www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Computed
tomography
based
analysis
of
the
lamina
papyracea
variations
and
morphology
of
the
orbit
concerning
endoscopic
surgical
approaches
夽
Gülay
Ac
¸ar
a,∗,
Mustafa
Büyükmumcu
a, ˙Ibrahim
Güler
baNecmettinErbakanUniversity,MeramFacultyofMedicine,DepartmentofAnatomy,Konya,Turkey bSelcukUniversity,FacultyofMedicine,DepartmentofRadiology,Konya,Turkey
Received5March2018;accepted17April2018 Availableonline18May2018
KEYWORDS Computed tomography; Endoscopicapproach; Laminapapyracea; Orbitalmorphometry; Reconstructive surgery Abstract
Introduction:Radiologic evaluationismandatorytoassessthetype ofendoscopicapproach concerningsinonasalpathologyandreconstructionoffractureddefectsbeforeanytreatment modalitiesareinstitutedrelatedtomedialwalloftheorbit.
Objective: Thegoalwastoprovideimprovedunderstandingofthelaminapapyraceavariations andtherelationshipwiththeorbitalmorphometry.
Methods:This retrospectivestudy was performedusing computedtomography scansof200 orbitsandresultswerecomparedwithrespecttoage,sex,lateralityandLPvariations.
Results:LaminapapyraceavariationswerecategorizedastypeA,80.5%(161/200);typeB,16% (32/200);typeC,3.5%(7/200).Formedialwalltheanteriorandposteriorlaminapapyracea heightsandangleswerefoundas17.14mm,147.88◦ and9.6mm,152.72◦,respectively.Also, the length ofthe lamina papyracea, themean area ofthe orbital floor,medial wall, lam-inapapyraceaandorbitalentrancewere33.3mm,7.2cm2,6.89cm2,4.51cm2and12.46cm2
respectively. The orbitalheightandwidth weremeasured as35.9mmand39.2mm respec-tively.Themeanorbitalcavitydepthwas46.3mmfromopticforamentotheorbitalentrance andtheorbitalvolumewas19.29cm3.Weanalyzedthemorphometricmeasurementstending
toincreasewithagingandgreaterinmenandtherelationshipofthemwithlaminapapyracea types.
夽 Pleasecitethisarticleas:Ac¸arG,BüyükmumcuM,Güler ˙I.Computedtomographybasedanalysisofthelaminapapyraceavariationsand morphologyoftheorbitconcerningendoscopicsurgicalapproaches.BrazJOtorhinolaryngol.2019;85:551---9.
∗Correspondingauthor.
E-mail:[email protected](G.Ac¸ar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.
https://doi.org/10.1016/j.bjorl.2018.04.008
1808-8694/©2019Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
Conclusion:Preciseknowledgeofthelaminapapyraceaanatomyusingcomputedtomography isessentialforsaferandmoreeffectivesurgeryandpreformingthedimensionsofanimplant. Inthisway,thepostoperativecomplicationscanbedecreasedandthebestoutcomecanbe provided.
© 2019 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/). PALAVRAS-CHAVE Tomografia computadorizada; Abordagem endoscópica; Laminapapirácea; Morfometriaorbital; Cirurgia reconstrutora
Análisetomográficadasvariac¸õesdalâminapapiráceaedamorfologiaorbitalem abordagenscirúrgicasendoscópicas
Resumo
Introduc¸ão: Aavaliac¸ãoradiológicaémandatóriaparaavaliarotipodeabordagemendoscópica notratamentocirúrgicodedoenc¸anasossinusalenareconstruc¸ãodefraturasantesdequaisquer modalidadesdetratamentorelacionadasàparedemedialorbital.
Objetivo:O objetivo foi proporcionar uma melhor compreensão das variac¸ões da lâmina papiráceaearelac¸ãocomamorfometriaorbital.
Método: Este estudo retrospectivo foi realizado por meio de tomografia computadorizada de200órbitas, eosresultadosforamcomparados emrelac¸ão àidade, sexo,lateralidadee variac¸õesdalâminapairácea.
Resultados: As variac¸ões da lâmina papirácea foram categorizadas como tipo A, 80,5% (161/200);tipoB,16%(32/200);tipoC,3,5%(7/200).Paraaparedemedial,asmedidasdas alturasanterioreseposterioresdalâminapapiráceaeângulosforamde17,14mm,147,88◦e 9,6mm,152,72◦,respectivamente.Alémdisso,asmedidasdoseucomprimentoda,daárea médiado assoalhoorbital,e daparedemedial,lâmina papyraceae entradaorbital foram: 33,3mm, 7,2cm2, 6,89cm2, 4,51cm2 e 12,46cm2, respectivamente. As medidas da altura
edalarguraorbitaisforam35,9mme39,2mm,respectivamente.Aprofundidademédiada cavidadeorbitalfoide46,3mm,doforameópticoatéaentradaorbital,eovolumeorbital foi de 19,29cm3.Analisamos as medidas morfométricas com tendência a aumentar como
envelhecimento enos indivíduos dosexo masculino, ea relac¸ão dasmesmas com ostipos delâmina.
Conclusões:Oconhecimentoprecisodaanatomiadalâminapapiráceapormeiodetomografia computadorizada éessencialpara umacirurgia maissegura eeficaz,alémdepermitir pré-moldaras dimensõesdo implante.Assim,as complicac¸õespós-operatórias podem ser mini-mizadas,obtendo-semelhoresresultados.
© 2019 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
The lamina papyracea (LP) is the weakest point of the medial wall of the orbit, which forms a connecting line between paranasal sinuses and the orbit. Also, the eth-moidal foramina along the LP are life-saving anatomical landmarksand allow transverse passage of the ethmoidal arteriesintoethmoidalcells.1Duringsurgicalinterventions
suchasreconstructionandendoscopicapproaches,success insurgicalstrategyandplanningmainlyrelyonthesurgeon’s detailedknowledgeoftheLPvariationsandthelocationof ethmoidalforamina,providing a shortersurgery timeand avoidanceofcomplications.2---4
During endoscopic sinus surgery (ESS) which is essen-tialforthetreatmentofchronicrhinosinusitisandremoval of the sinonasal pathologies, accidental LP injury can be incurred.4,5PreciseknowledgeofLPlocalizationaccording
toinferiornasalturbinate (INT)attachmenttothelateral nasal wall is essential to avoid orbital penetration.4 As a
consequence of LP penetration, periorbital ecchymosisor emphysema,venousorbitalhematoma,medialrectusinjury, andblindnesscanoccur.Also,revisionESScanberequired forresidualunopenedethmoidcellsattheLPdueto insuffi-cientknowledgeoftheradiologicalandendoscopicsinonasal anatomy.4,6
Ontheother hand,reconstructionisindicated incases of visual acuity, diplopia withextraocular muscle entrap-ment, large bony defects, enophthalmos and cosmetic complications.7,8Theinferomedialstrut(IMS),theanterior
(AEF)andposteriorethmoidal(PEF)foraminaidentifiedon CT coronal plane are important surgical landmarks for a combinedrepair of orbitalbony defects.1,9 The combined
orbital fractures involving the IMS represent an applica-tiondifficultyofimplantmaterialinreconstructionsurgery.
In addition, an adequate surgical exposure and access as well as an implant with proper size and shape is essen-tial to insure the success of surgical technique.10,11 Also,
thelackofmalleabilityofthickimplants,theclose proxim-ityoftheimplanttovitalorbitalstructures,andincorrect estimationofthedimensionsoftheimplantcancause sig-nificantpostoperativecomplicationssuchasenophthalmos, opticneuropathysecondarytoimplantimpingement,orbital emphysemaandhemorrhage.7,10,11
By using multiplanar reconstruction (MPR) detailed knowledge of the normal anatomy of the bony orbit and relationship with the surrounding structures can be acquired.12,13 Radiologic description of the size and
mor-phologyofthemedialwalloftheorbitonCTscanisessential toguidethesurgeonindiagnosis,decidingtheproper sur-gicalapproachandoutcomeprediction.13
Inthisstudy,wefocusedontheLPvariationsandorbital medialwallmorphometryfromthepointofviewof endo-scopic sinus surgery and reconstruction of fractures. To understandthemedialwalloftheorbitprecisely,we mea-suredasetofangularandlinearparametersbyusingfacial MPRimages.Inparticular, weanalyzedtherelationshipof thesemorphometricparameterswithLPvariations.TheCT scan analysis of these parameters may be helpful to the surgeon in preoperative planning and avoiding accidental penetrationoftheLP.
Methods
This retrospective study wasapprovedby ourlocal Ethics Committee with an approval number 2016/539 and per-formed using facial (orbital and paranasal) CT images of 100patients,rangingfrom18to90yearsofage,who pre-sentedtotheDepartmentofRadiologyforclinicalpurposes betweenSeptember2015andJuly2016.Thepatientswho hadorbitalfractures,paranasalsinuseswithanydistorting pathologieswhichdamagedtheorbitalbonycontours, con-genitaldeformitiesandGravesorbitopathywereexcluded. All patientswere evaluatedusing128 slice CTscanner (Siemens,imagingparameters:Kv=120;mA=160;rotation time, 0.5s; collimation, 128×0.625; FOV=220mm). MPR images(associatedcoronalandsagittalimagesof1mmslice thickness)weregeneratedonthebasisoftheaxialimages whichwereobtainedwithasectionthickeningof0.625mm. AccordingtoapredesignedprotocolonSyngoVia(Siemens, Germany)theCTimageswerereconstructedandanalyzed by thetwoinvestigators(a radiologist andan anatomist). Also,all results werecheckedfor accuracy bythem. The
Table 1 Definitions of measurements of the orbital morphometry.
Definitions Orbitalentrance
height
Thedistancefromtheinfraorbital canaltosuperiororbitalrim Orbitalentrance
width
Thedistancefromthe
frontoethmoidalsuturetomidpoint ofthelateralrim
Orbitalcavity depth
Thedistancefromtheorbital foramentotheplanepassingacross theorbitalentrance
Orbitalentrance area
Theareaofanoctagonalpolygon whichisformedbyanatomical landmarks;supraorbitalforamen, frontoethmoidalsuture,infraorbital foramen,zygomaticofrontalsuture andmidpointsbetweenthem Orbitalfloorarea Thetriangularareafromtheorbital
foramentotheplanepassingacross theorbitalentrance
Orbitalmedial wallarea
Thetriangularareafromtheorbital foramentotheplanepassingacross theorbitalentrance
Anteriororbital medialwallheight andinferiomedial angle
ThedistancefromtheAEFtothe ethmoidomaxillarysutureand inferomedialanglebetweenthe orbitalmedialandinferiorwalls Posteriororbital
medialwallheight andinferiomedial angle
ThedistancefromtheAEFtothe ethmoidomaxillarysutureand inferomedialanglebetweenthe orbitalmedialandinferiorwalls Laminapapyracea
length
Thedistancefromtheposterior lacrimalcresttojunctionpoint betweensphenoidandethmoid sinuses
patientsconsistedof23females(43%)and77males(57%) witha medianage of48.60±12.32 yearsfor femalesand 37.36±15.24yearsformales.Wedividedthepatientsinto 3agegroups:Group 1(18---39y)including94orbits,Group 2 (40---59y) including78 orbits; Group 3 (60---90y) includ-ing28orbits. We describedthe anatomiclandmarksusing measurementsinTable1.
WedeterminedtheAEFandPEF,andmeasuredthelength oftheLPbetweentheminanaxialplane(Fig.1A).Then, in coronal plane we measured the anterior and posterior
Figure1 (A)Axialimageidentifyingthelocationoftheanterior(AEF)andposteriorethmoidalforamen(PEF)showsthe mea-surementoflaminapapyracealength(LPlength);(B)coronalimageshowstheanteriorlaminapapyraceaheight(LPheight)fromthe
anteriorethmoidalforamentotheethmoidomaxillarysuture(EMS)andtheanteriorinferomedialangle(arrow)betweenmedial andinferiorwallstheorbit.
Figure2 Coronalimageshows the posteriorlamina papyraceaheight(LPheight)fromtheposterior ethmoidal foramentothe
ethmoidomaxillarysuture(EMS)andtheposteriorinferomedialangle(arrow)betweenmedialandinferiorwallstheorbit.
Figure3 Coronalimageshowsthelaminapapyraceavariationsrelatedwithinferiornasalturbinateattachment(whitevertical axis)tothelateralnasalwall.TypeA(whitethindottedaxis);locatedwithin2mmoneithersideoftheverticalaxis;TypeB(white thickdottedaxis);medialtoaxisby>2mm;TypeC(blackthickdottedaxis);lateraltoaxisby>2mm.
LPheightsasadistancefromtheAEF andPEFtotheIMS, whichwasthejunctionbetweentheorbitalmedialwalland floor.Also,the anteriorandposterior inferomedialangles attheIMSweremeasured(Figs.1Band2).Conversely,we accepted the LP as a trapezoid and calculated the area oftheLPby usingtheformula;LPlength/2×(anteriorLP height+posterior LP height). Also,we analyzed the types oftheLPpositionrelatedwithINTattachmenttothe lat-eralnasalwall(Fig.3).Theverticalaxiswaslocatedonthe INTattachmentinthecoronalplane.WecategorizedtheLP intothreetypesasfollows,whichwerebasedonHerzallah etal.’s4classificationoftheLPtype:
TypeA,locatedwithin2mmoneithersideofthevertical axis;
TypeB,medialtoaxisby>2mm; TypeC,lateraltoaxisby>2mm.
The intersectionof‘x’and‘y’axeswaslocated atthe orbital foramen (OF) and the vertical axis passed along themedialrectus muscle inthe axialplane (Fig.4A).We measured the area of the medial wall at this position in sagittalplane(Fig.4B). Then,theintersectionoftheaxes
waslocatedattheOFandthehorizontalaxispassedalong inferior rectus muscle in the sagittal plane (Fig. 5A). We measuredtheareaoftheinferiorwallatthispositioninthe axialplane(Fig.5B).
Inaddition,weaimedtodescribethemorphometryand geometry ofthe orbitfromthe pointof viewof an endo-scopic reconstructive surgery and to provide a detailed knowledge about the size and shape of the implant. We formed an octagonal polygon on orbital rims by specify-ing 8 anatomic landmarks and measured the area of the orbitalentrance(OE). Theseorbitalrim landmarks, which were visually identifiable and similar to the morphomet-ric parameters in previous studies included; supraorbital foramen superiorly, the frontoethmoidal suture medially, infraorbitalforameninferiorly,thezygomaticofrontalsuture laterallyandmidpointsbetween them(Fig.6A).Also,the vertical measurement between the infraorbital canal and superiororbitalrim,andthehorizontalmeasurementfrom the frontoethmoidalsuture tomidpointof thelateral rim weretakenasanOEheightandwidth,respectively(Fig.6A). Ontheotherhand,theopticnervewasviewedas uninter-ruptedintheaxialplaneandthedepthoftheorbitalcavity fromtheOFtotheplanepassingacrosstheOEwasmeasured
Figure4 (A)Axialimageshowsidentificationoftheorbitalforamen(OF)andmedialrectusmuscle(MR).(B)Themeasurement oftheareaofthemedialwallinsagittalplaneofaxialposition.
Figure5 (A)Sagittalimageshowsidentificationoftheorbitalforamen(OF)andinferiorrectusmuscle(IR).(B)Themeasurement oftheareaoforbitalfloorinaxialplaneofsagittalposition.
Figure6 MultiplanarreconstructionoftheCTimagesshowingthemorphometricmeasurementsregardingorbitalentranceand orbitaldepth.(A)The orbitalrim landmarkswereidentifiedonoctagonal polygonshaped orbitalentranceincoronalplane: 1 supraorbitalforamen,3frontoethmoidalsutureand2midpointbetweenthem,4ethmoidomaxillarysuture,5infraorbitalforamen, 7zygomaticofrontalsutureand6midpointbetweenthem,8midpointbetweenzygomaticofrontalsutureandsupraorbitalforamen. The areaofthisoctagonal polygonwas measuredasorbital entrancearea.Orbitalentranceheight(OEheight)frominfraorbital
foramentomidpointofthesuperiororbitalrimandorbitalentrancewidth(OEwidth)fromfrontoethmoidalsuturetomidpointof
thelateralorbitalrim.(B)Orbitaldepthwastakenashorizontalmeasurementfromorbitalforamen(OF)toorbitalentrance.
(Fig.6B). Weassumed the orbitasan octagonal pyramid-shaped bony compartment and calculated the orbital volumebyusingtheformula;1/3×OEarea×orbitaldepth. Ontheotherhand,wecomparedthemeasurement val-ueswithrespecttoage,sex,lateralityandLPtypes.SPSS 22 (SPSS, Inc., Chicago, IL, USA) was used for statistical analysis.Forstatisticalcomparisons,Chi-squaretest,t-test,
One-WayAnalysisofVariance (ANOVA)wereused.The sig-nificancelevelwassetatp<0.05.
Results
Wemeasured themean lengthofthe LPas33.3±2.9mm and calculated the mean area of the trapezoid LP as 4.51±0.81cm2. The mean lengths of the anterior and
posterior LP height at the level of the AEF and PEF in the coronal scan were found as 17.4±2.7mm and 9.6±2.5mm, respectively. Also, the mean inferomedial angularmeasurements includingAEF and PEF levelswere 147.88◦±7.54◦ and152.72◦±9.61◦,respectively.We mea-suredthemeanvaluesofthemedialandinferiorwallareas as 7.20±0.6cm2 and 6.89±0.59cm2, respectively. Both
themeanOE height, widthand areameasurementvalues were 35.9±1.7mm, 39.2±2.0mm and 12.46±0.70cm2,
respectively. We reported the mean values of orbital depthand volumeas46.3±2.2mm and 19.29±1.61cm3,
respectively.Allmorphometricmeasurementvaluesshowed significantdifferenceswithrespecttosexandageasseen inTables 2 and 3,although therewasno statistically sig-nificantdifferenceamongright andleftsides. In Table2, wedemonstratedthatallmeasurementvalueswerehigher
Table2 Thedistributionofthecomparisoninmorphometricmeasurementsbetweenfemalesandmales.
Morphometricmeasurements Female Male Total
Mean±SD Mean±SD Mean±SD
Orbitalentranceheight(mm) 35.0±1.3b 36.2±1.8b 35.9±1.7
Orbitalentrancewidth(mm) 38.5±1.6a 39.4±2.1a 39.2±2.0
Orbitalentrancearea(mm2) 1205±66b 1258±67b 1246±70
Orbitalcavitydepth(mm) 45.5±2.4a 46.5±2.0a 46.3±2.2
Orbitalvolume(mm3) 1878±167b 1997±150b 1929±161
Orbitalfloorarea(mm2) 659±57b 698±57b 689±59
Orbitalmedialwallarea(mm2) 688±56b 730±59b 720±60
Orbitalmedialwallheight(mm)
Anterior 16.2±3.4a 17.6±2.4a 17.4±2.7
Posterior 9.0±2.5a 9.8±2.4a 9.6±2.5
Orbitalinferiomedialangle(◦)
Anterior 147.82±8.45 147.89±7.28 147.88±7.54 Posterior 151.92±8.11 152.96±10.02 152.72±9.61
Laminapapyracealength(mm) 32.5±2.9a 33.5±2.9a 33.3±2.9
Laminapapyraceaarea(mm2) 418±75a 460±81a 451±81
Mean±SD(standarddeviation). Unpairedt-test.
ap<0.05. b p<0.001.
Table3 Comparisonsofthemorphometricmeasurementsamongthethreeagegroups.
Morphometricmeasurements Total 18---39y 40---59y 60---90y Orbitalentranceheight(mm) 35.9±1.7 35.3±3.0a 36.4±2.1a 36.1±0.6
Orbitalentrancewidth(mm) 39.2±2.0 38.8±2.3a 39.4±0.6a 39.0±0.4
Orbitalentrancearea(mm2) 1246±70 1185±11 1266±11 1254±20
Orbitalcavitydepth(mm) 46.3±2.2 45.7±1.2a 46.4±1.0a 46.2±0.3
Orbitalvolume(mm3) 1929±161 1851±13 1957±14 1933±20
Orbitalfloorarea(mm2) 689±59 673±10a 699±46a 686±64
Orbitalmedialwallarea(mm2) 720±60 689±39a 726±17a 710±48
Anterior 17.4±2.7 16.4±1.0a 17.7±1.2a 17.5±1.5
Posterior 9.6±2.5 9.5±3.3 10.1±0.3 9.8±0.7 Anterior 147.88±7.54 148.70±14.6 147.39±13.6 147.33±21.0 Posterior 152.72±9.61 152.88±3.70 152.56±10.3 152.45±3.81 Laminapapyracealength(mm) 33.3±2.9 33.7±3.5 33.5±3.5 33.0±2.6 Laminapapyraceaarea(mm2) 451±81 460±32 455±68 446±10
ANOVA(One-WayAnalysisofVariance).
ap<0.05.
inmalesthanfemalesandshowedstatisticallyasignificant differenceexceptfortheangularresults.Themeasurement resultsindicated thatsubjectsin thefirstandsecond age groupsshowedstatisticallysignificantdifferencesinorbital height,widthanddepth,medialandinferiorwallareasand anteriorLPheightasshowninTable3.
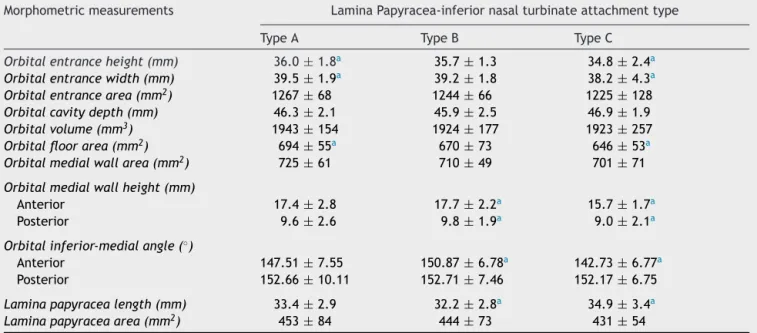
Thedistributionsof200LPtypeswerecategorizedas fol-lows;TypeA,80.5%(161/200);TypeB,16%(32/200);TypeC, 3.5%(7/200).Therewerenostatisticallysignificant differ-encesinprevalenceswithrespecttosex,ageandlaterality. Inaddition,weanalyzedtherelationshipbetween morpho-metricmeasurementsandLPtypes.AsseeninTable4,all meanvaluesexcepttheorbital depthandLP lengthwere smallestinTypeC,whereastheinferiorwallarea,anterior
and posterior LP heights, anteriorinferomedial angle and LPlengthvaluesshowedstatisticallysignificantdifferences betweenTypeBandC.
Discussion
The medial wall of the orbit contributes significantly to maintain orbital volume and the displaced or combined fracturesandperforationoftheLPresultinariskof enoph-thalmos.ThenotchesintheLP,whichcanbeidentifiedon coronalCTimageareagoodreferenceforthepositionand orientationoftheethmoidalarteries.1,10,14Fortheremoval
Table4 Therelationshipbetweenthemorphometricmeasurementsandthelaminapapyracealocationtypes. Morphometricmeasurements LaminaPapyracea-inferiornasalturbinateattachmenttype
TypeA TypeB TypeC
Orbitalentranceheight(mm) 36.0±1.8a 35.7±1.3 34.8±2.4a
Orbitalentrancewidth(mm) 39.5±1.9a 39.2±1.8 38.2±4.3a
Orbitalentrancearea(mm2) 1267±68 1244±66 1225±128
Orbitalcavitydepth(mm) 46.3±2.1 45.9±2.5 46.9±1.9
Orbitalvolume(mm3) 1943±154 1924±177 1923±257
Orbitalfloorarea(mm2) 694±55a 670±73 646±53a
Orbitalmedialwallarea(mm2) 725±61 710±49 701±71
Orbitalmedialwallheight(mm)
Anterior 17.4±2.8 17.7±2.2a 15.7±1.7a
Posterior 9.6±2.6 9.8±1.9a 9.0±2.1a
Orbitalinferior-medialangle(◦)
Anterior 147.51±7.55 150.87±6.78a 142.73±6.77a
Posterior 152.66±10.11 152.71±7.46 152.17±6.75
Laminapapyracealength(mm) 33.4±2.9 32.2±2.8a 34.9±3.4a
Laminapapyraceaarea(mm2) 453±84 444±73 431±54
TypeA,laminapapyracealocatedwithin≤2mmoneithersideoftheinferiornasalturbinateattachment;TypeB,medialtoinferior nasalturbinateattachmentby>2mm;TypeC,lateraltoinferiornasalturbinateattachmentby>2mm.
Mean±standarddeviation.
ANOVA(One-WayAnalysisofVariance).
a p<0.05.
normalorbitalanatomy,CTimagingistheprimarytechnique usingtoviewLPvariationsordehiscenceandtolocalizethe ethmoidaircellsandhypoplasticmaxillarysinus.4,8,14Also,
MPRallowsobservationof craniofacialbonesfromvarious anglesand anevaluation of thesinonasalpathologies and complexfractures withoverlapping fragments or minimal displacement.15,16RecognitionoftheCTappearanceofthe
normal LPanatomy allowsassessment of the goals ofESS and reconstructive surgeryincluding meticulous planning, the use of adjunctive surgical approaches, and efficient clearanceofethmoidaircellsontheLP,avoidingitsinjury andproperimplantdimensions.17Inradiologicalanatomical
studies of the anatomicallandmarkson orbitalwalls, the areaandvolumeoftheorbitalcavitywereanalyzedtoguide asurgeoninthechoiceanappropriateendoscopicapproach andtoavoidsurgicalcomplications.12,14,18,19
Many clinical problems including, nasal polyposis, hypoplastic maxillary sinus, uncinectomy, middle meatal antrostomy, severe epistaxis, orbital decompression and reconstructionmayrequireanendoscopicsurgicalapproach totheLP.2,4DuringESS,anunexpected penetrationof the
LP,which is locatedjust superiortothe maxillary antros-tomy, can cause orbital complications such as massive hemorrhage, orbital hematoma, blindness and optic neuropathy.4,5,14 Shigetaetal. reportedtheprevalenceof
theLPinjuryintheirprospectivestudyas5.8%.5Therewere
differentgradesofnasalpolyposisaffectingupto4%ofthe population,and also,largerpolyps representa riskfactor during ESS.6 Also,Gore et al.demonstrated that residual
ethmoidaircellsontheLPwereidentifiedin79%of revi-sionESS patients.20 So, radiologic identification of theLP
positionsfromtheperspectiveofendoscopicapproachcan beofgreathelpinefficientclearanceofethmoidaircells onthe LP andavoidanceof penetration.Also, itcan also
provideabaselineforfuturestudiestoidentifyLPvariations associatedwithhigherriskofinjuryorresidualdisease.4,6,14
In the literature, the prevalence of the pure medial orbital wallfractures washigher than floor fracturesand theratioof themaround 1.8:1.11,21 Althoughthe weakest
pointofthemedialwallistheLP,thebonyseptabetween thebullaeofethmoidpneumatizationwhichappear honey-combedshapesupportstheLPagainsttraumaforces.But, thecombinedorbitalwallfracturesmostlyoccuratIMSand cause the loss of internal bony support.1,11 Also,
recons-tructivesurgeonsmaybeconfrontedwithdifficultpatients suchasthoseinvolvingcomplexfractures:reconstructionof largedefectspresents challenges.The significant discrep-ancybetweentheimplantshapeandthenormalanatomic shapeoftheorbitalwallinfracturesincludingIMScanresult ininsufficientorbitalvolumereduction.7,10,21 Ontheother
hand,the AEF and PEFat thelevel of the frontoethmoid suture can serve asa vital anatomic reference toproper implantplacement.Asaresultofinaccuratereductionand reconstructionof theorbital walls, residualcomplications such as enophthalmos, diplopia, retrobulbar hemorrhage frominjury to the posterior ethmoidal artery and orbital emphysemacan beseen.7,10,11 Therefore,revisionsurgery
totreatthemisrequiredbeforeexcessscarringoccurs.To avoidthesecomplicationsitisnecessarytobeawareofthe linearandangularorbitalmorphometryincludingtheIMS.7
Becausethemedialwalloftheorbitcanbefracturedeasily andtheLPismostlyusedinendoscopicendonasalapproach, knowledgeofthe anatomicdimensionsof themedialwall increasesthe successrate ofsurgical techniqueand mini-mizestheiatrogeniccomplications.22
The AEF andPEF asanotch inthe medialorbital wall wereusedtoidentifythedimensionsoftheLP.Also,these parameters can be used in confirmation of the posterior
margin ofthe fracture, which iscritical toprevent resid-ual enophthalmos due to inadequate placement of the implant.10,11,21 Using CT scans Song et al. measured the
anterior and posterior heights of the LP, the length of theLP andLP areaas15.32mm,11.04mm,30.50mmand 4cm2.11Using3DCTimagesKangetal.reportedtheanterior
andposteriorheights oftheLPandinferomedialanglesas 17.73mm,12.76mm,132.118◦ and136.88◦,respectively.21
Inourstudy,themeanvaluesofthelength,area,anterior andposteriorheightsoftheLPandinferomedialangleswere 33.3±2.9mm, 451±81cm2, 17.4±2.7mm, 9.6±2.5mm,
147.8◦±7.54◦and152.72◦±9.61◦,respectively.All param-etersshowedatendency toincreasewithagingandwere greaterinmen,similartothefindingsofKangetal.Also, angularvaluesdidnotshow statisticallysignificant differ-enceswithrespecttosex,age,andlaterality.
The CT scan analysis of surface area of the floor and medialorbitalwallcanofferaccurateunderstandingofthe sizeof the surgical window for resectionor repair of the orbitaland sinonasalpathology. Inmany previous studies, abaselinevolumeofnormalbonyorbit,which isusefulin the prediction of enophthalmos, was measured and com-paredwithvolumetricchangesinthefracturedorbit.12,14,19
Feldingetal.measuredthevolumeandsurfaceareaofthe orbitalcavity as 24.27±3.88cm3 and 32.47±2.96cm2 by
usingunbiasedstereologicalsamplingtechnique.12 We
cal-culatedthemeanvolumeofan octagonalpyramid-shaped bonyorbitas19.29±1.61cm3.VanRompaeyetal.measured
theareaoftheorbitalfloorandmedialwallofretrobulbar spaceas4.33cm2and 3.34cm2by usingCTscans.14 Using
dryskulls,Fitzhughetal.foundtheareaoftheorbitalfloor andmedial wall as 7.14cm2 and 6.58cm2, respectively.19
Wemeasured their mean valuesas7.20cm2 and 6.89cm2
that were similar to Fitzhugh et al.’s. Also,these values werelargerinmalesthanfemales andshowedatendency toincreasewithagingasseeninTables2and3.
According to previous studies, there was a significant difference between the morphometric measurements of theorbital cavitywhich complicated toselect theproper size of repairing materials.7,8 The dimensions of
octago-nal shaped OE arean important factor for reconstructing the orbital rims and volume.19 Khademi et al., Ji et al.
and Fitzhugh et al. found the orbital width and height as 32.14mm, 33.35mm, 33.9mm and 28.49mm, 39mm, 38.7mm,respectively.18,19,23Inourstudy,thesevalueswere
found as 35.9mm and 39.2mm and larger in males than females,similartotheresultsinpreviousstudies.Jietal. measured the mean OE area as 11.80cm2 similar to our
value as 11.46cm2.23 Khademi et al.18 found the orbital
depthfrom OF tothe OE as38.84mm, but we measured itas46.3mm. WereportedthattheOE measurement val-ues were higher in male and increased significantly with age(p<0.05),althoughtherewasnostatisticallysignificant differencewithrespecttolaterality(Table3).
Duringendoscopicsinus surgery, the lowerlimit ofthe middlemeatalantrostomywastheinferiornasalturbinate attachmenttothelateralnasalwall.Ifpreoperativelythe LP location related to this limit can be identified, the LP penetration, which was the most frequent iatrogenic complication (5%) was prevented.4 So, we classified the
LPlocalizationconcerningendoscopicperspectiveand ana-lyzedtherelationshipwiththemorphometricmeasurements
inTable4.Also,El-Anwaretal.describedthepositionsof the LP in patients whohad nasal polypand reported the prevalence’sofTypeA,B,Cas60.6%,18.6%,21.3%.6Inour
study,we demonstratedthat the ratioof Type A,B, C in normalsinonasalanatomywas80.5%,16%,3.5%.Amedially locatedLP(TypeB)thattheleastresistanttosurgical inter-ventions can be easily penetrated during uncinectomy. A laterallylocatedLP(TypeC)requiresadequateclearanceof ethmoidaircellswhichcausestheLPpenetration.4El-Anwar
etal.found thatthepatientswhohadlargerpolypswere associated withsignificantly moreLP Type Bthan smaller polyp.6Inthisstudy,theorbitaldepthandLPlengthwere
foundasthelongestinTypeCandsmallestinTypeB.Both oftheanteriorandposteriormedialwallheightsand infer-omedialangleswerehighestinTypeB,smallestinTypeC. The meanvalues of the inferior wall area, orbital height and widthwere significantlylargerin TypeA thanType C (p<0.05).Also,theOEarea,orbitalvolumeandmedialwall areashowedamildtendencytoincreaseinTypeA.
Comparedwithprevious studies, ouroutcomesshowed little diversity depending on the differences in reference landmarks,methodologyandethnicities.Ontheotherhand, usingMPRimageswemeasuredsomeparameterswhichwere notusedinpreviousstudiessuchasanareaoftheOEwhich wasresembled theoctagonal polygonin shape,the ante-riorand posterior inferomedialangles, which wereuseful forreconstructivesurgery.Alsoweanalyzedtherelationship between theLP variations andthesemeasurement values concerningESS.Thus,thecomparativedatawasdeficient. Nevertheless,thehighernumberofpatientsandfuture stud-ies includingmeasurements in children and patients with orbitalfracturesmaygiveresearchersmorecomprehensive results.
Conclusion
Inthisstudy,we evaluatedLP variations,theorbital mor-phometry and analyzed the relationship between them concerningendoscopicsurgeryinallrespects. Asaresult, theLPvariationscanaltertheorbitalgeometryandplaya keyrolewhenchoosinganappropriatesurgicalapproachto avoid LPinjury.These resultsagain emphasizedthe value ofpreoperativeCTimagingwhichcanofferaccurate under-standingtheregionalanatomyofandaroundthebonyorbit. Thecomprehensiveknowledgeofthenormalanatomyofthe LPallowssaferandmoreeffectivesinussurgeryandis essen-tialforsufficientorbitalreconstructionwithproperimplant, andalsorecreationofnaturalslopeattheIMS.So,the suc-cessofsurgicaltechniqueincreasesandthebestoutcome canbeprovided.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ShermanD,LemkeB.Orbitalanatomyanditsclinical applica-tions.Duane’sClinOphthalmol.1992;2:13---20.
2.CelikS,OzerMA,KazakZ,GovsaF.Computer-assistedanalysis ofanatomicalrelationshipsoftheethmoidalforaminaandoptic
canalalongthemedialorbitalwall.EurArchOtorhinolaryngol. 2015;272:3483---90.
3.ParkJ,KimJ,LeeJ,ChangM,LeeH,ParkM,etal.Secondary reconstructionof residual enophthalmosusing anendoscope andconsideringtheorbitalfloorandmedialwallslope.J Cran-iofacSurg.2016;27:992---5.
4.Herzallah IR, Marglani OA, Shaikh AM. Variations of lamina papyracea position from the endoscopic view: a retrospec-tivecomputedtomographyanalysis.IntForumAllergyRhinol. 2015;5:263---70.
5.Shigeta Y, Okushi T, Yoshikawa M. Endoscopic sinus surgery complicationsaprospectivemulticenterstudy.NihonJibiinkoka GakkaiKaiho.2012;115:22---8.
6.El-Anwar MW, Khazbak AO, Eldib DB, Algazzar HY. Lamina papyraceaposition inpatientswithnasalpolypi:acomputed tomographyanalysis.AurisNasusLarynx.2018;45:487---91.
7.Cho RI, Davies BW. Combined orbital floor and medial wall fractures involving the inferomedial strut: repair technique andcaseseriesusingpreshapedporouspolyethylene/titanium implants.CraniomaxillofacTraumaReconstr.2013;6:161---70.
8.MiloroM,GhaliGE,LarsenP,WaiteP.Peterson’sprinciplesof oralandmaxillofacialsurgery.BCDecker.2004;1:168---82.
9.Lee JE, Lee JJ, Lee SU, Nam KY, Kwon JH, Park JH, etal.Ct-basedmorphologicalanalysisofisolatedinferiorand medial blow-out orbital fractures in Korean adults. Orbit. 2015;34:303---8.
10.Reiter MJ, Schwope RB, Theler JM. Postoperative ct of the orbital skeleton after trauma: review of normal appear-ances and common complications. AJR Am J Roentgenol. 2016;206:1276---85.
11.SongWK,LewH,YoonJS,OhMJ,LeeSY.Roleofmedialorbital wallmorphologicpropertiesinorbitalblow-outfractures. Inves-tigOphthalmolVisSci.2009;50:495---9.
12.FeldingUA,BlochSL,BuchwaldC.Thedimensionsoftheorbital cavitybasedonhigh-resolutioncomputedtomographyofhuman cadavers.JCraniofacSurg.2016;27:1090---3.
13.Lethaus B,WeiglS,Kloss-BrandstatterA, KlossFR,KesslerP, HolzleF,etal.Lookingforlandmarksinmedialorbitaltrauma surgery.IntJOralMaxillofacSurg.2013;42:209---13.
14.VanRompaeyJ,BushC,SolaresCA.Anatomicanalysisspecific fortheendoscopicapproachtotheinferior,medialandlateral orbit.Orbit.2014;33:115---23.
15.JosephJM,IPG.Orbitalfractures:areview.ClinOphthalmol. 2011;5:95---100.
16.CaranciF,CicalaD,CappabiancaS,BrigantiF,BruneseL,Fonio P.Orbitalfractures:roleofimaging.SeminUltrasoundCTMR. 2012;33:385---91.
17.SantosDT,OliveiraJX,VannierMW,CavalcantiMG.Computed tomographyimagingstrategiesandperspectivesinorbital frac-tures.JApplOralSci.2007;15:135---9.
18.KhademiZ,BayatP.Computedtomographicmeasurementsof orbitalentrancedimensionsinrelationto ageandgenderin a sample of healthy Iranian population. J Curr Ophthalmol. 2016;28:81---4.
19.Fitzhugh A, Naveed H, Davagnanam I, Messiha A. Proposed three-dimensionalmodeloftheorbitandrelevancetoorbital fracturerepair.SurgRadiolAnat.2016;38:557---61.
20.Gore MR, Ebert CS Jr, Zanation AM, Senior BA. Beyond the ‘‘centralsinus’’:radiographicfindingsinpatientsundergoing revisionfunctionalendoscopicsinussurgery.IntForumAllergy Rhinol.2013;3:139---46.
21.KangHS,HanJJ,OhHK,KookMS,JungS,ParkHJ.Anatomical studiesoftheorbitalcavityusingthree-dimensionalcomputed tomography.JCraniofacSurg.2016;27:1583---8.
22.LethausB,WeiglS,Kloss-BrandstätterA,KlossF,KesslerP, Höl-zleF, etal. Looking for landmarksin medialorbital trauma surgery.IntJOralMaxillofacSurg.2013;42:209---13.
23.JiY,QianZ,DongY,ZhouH,FanX.Quantitative morphome-tryoftheorbitinChineseadultsbasedonathree-dimensional reconstructionmethod.JAnat.2010;217:501---6.