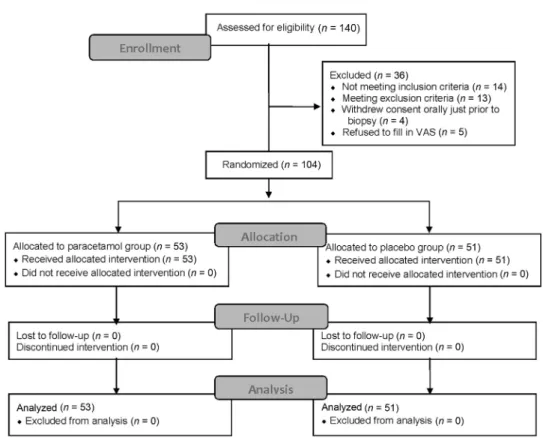
Intravenous paracetamol for relief of pain during transrectal-ultrasound-guided biopsy of the prostate A prospective, randomized, double-blind, placebo-controlled study
Tam metin
Şekil
Benzer Belgeler
Bu doğrultuda şu araştırma sorularının cevabı aranmıştır: (1)Kurumsal Yönetim Endeksi’nde yer alan şirketlerin Halkla İlişkiler departmanları özerk midir?,
“Türk sinemasında kadın karakterlerin giyim tarzlarında kültürel anlamlar” başlıklı bu çalışmada; Türk sinemasının melodram filmlerinde, film ile seyirci
Bu çalışma, bu tür bir sorgulayıcı yaklaşımla, Türkiye’de katılımcı gazeteciliğin mevcut durumunu ele alıp değerlendirmekte ve bu amaçla çevrimiçi profesyonel
Marmara Üniversitesi Ekonomik ve Sosyal Alanda Kad›n Çal›flmalar› Uygulama ve Araflt›rma Merkezi 2016 Mimar Sinan Güzel Sanatlar Üniversitesi Kad›n
Kadına yönelik aile içi şiddet genel olarak her türlü toplum ve statüde görülebilmesine rağmen, sosyoekonomik ve eğitim düzeyi düşük olan, evlilik sorunları
Giriş kısmında Türk âşık geleneği ve âşık muhitleri hakkında, Âşık Şenlik’in bu gelenekteki yeri üzerine bir değerlendirme yapılmış, aynı zamanda
Türkiye Türkçesinden seslenme sözlerine dair verilerin tasnifinde Özezen’in (2004) yapmıĢ olduğu tasnif dikkate alınmıĢtır. Ancak elde edilen bulgulara göre
Osmanlı şiirinde ģāżır bāş ve ģāżır-bāş ol- biçiminde kullanılan kalıp söz, kaynaklarda belirtildiği gibi ‘hazır ol, dikkatli ol, tetikte ol, tedbiri
