ≥30 kg/m
2, overweight if BMI
was >25 kg/m
2, and normal if BMI <20 kg/m
2.
[12,16]In line
with the World Health Organization guidelines, hypertension
was evaluated as systolic blood pressure ≥130 mmHg or
DBP ≥85 mmHg or using anti-hypertensive medication.
[12,16,19]24 juin 2017. L’analyse des données comprenait des caractéristiques sociodémographiques, des habitudes de vie, des mesures de la tension artérielle, les profils sériques des lipides, le calcium sérique, la vitamine D 25-hydroxy, l’acide urique et l’HbA1c avant 4 semaines et après 12 semaines de Ramadan. Résultats: Sur 1246 patients, 593 (47,6%) étaient des hommes et 653 (52,4%) étaient des femmes. L’âge moyen ± écart-type des patients était de 50,39 ± 15,3 ans. Les mâles étaient significativement plus âgés que les femelles (51,53 ± 12,56 contre 49,26 ± 14,4, P = 0,003, respectivement). Important différences ont été trouvées dans la vitamine D, la glycémie, le taux d’HbA1c, la créatinine, la bilirubine, l’albumine, le cholestérol total, les triglycérides, la densité lipoprotéine-cholestérol (femelle), lipoprotéine-cholestérol de basse densité (mâle), acide urique et tension artérielle systolique et diastolique après et avant le mois sacré du Ramadan (P <0,05 pour chacun). HbA1c (P < 0,001), activité physique (P <0,001), heures de sommeil (P <0,001), tension artérielle systolique (TA) (mmHg) (P = 0,007), IMC (P = 0,016), TA diastolique (mmHg) (P = 0,018), antécédents familiaux (P = 0,021), et le tabagisme (P = 0,045) a été identifié comme étant significativement associé au jeûne du Ramadan en tant que facteurs contributifs. Conclusion: Dans l’un des les plus grandes études de son genre, nous montrons que le jeûne du Ramadan a des effets positifs sur les patients atteints de DT2 car il réduit leur tension artérielle, le sang glucose, HbA1C et BMI. En outre, il y a des améliorations dans la durée du sommeil et de l’activité physique, le rôle du jeûne du Ramadan dans la thérapie du diabète a été confi rmée.
Smoking habits were classified as being past, current smoker
or nonsmoker. Patients were categorized as physically active
if they walked or cycled for more than 30 min a day.
Laboratory measurements
After 10 h of fasting, blood sample (10 ml) were collected
from the patients. Subsequently, different blood parameters
were determined in a central certified laboratory at the
Medipol Hospital. Plasma glucose, total cholesterol,
triglyceride, HDL-C, and LDL-C were measured using an
auto-analyzer (ROCHE COBAS 6000). A high-performance
liquid chromatography method was used to evaluate HbA1c
concentration.
[12,18]Statistical analysis
Student’s paired t-test was performed to specify the differences
between biochemistry parameters 4 weeks before and 12 weeks
after while the Wilcoxon signed-rank test was used for the
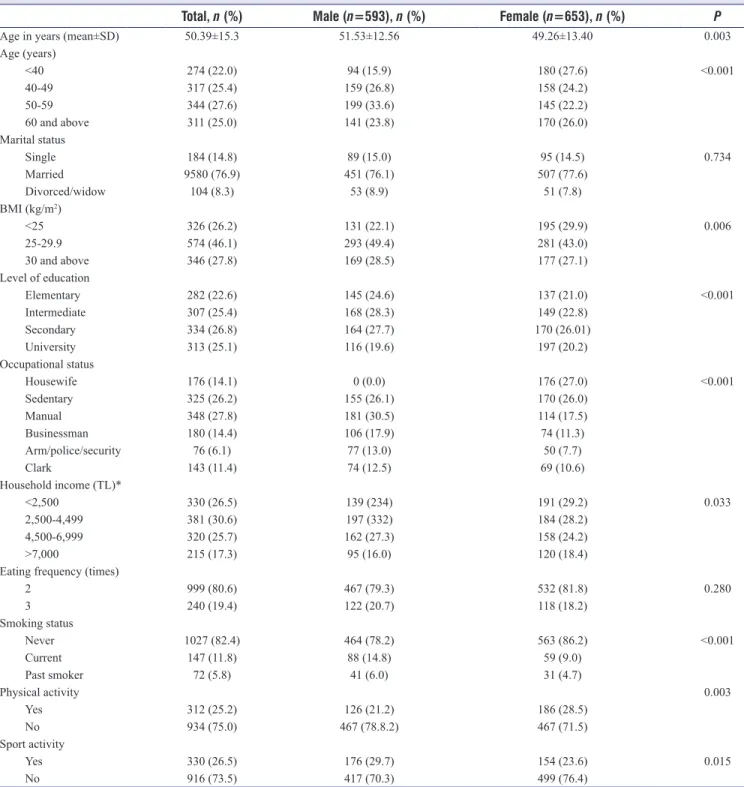
Table 1: Comparison of sociodemographic characteristics of the participants in Istanbul, Turkey (
n=1246)
Total, n (%) Male (n=593), n (%) Female (n=653), n (%) P
Age in years (mean±SD) 50.39±15.3 51.53±12.56 49.26±13.40 0.003
Age (years) <40 274 (22.0) 94 (15.9) 180 (27.6) <0.001 40-49 317 (25.4) 159 (26.8) 158 (24.2) 50-59 344 (27.6) 199 (33.6) 145 (22.2) 60 and above 311 (25.0) 141 (23.8) 170 (26.0) Marital status Single 184 (14.8) 89 (15.0) 95 (14.5) 0.734 Married 9580 (76.9) 451 (76.1) 507 (77.6) Divorced/widow 104 (8.3) 53 (8.9) 51 (7.8) BMI (kg/m2) <25 326 (26.2) 131 (22.1) 195 (29.9) 0.006 25-29.9 574 (46.1) 293 (49.4) 281 (43.0) 30 and above 346 (27.8) 169 (28.5) 177 (27.1) Level of education Elementary 282 (22.6) 145 (24.6) 137 (21.0) <0.001 Intermediate 307 (25.4) 168 (28.3) 149 (22.8) Secondary 334 (26.8) 164 (27.7) 170 (26.01) University 313 (25.1) 116 (19.6) 197 (20.2) Occupational status Housewife 176 (14.1) 0 (0.0) 176 (27.0) <0.001 Sedentary 325 (26.2) 155 (26.1) 170 (26.0) Manual 348 (27.8) 181 (30.5) 114 (17.5) Businessman 180 (14.4) 106 (17.9) 74 (11.3) Arm/police/security 76 (6.1) 77 (13.0) 50 (7.7) Clark 143 (11.4) 74 (12.5) 69 (10.6) Household income (TL)* <2,500 330 (26.5) 139 (234) 191 (29.2) 0.033 2,500-4,499 381 (30.6) 197 (332) 184 (28.2) 4,500-6,999 320 (25.7) 162 (27.3) 158 (24.2) >7,000 215 (17.3) 95 (16.0) 120 (18.4)
Eating frequency (times)
2 999 (80.6) 467 (79.3) 532 (81.8) 0.280 3 240 (19.4) 122 (20.7) 118 (18.2) Smoking status Never 1027 (82.4) 464 (78.2) 563 (86.2) <0.001 Current 147 (11.8) 88 (14.8) 59 (9.0) Past smoker 72 (5.8) 41 (6.0) 31 (4.7) Physical activity 0.003 Yes 312 (25.2) 126 (21.2) 186 (28.5) No 934 (75.0) 467 (78.8.2) 467 (71.5) Sport activity Yes 330 (26.5) 176 (29.7) 154 (23.6) 0.015 No 916 (73.5) 417 (70.3) 499 (76.4)
nonparametric dataset. Chi-square and Fisher’s exact tests were
used to determine for differences in proportions of categorical
variables between two or more groups. A multivariable linear
regression model with step-wise elimination was performed to
Table 2: The comparison of biochemical characteristics and blood pressures among males and females before and after
Ramadan (n=1246)
Blood investigations Mean±SD Change (after‑before) (95% CI) P
After Ramadan Before Ramadan Vitamin D 25-OH
Male 20.70±10.74 19.11±10.50 1.59 (1.59-1.40) <0.001
Female 21.20±10.82 19.64±10.56 1.56 (1.43-1.68) <0.001
Blood glucose (mmol/L)
Male 7.18±1.17 9.14±2.10 −1.95 (−2.098-−1.81) <0.001 Female 7.39±1.09 9.82±2.03 −2.43 (−2.56-−2.94) <0.001 HbA1c Male 7.54±1.13 8.77±1.20 −1.23 (−1.34-−1.12) <0.001 Female 7.40±1.09 9.21±1.13 −1.81 (−1.93-−1.69) <0.001 Calcium (mmol/L) Male 4.03±1.70 3.05±1.97 0.97 (0.17-1.78) 0.018 Female 3.72±1.91 3.02±2.58 0.70 (0.22-1.17) 0.004 Urea (mmol/L) Male 5.39±2.17 5.61±3.14 −0.22 (−0.49-0.37) 0.092 Female 4.94±1.59 5.11±2.09 −0.17 (−0.35-−0.02) 0.076 Creatinine (mmol/L) Male 72.09±32.88 70.35±29.19 1.73 (0.11-3.36) 0.036 Female 67.27±34.45 64.55±27.75 2.72 (1.14-4.29) 0.010 Bilirubin (mmol/L) Male 7.72±3.63 8.64±3.01 −0.92 (−1.45-−0.39) <0.001 Female 7.50±3.63 8.56±2.04 −1.05 (−1.55-−0.55) <0.001 Albumin (mmol/L) Male 38.13±4.46 40.47±4.79 −3.44 (−3.85-−3.03) <0.001 Female 36.82±3.93 40.47±3.93 −3.66 (−4.10-−3.19) <0.001 Cholesterol (mmol/L) Male 3.22±1.21 4.75±1.07 −1.52 (−1.62-−1.42) <0.001 Female 3.27±1.23 4.81±0.98 −1.54 (−1.64-−1.44) <0.001 Triglycerides (mmol/L) Male 1.52±0.46 1.63±0.75 −0.11 (−0.17-−0.33) <0.001 Female 1.51±0.42 1.64±0.71 −0.12 (−0.27-−0.20) <0.001 HDL-C (mmol/L) Male 1.06±0.21 1.08±0.28 −0.02 (−0.04-−0.03) 0.068 Female 1.07±0.20 1.09±0.27 −0.02 (−0.04-−0.01) 0.021 LDL-C (mmol/L) Male 2.00±0.89 1.82±0.97 0.19 (−0.24-−0.06) 0.001 Female 2.07±0.84 1.94±0.80 0.13 (−0.21-−0.08) 0.077
Uric acid (mmol/L)
Male 283.9±89.3 269.1±72.7 14.10 (6.61-21.6) <0.001 Female 286.5±88.9 272.2±65.5 14.4 (7.30-21.5) <0.001 SBP (mmHg) Male 128.5±14.4 135.4±14.6 −6.5 (−7.45-−5.54) 0.010 Female 128.9±14.2 136.1±15.1 −7.3 (−8.16-−6.44) <0.001 DBP (mmHg) Male 76.7±9.9 78.3±8.7 −2.4 (−3.5-−1.35) 0.018 Female 78.1±8.5 78.8±8.5 −0.75 (−1.67-−1.69) 0.004 BMI Male 26.54±4.15 28.00±4.32 −1.46 (−1.52-−1.39) <0.001 Female 25.93±4.00 27.42±4.20 −1.49 (−1.55-−1.40) <0.001
Two-sided P values based on pair t-test. SD=Standard deviation, BMI=Body mass index, 25-OH=25-hydroxy, HDL-C=High-density
lipoprotein-cholesterol, LDL-C=Low-density lipoprotein- cholesterol, SBP=Systolic blood pressure, DBP=Diastolic blood pressure, HbA1c=Glycated hemoglobin, CI=Confidence interval
evaluate the association between dependent and independent
variables and to predict potential factors for diabetes. Statistical
significance was accepted at the P < 0.05 level.
r
esults
Table 1 presents sociodemographic and lifestyle characteristics
of the participants (n = 1246). Out of 1246 patients, 593 (47.6%)
were male and 653 (52.4%) were female. The mean ± standard
deviation (SD) age of the participants was 50.39 ± 15.3 years.
Males were significantly older than females (51.53 ± 12.56 vs.
49.26 ± 13.4; P = 0.003, respectively). There were significant
differences between females and males in the level of
education, occupation, smoking status, physical, and sporting
activity.
Table 2 presents the mean of biochemical characteristics and
blood pressures among males and females before 4 weeks and
after 12 weeks of Ramadan. The significant differences were
found in serum Vitamin D 25-OH, blood glucose, HbA1c level,
creatinine, bilirubin, albumin, total cholesterol, triglycerides,
HDL-C (female), LDL-C (male), uric acid, systolic and DBP
before and after Ramadan (P < 0.05 for each). Furthermore,
there were significant differences in the number of sleeping hours
between during and after Ramadan (5.61 ± 0.58 vs. 6.93 ± 0.72;
P < 0.001, respectively).
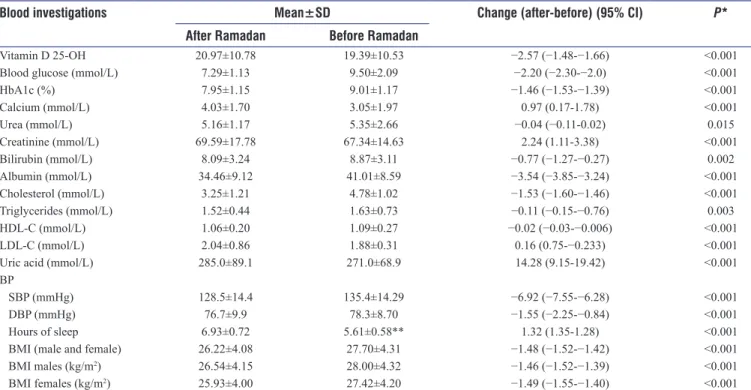
Table 3 shows the comparison of average biochemical
characteristics and blood pressures among the participants
before 4 weeks and after 12 weeks of Ramadan. There were
significant differences Vitamin D 25-OH, blood glucose,
Table 4: Multivariable linear regression analysis to show predictors and effect of Ramadan fasting on different
biochemical and anthropometric parameters in diabetic patients
Independent variables Unstandardized coefficient (B) SE Standardized coefficient (β) t P
HbA1c level −3.530 0.984 −0.231 −3.587 <0.001
Less physical activity −4.939 1.267 −0.330 −3.898 <0.001
Less hours of sleeping −2.856 0.787 −0.229 −3.628 <0.001
SBP (mmHg) −2.320 0.858 −0.176 −2.703 0.007
BMI (kg/m2) −3.761 1.545 −0.215 −2.434 0.016
DBP (mmHg) −2.121 0.890 −0.155 −2.383 0.018
Family history −2.094 0.897 −0.145 −2.334 0.021
Smoking (yes) −2.657 1.321 −0.129 −2.011 0.045
SE=Standard error, SBP=Systolic blood pressure, DBP=Diastolic blood pressure, HbA1c=Glycated hemoglobin, BMI=Body mass index
Table 3: The comparison of biochemical characteristics and blood pressures among patients before and after
Ramadan (n=1246)
Blood investigations Mean±SD Change (after‑before) (95% CI) P*
After Ramadan Before Ramadan
Vitamin D 25-OH 20.97±10.78 19.39±10.53 −2.57 (−1.48-−1.66) <0.001
Blood glucose (mmol/L) 7.29±1.13 9.50±2.09 −2.20 (−2.30-−2.0) <0.001
HbA1c (%) 7.95±1.15 9.01±1.17 −1.46 (−1.53-−1.39) <0.001 Calcium (mmol/L) 4.03±1.70 3.05±1.97 0.97 (0.17-1.78) <0.001 Urea (mmol/L) 5.16±1.17 5.35±2.66 −0.04 (−0.11-0.02) 0.015 Creatinine (mmol/L) 69.59±17.78 67.34±14.63 2.24 (1.11-3.38) <0.001 Bilirubin (mmol/L) 8.09±3.24 8.87±3.11 −0.77 (−1.27-−0.27) 0.002 Albumin (mmol/L) 34.46±9.12 41.01±8.59 −3.54 (−3.85-−3.24) <0.001 Cholesterol (mmol/L) 3.25±1.21 4.78±1.02 −1.53 (−1.60-−1.46) <0.001 Triglycerides (mmol/L) 1.52±0.44 1.63±0.73 −0.11 (−0.15-−0.76) 0.003 HDL-C (mmol/L) 1.06±0.20 1.09±0.27 −0.02 (−0.03-−0.006) <0.001 LDL-C (mmol/L) 2.04±0.86 1.88±0.31 0.16 (0.75-−0.233) <0.001
Uric acid (mmol/L) 285.0±89.1 271.0±68.9 14.28 (9.15-19.42) <0.001
BP
SBP (mmHg) 128.5±14.4 135.4±14.29 −6.92 (−7.55-−6.28) <0.001
DBP (mmHg) 76.7±9.9 78.3±8.70 −1.55 (−2.25-−0.84) <0.001
Hours of sleep 6.93±0.72 5.61±0.58** 1.32 (1.35-1.28) <0.001
BMI (male and female) 26.22±4.08 27.70±4.31 −1.48 (−1.52-−1.42) <0.001
BMI males (kg/m2) 26.54±4.15 28.00±4.32 −1.46 (−1.52-−1.39) <0.001
BMI females (kg/m2) 25.93±4.00 27.42±4.20 −1.49 (−1.55-−1.40) <0.001
*Two sided P values based on pair t-test, **Number of sleeping hours during Ramadan timing. BP=Blood pressure, SD=Standard deviation, BMI=Body mass index, 25-OH=25-hydroxy, HDL-C=High-density lipoprotein-cholesterol, LDL-C=Low density lipoprotein-cholesterol, SBP=Systolic blood pressure, DBP=Diastolic blood pressure, HbA1c=Glycated hemoglobin, CI=Confidence interval
HbA1c level, calcium, creatinine, albumin, total cholesterol,
HDL-C, LDL-C, uric acid, systolic and DBP, hours of sleep,
and BMI before and after Ramadan (P < 0.001 for each).
Table 4 shows the results of multiple linear regression
analysis to indicate predictors and impact of Ramadan fasting
on several biochemical and lifestyle parameters in diabetic
patients. As can be seen from this table, HbA1c (P < 0.001),
physical activity (P < 0.001), hours of sleeping (P < 0.001),
systolic BP (mmHg) (P = 0.007), obesity (P = 0.016),
diastolic BP (mmHg) (P = 0.018), family history (P = 0.021),
and smoking (P = 0.045) were significantly associated with
Ramadan fasting as contributing factors.
d
IscussIon
In Turkey, a large proportion of patients with diabetes
mellitus fast regularly during Ramadan. Ramadan fasting is
a challenge for diabetic patients because of the acute changes
in their dietary and lifestyle patterns. Therefore, it is difficult
to suggest a treatment for this group of people. The number
of studies on Ramadan fasting T2DM patients from Turkey is
limited and has been restricted to using few patients, with the
largest study using 122 patients.
[5]In this context, the current
study is much larger as it recruited 1246 T2DM patients. The
present study, with a much larger number of patients, revealed
the favorable impact of Ramadan fasting on the important
parameters of diabetes including blood glucose, HbA1c levels,
and lipid profile. The results are consistent with previous
studies reported in the literature.
[1,4-7,12-15,19-24]In patients with
T2DM, diet, exercise, and antidiabetic medications can help
stabilize blood glucose level. However, any alteration can
fluctuate the blood glucose level and lead to hyperglycemia
or hypoglycemia.
[1,14,16]A previous small study (n = 122)
investigated Turkish patients with T2DM before and after
Ramadan. It did not find any negative effects of fasting on
this group of patients.
[5]This is in agreement with our much
larger study (1246 T2DM patients). Therefore, the current
evidence suggests that Ramadan fasting is unlikely to be risky
for well-controlled patients.
[1,2,16,20-24]According to previous
studies, Ramadan fasting had no negative impacts on glucose
regulation of patients with T2DM who use antidiabetic
medications.
[5-7,12-14,20-24]This is in good agreement with our
study. The findings from our study revealed that fasting leads to
a statistically significant reduction in blood glucose levels that
were consistent with other studies.
[5-6,13]It has been previously
reported that weight loss is important for improving the health
status of T2DM patients.
[25]For example, weight loss has been
found to be a stronger predictor of HbA1c goal attainment in
T2DM compared to medication adherence.
[26]The finding of
this study revealed that after the month of Ramadan fasting
there is a significant decrease in body weight which could
beneficial for T2DM patients and Ramadan fasting could play
a role in diabetes therapy. There is now consensus that physical
activity can be beneficial for diabetes as it can improve various
risk factors associated with diabetes including blood glucose
level.
[27]The study reveals that compared to before Ramadan,
there is a statistically significant increase in physical activity
after Ramadan. The precise reason for this change is not clear,
but the reduction in body weight and the improvement in blood
parameters may have some contributory roles. In addition
to improvements in blood parameters, Ramadan fasting led
to a statistically significant increase in the duration of sleep
compared to before Ramadan. This is important since there is
insufficient sleep duration is associated with a poor glycemic
control in T2DM.
[28]In a comprehensive study,
[29]several suggestions have been
recommended for patients with diabetes mellitus.
[29]The
suggestions were blood glucose monitoring, consultation with
their physicians, not skipping predawn meal, not doing tiring
exercises, and regulation of medication dose. Monitoring
plasma glucose during Ramadan fasting is a difficult issue
for doctors and patients.
[2]The plasma glucose levels are
determined by food intake, physical activity, and medications.
Patients with T2DM should be recommended to monitor blood
glucose regularly throughout the fasting month.
[12]c
onclusIon
The current study represents the largest study (n = 1246) with
Turkish T2DM patients to explore the impact of Ramadan
fasting on different biochemical and lifestyle parameters.
We found significant differences between Ramadan fasting
and decrease in blood lipid profile, blood pressure, blood
glucose, HbA1c levels, BMI, and sleeping problems among
patients with T2DM. The study suggests that Muslim diabetic
patients can fast during Ramadan after consultation with their
physicians. Indeed, Ramadan fasting can be considered as a
strategy for managing and improving the health of diabetic
patients.
Acknowledgment
This work was generously supported and funded by the
Qatar Diabetes Association, Qatar Foundation. The authors
would like to thank the Cerrahpaşa Faculty of Medicine and
Medipol International School of Medicine, Istanbul Medipol
University for their support and ethical approval (RP#
10840098-604.01-E.3192).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
r
eferences
1. Khan N, Khan MH, Shaikh MZ, Khanani MR, Rasheed A. Effects of Ramadan fasting and physical activity on glucose levels and serum lipid profile among type 2 diabetic patients. Pak J Med Sci 2012;28:91-6. 2. Salti I, Bénard E, Detournay B, Bianchi-Biscay M, Le Brigand C,
Voinet C, et al. A population-based study of diabetes and its characteristics during the fasting month of ramadan in 13 countries: Results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004;27:2306-11.
A population-based study in Qatar. J Egypt Public Health Assoc 2014;89:47-52.
4. Lamri-Senhadji MY, El Kebir B, Belleville J, Bouchenak M. Assessment of dietary consumption and time-course of changes in serum lipids and lipoproteins before, during and after Ramadan in young Algerian adults. Singapore Med J 2009;50:288-94.
5. Sahin SB, Ayaz T, Ozyurt N, Ilkkilic K, Kirvar A, Sezgin H, et al. The impact of fasting during Ramadan on the glycemic control of patients with type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes 2013;121:531-4.
6. Karatoprak C, Yolbas S, Cakirca M, Cinar A, Zorlu M, Kiskac M, et al. The effects of long term fasting in Ramadan on glucose regulation in type 2 diabetes mellitus. Eur Rev Med Pharmacol Sci 2013;17:2512-6. 7. Chentli F, Azzoug S, Amani Mel A, Elgradechi A. Diabetes mellitus and
Ramadan in Algeria. Indian J Endocrinol Metab 2013;17:S295-8. 8. Khan N, Rasheed A, Ahmed H, Aslam F, Kanwal F. Effect of Ramadan
fasting on glucose level, lipid profile, hbA1c and uric acid among medical students in Karachi, Pakistan. East Mediterr Health J 2017;23:274-9. 9. Al Suwaidi J, Bener A, Hajar HA, Numan MT. Does hospitalization
for congestive heart failure occur more frequently in Ramadan: A population-based study (1991-2001). Int J Cardiol 2004;96:217-21. 10. Al Suwaidi J, Bener A, Gehani AA, Behair S, Al Mohanadi D, Salam A,
et al. Does the circadian pattern for acute cardiac events presentation
vary with fasting? J Postgrad Med 2006;52:30-3.
11. Bener A, Azhar A, Bessisso M. Do fasting and life style eating habits in Ramadan affect headache? Nutr Food Sci 2007;37:427-33.
12. Bener A, Galadari S, Gillett M, Osman N, Al Taneji H, Al-Kuwaiti MH,
et al. Fasting during the holy month of Ramadan does not change the
composition of breast milk. Nutr Res 2001;21:859-64.
13. Ismail NA, Olaide Raji H, Abd Wahab N, Mustafa N, Kamaruddin NA, Abdul Jamil M, et al. Glycemic control among pregnant diabetic women on insulin who fasted during Ramadan. Iran J Med Sci 2011;36:254-9. 14. Velayudhan M. Managing diabetes during the Muslim fasting month of
Ramadan. Med J Malaysia 2012;67:353-4.
15. World Health Organization. The Prevention of Diabetes and its Complications, WHO Report; 2006. Available from: http://www.who. int/diabetes/preventionflyer/en/. [Last accessed on 2017 Sep 04]. 16. Bener A, Keskin FE, Kurtulus EM, Guzel M, Çekirdekçi EI, Kadıoğlu
P, Konukoğlu D, Öztürk M. Essential parameters and risk factors of the patients for diabetes care and treatment. Diabetes Metab Syndr. 2017;11 Suppl 1:S315-20. Doi: 10.1016/j.dsx.2017.03.008.
17. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and
classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 1998;15:539-53.
18. Sözmen K, Unal B, Capewell S, Critchley J, O’Flaherty M. Estimating diabetes prevalence in turkey in 2025 with and without possible interventions to reduce obesity and smoking prevalence, using a modelling approach. Int J Public Health 2015;60 Suppl 1:S13-21. 19. National Cholesterol Education Program (NCEP) Expert Panel on
Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult treatment panel III) final report. Circulation 2002;106:3143-421. 20. Katibi IA, Akande AA, Bojuwoye BJ, Okesina AB. Blood sugar control
among fasting muslims with type 2 diabetes mellitus in Ilorin. Niger J Med 2001;10:132-4.
21. Khatib FA, Shafagoj YA. Metabolic alterations as a result of Ramadan fasting in non-insulin-dependent diabetes mellitus patients in relation to food intake. Saudi Med J 2004;25:1858-63.
22. Rehman J, Shafiq M. Changes in blood glucose and lipid profile during Ramdan fasting. JAMC 2000;12:13-5.
23. Al Suwaidi J, Bener A, Suliman A, Hajar R, Salam AM, Numan MT,
et al. A population based study of Ramadan fasting and acute coronary
syndromes. Heart 2004;90:695-6.
24. Bener A, Hamad A, Fares A, Al-Sayed HM, Al-Suwaidi J. Is there any effect of Ramadan fasting on stroke incidence? Singapore Med J 2006;47:404-8.
25. Anderson JW, Kendall CW, Jenkins DJ. Importance of weight management in type 2 diabetes: Review with meta-analysis of clinical studies. J Am Coll Nutr 2003;22:331-9.
26. McAdam-Marx C, Bellows BK, Unni S, Mukherjee J, Wygant G, Iloeje U, et al. Determinants of glycaemic control in a practice setting: The role of weight loss and treatment adherence (The DELTA study). Int J Clin Pract 2014;68:1309-17.
27. Colberg SR, Sigal RJ, Fernhall B, Regensteiner JG, Blissmer BJ, Rubin RR, et al. Exercise and type 2 diabetes: The American college of sports medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010;33:e147-67.
28. Lee SWH, Ng KY, Chin WK. The impact of sleep amount and sleep quality on glycemic control in type 2 diabetes: A systematic review and meta-analysis. Sleep Med Rev 2017;31:91-101.
29. Ibrahim M, Abu Al Magd M, Annabi FA, Assaad-Khalil S, Ba-Essa EM, Fahdil I, et al. Recommendations for management of diabetes during Ramadan: Update 2015. BMJ Open Diabetes Res Care 2015;3:e000108.