CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports5(2014)509–512
ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
j o u r n al ho m e p a g e :w w w . c a s e r e p o r t s . c o m
Bilateral
intertrochanteric
and
femoral
diaphyseal
fractures
with
unilateral
proximal
tibial
fracture:
A
case
report
and
review
of
the
literature
Ali
Seker
a,∗,
Adnan
Kara
a,
Mustafa
Faik
Seckin
b,
Mesut
Sonmez
c,
Erden
Erturer
b,
Irfan
Ozturk
daIstanbulMedipolUniversityMedicalFaculty,DepartmentofOrthopaedicsandTraumatology,Turkey bIstanbulBilimUniversityMedicalFaculty,DepartmentofOrthopaedicsandTraumatology,Turkey cSisliEtfalTrainingandResearchHospital,OrthopaedicsandTraumatologyClinic,Turkey
dIstanbulUniversityIstanbulMedicalFaculty,DepartmentofOrthopaedicsandTraumatology,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received23April2014 Accepted2June2014 Availableonline16June2014
Keywords:
Intertrochantericfracture Femoraldiaphysealfracture Bilateral
a
b
s
t
r
a
c
t
INTRODUCTION:Bilateralintertrochantericfemurfracturesarerelativelyrareinjuries.Thisstudyaims
topresentacaseofapatientwithsimultaneousbilateralintertrochantericfemurfracturesandfemoral
diaphysealfracturesandproximaltibialfracturewithhistwelveyearsfollow-up.
PRESENTATIONOFCASE:A44-year-oldmanpresentedtoemergencydepartmentafteramotorvehicle
accident.Bilateralintertrochantericfemurfractures(OTAclassification–31A.1.2)andbilateralfemoral
diaphysealfractures(OTAclassification–32A.2)andnondisplacedrightproximaltibialfracture(OTA
classification–41B.1)weredeterminedinradiographs.Followingclosedreduction,fractureswerefixed
withintramedullarynailsbilaterally.Proximaltibialfracturewasfixedwithcannulatedscrewsfollowing
openreduction.Attwelfthyearfollow-uphewasabletodohisdailyactivitieswithminimallimitation.
DISCUSSION:Highenergytraumas,stressfractures,systemicdisorders(osteomalacia,chronicrenal
fail-ure),steroidtreatments,seizuresandelectricinjuriesarepossiblecausesforbilateralhipfactures.
Howeverbilateralfemoraldiaphysealfracturesaremostlyduetohighenergytraumas.Long-term
biphos-phonateusemayalsocausebilateralfractures.Single-stagesurgeryshouldbeperformedinordertoavoid
secondarydamagesofsurgicalinterventions.Allfracturesofourpatientwerefixedinasinglesession.
Thispreventedfurtherdeteriorationofpatient’sstatusandmaderehabilitationeasy.
CONCLUSION:Carefulevaluationofallsystemsshouldbeperformedinmulti-traumapatientstofindout
concomitantinjuries.Singlestagedsurgicaltreatmentmaydecreasemorbidities.
©2014TheAuthors.PublishedbyElsevierLtd.onbehalfofSurgicalAssociatesLtd.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/3.0/).
1. Introduction
Intertrochantericfemurfracturesandfemoraldiaphyseal frac-tures are frequently seen in emergency departments in daily practice.Simplefallsaremaincausesofthesefracturesinelderly patientsbut high energy traumas are leading causesin young population.1 Althoughbilateralfemoraldiaphysealfracturesare
relativelycommonproblem, bilateralintertrochantericfractures arerare.
Thisarticleaimstoreportapatientwithsimultaneousbilateral intertrochantericfemurfractureswithbilateralfemoraldiaphyseal fracturesandunilateralproximaltibialfractureandhis12years follow-up.Toourknowledgethereisnosuchacaseinliterature.
∗ Correspondingauthorat:MedipolMegaHastane,TEMAvrupaOtoyoluGoztepe C¸ıkıs¸ıNo.1,Bagcilar,Istanbul,Turkey.Tel.:+905323262202;fax:+902124607070.
E-mailaddress:[email protected](A.Seker).
2. Presentationofcase
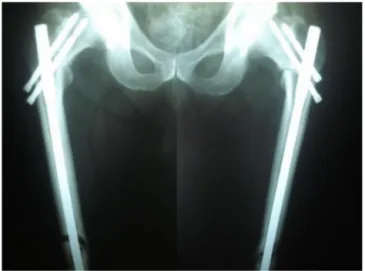
A44-year-oldman waspresented toemergency department afteramotorvehicleaccident.Onphysicalexaminationlocal ten-dernessandswellingwaspresentoverboththighsandrightknee. His vital signs were 90/60mmHg blood pressure and 130/min pulserate.Thehemoglobinlevelwas10.2g/dlinitially.Bilateral intertrochantericfemurfractures(OTAclassification–31A.1.2)and bilateralfemoraldiaphysealfractures(OTAclassification–32A.2) and nondisplaced right proximaltibial fracture (OTA classifica-tion – 41B.1)were determinedin radiographs (Fig. 1).He was operatedonthefifthdayofadmissionafterhemodynamic stabi-lization.Transtibialskeletaltractionswereappliedforbothsides uptosurgery.Inasinglesession,lockedintramedullarynailswere usedforthefixationofintertrochantericanddiaphysealfemoral fracturesafterclosedreductionforbothextremities.Open reduc-tionandinternalfixationwithcannulatedscrewswereperformed forrightproximaltibialfracture.Fourunitsofpackedredblood
http://dx.doi.org/10.1016/j.ijscr.2014.06.001
2210-2612/© 2014TheAuthors. Publishedby ElsevierLtd.on behalfof SurgicalAssociates Ltd.Thisis an openaccessarticle underthe CCBY-NC-ND license
CASE
REPORT
–
OPEN
ACCESS
510 A.Sekeretal./InternationalJournalofSurgeryCaseReports5(2014)509–512
Fig.1.Radiographsshowfracturesofbothfemur.
cells and two units of fresh frozen plasma were given to the patienttotally.Arehabilitationprogramwasstartedimmediately aftersurgery.Oneweekaftersurgeryseropurulentdischargewas observedfromtheincisionofrighttibia.Staphylococcusaureuswas cultivated.Infectionwastreatedwithoralantibiotics.Patientwas discharged12daysafteroperation.Weightbearingwasallowed6 weeksaftersurgeryforbothsides.Dynamizationofbothnailswere performedat4thmonthduetodelayedunion.(Fig.2)Complete unionoffractureswereshowedwithradiographsat8th month followup.Implantswereremovedthreeyearslater.Patienthad mildpain,especiallyinhisrighthip,andlimpat12thyearcontrol. Degenerativechangeswereobservedatrighthiponradiographs. (Fig.3)Althoughmovementsofrighthipwererestricted,hewas abletodohisdailyactivitieswithminimallimitationandwithout medication(Fig.4).
3. Discussion
Althoughproximalfemoralfracturesarefrequentlyseenindaily practice,bilateralfracturesarerare.Casereportsinliteratureare mostlyrelatedwithbilateralfemoralneckfracturesorfractures
Fig.2. Atpostoperative4thmonthcompleteunionwasnotachievedand dynamiza-tionofnailswereperformedbilaterally.
Fig.3.Degenerativechangeswereobservedinrighthipat12thyearcontrol radio-graph.
withmixedpatterns.Onlyfewpapersarereportingsimultaneous bilateralintertrochantericfemurfractures.Ourcaseisthefirstfor simultaneous bilateralintertrochantericand femoraldiaphyseal fractures.
High energy traumas, stress fractures, systemic disorders (osteomalacia,chronicrenalfailure),steroidtreatments,seizures andelectricinjuriesarepossiblecausesforbilateralhipfactures.2–7
Howeverbilateralfemoraldiaphysealfracturesaremostlydueto highenergytraumas.Long-termbiphosphonateusemayalsocause bilateralfractures.8
Grisoni et al.1 reported 8 bilateral cases (0.3%) in 2426
hipfractures and only two patients had simultaneous bilateral intertrochantericfractures.Themechanism ofinjurywasmotor vehicleaccidentfora patientand simplefallfortheother.First patientwasa53-year-oldmaleandhadadditionaltibiaandpatella fractures.Secondpatientwasa88-year-oldwomanwithout addi-tionalinjury.Bothpatientswereoperatedinasinglesessionand dynamichipscrews (DHS)werepreferredfor fixation.Younger patientwasdischargedtohomebutelderonewasdeadat post-operativeseventhday.
Dendrinosetal.9reportedthreecaseswithsimultaneous
bilat-eralhipfractures.One ofthesepatientswasa 53-year-oldguy withbilateralcomminutedpertrochantericfractures.Mechanism ofinjurywasamotorvehicleaccident.Duetothevisceralinjuries bothhipswerefixedwithslidingscrew-platesystemfivedaysafter laparatomy.Mildpaininrighthipandslightlimp wasnotedat the26thmonthfollow-up.Othertwopatientshadbilateral sub-trochantericfractures.
Panagopoulosetal.2reporteda44-year-oldpatientwith
bilat-eral intertrochanteric femur fractures. He had additional left acetabularandleftdistalradiusfractures.Patientwastreatedwith proximalfemoralnailinginsinglesession. Distalradiusfracture wasoperatedatthesametime.Conservativetreatmentwas cho-senforacetabularfracture.Authorsgave18monthsfollow-upwith goodresults.
CASE
REPORT
–
OPEN
ACCESS
A.Sekeretal./InternationalJournalofSurgeryCaseReports5(2014)509–512 511
Fig.4.Despitedegenerativechangesintheradiographspatientwasabletodohisdailyactivitieswithminimalrestriction.
Harshvardhan3 reported a 40-year-old man with bilateral
intertrochantericfemurfractureswithoutadditional injury.The mechanismof injurywasamotor vehicleaccident.Patientwas treatedwithtwo-stageinternalfixationwithDHSinonesideand DynamicCondylarScrewintheother.Postoperativefollow-ups werenotincludedinthetext.
Balietal.4reportedapatientwithbilateralpertrochanteric
frac-tureswithbilateralpatellarfracturesandunilateralmedialtalar processfracture.HipfracturesweretreatedwithDHSand bilat-eralpatellarfractureswithORIFinasinglestagedsurgery.Atthe endoftheoneandhalfyear-follow-uppatientreturnedtohisdaily activitieswithminimaldifficulties.
Suhetal.5reportedapatientwithbilateralfemoralneck
frac-turessecondarytohypocalcemicconvulsion.Patientwastreated withmultiplecannulatedscrews.Duringpostoperative rehabili-tationpatientadmittedtohospitalafterconvulsionandbilateral intertrochantericfemurfractureswerediagnosed.Theauthors pre-ferredrevisionofonesidewithDHSandconservativetreatmentfor otherside.Completeunionoffractureswithoutavascular necro-sisoffemoralheadswerereportedathispostoperative2.5years follow-up.
Optimaltimingforsurgeryofpolytraumapatientsaredecided according to “Damage Control Orthopaedics’ principles. 10 Our
patientwasoperatedfivedaysaftertrauma.Bringingpatientto optimallevelforsurgerywasthecauseofdelay.Itisacceptedthat polytraumapatientswithhemodynamicstabilitycouldbeoperated early.Operationsofpatientsinborderline,unstableandextremis groupshouldbedelayed.Injuryseverityscoreofourpatientwas 32=9pointsandhewasinstablegroup.Hewouldbeoperated
early.
Despiteexceptionsinliterature,3 ifit ispossiblesingle-stage
surgeryshouldbeperformedinordertoavoidsecondarydamages ofsurgicalinterventions.Allfracturesofourpatientwerefixedin asinglesession.Thispreventedfurtherdeteriorationofpatient’s statusandmaderehabilitationeasy.
Although the primary goal of hip fracture treatment is fix-ation in acceptable position with closed reduction, it cannot be achieved always. In such cases open reduction should be performed.Intramedullary nails,dynamic hipscrews, proximal femurplatesandexternalfixatorscanbeusedinthetreatmentof intertrochantericfemurfractures.Duetoipsilateralfemoral dia-physealfracturesintramedullarynailswereourchoiceinthiscase. Inordertopreventhemodynamicdeteriorationofpatient,fractures werereducedinclosedmannerbutfemoraldiaphysealfractures madereduction difficult.Fixation in varusmalposition wasthe endresultforbothhips.Theaimofintramedullarynailingwasto allowearlyweightbearing.Withoutproperfracturereductionnail causedvarusangulationoffracture.Applicationofnailafteropen
reductionorfixationofhipandfemoraldiaphysiswithdynamic hipscrewwithlongplateafteropenreductionwouldbebetter.
Atfinalcontrol,arthroticchangeswereobservedinradiographs. Patientwasabletodohisdailyactivitieswithmildpainand with-outpainkiller.Harrishipscorewas81pointswithgoodresult.If openreductionwasperformed,suchacomplicationwouldnotbe observedandbetterfunctionaloutcomewouldbegot.
4. Conclusion
Bilateralhipfracturesareveryrare.Carefulevaluationofother systemsshouldbeperformedinsuchcasestofindoutconcomitant injuries.Singlestagedsurgicaltreatmentmaydecreasemorbidities. Openreductionshouldbekeptinmindifclosedreductioncouldnot beperformed.
Conflictofinterest
Theauthorsdeclarethatthereisnoconflictofinterest Funding
Thereisnosponsorforthisstudy. Ethicalapproval
Writteninformedconsentwasobtainedfromthepatientfor publicationofthiscasereport.Acopyofthewrittenconsentis avail-ableforreviewbytheEditor-in-Chiefofthisjournalonrequest. Authorcontributions
AliSeker,studyconceptordesign,datacollection,writingthe paper;AdnanKara,datacollection;MustafaFaikSeckin,data col-lection;MesutSonmez,datacollection;ErdenErturer,writingthe paper;IrfanOzturk,writingthepaper.
Keylearningpoints
• Bilateralintertrochantericfracturewithbilateralfemoral diaphy-sealfractureisveryrare.
• Managementofsuchinjuriesischallenging.
• Thequalityofreductionandfixationaregoingtoaffectthefinal results.
References
1.GrisoniN,FoulkD,SprottD,LaughlinRT.Simultaneousbilateralhipfracturesin
CASE
REPORT
–
OPEN
ACCESS
512 A.Sekeretal./InternationalJournalofSurgeryCaseReports5(2014)509–512
2.PanagopoulosA,PapadopoulosD,GiannikasD,TyllianakisM.Simultaneous
bilateraltraumaticinter-trochantericfractures:acasereport.ActaOrthopaed
TraumatolHellenica2002;53:284–6.
3.HarshvadhanJ,PrabhakarMM.Acaseofbilateralsimultaneoustraumatic
intertrochantericfractureinayoungpatientduetodashboardinjury.InternetJ
OrthopSurg2008;10:3.
4.BaliK,KrishnanV,SenR. Bilateralpertrochantericfractureswithbilateral
patellarfractureswith missedmedialprocessfracture oftalus inayoung
adult:a casereportand reviewof literature.MusculoskeletSurg2011;95:
259–63.
5.SuhKT,KangDJ,LeeJS.Bilateralintertrochantericfracturesaftersurgical
treat-mentofbilateralfemoralneckfracturessecondarytohypocalcemicconvulsions
withchronicrenalfailure:acasereportandreviewoftheliterature.ArchOrthop
TraumaSurg2006;126:123–6.
6.KöseN,Ozc¸elikA,GünalI,SeberS.Spontaneousbilateralhipfracturesina
patientwithsteroid-inducedosteoporosis–acasereport.ActaOrthopScand
1998;69:195–6.
7.ShaheenM,SabetN.Bilateralsimultaneousfractureofthefemoralneck
follow-ingelectricalshock.Injury1984;16:13–4.
8.CapeciCM,TejwaniNC.Bilaterallow-energysimultaneousorsequentialfemoral
fracturesinpatientsonlong-termalendronatetherapy.JBoneJointSurgAm
2009;91:2556–61.
9.Dendrinos G, Kousoulas D, Papagiannopoulos G. Simultaneous bilateral
trochantericandsubtrochantericfractures:casereports.JTrauma1993;34:
157–60.
10.PapeHC,GiannoudisP,KrettekC.Thetimingoffracturetreatmentin
poly-traumapatients:relevanceofdamagecontrolorthopedicsurgery.AmJSurg
2002;183:622–9.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.
View publication stats View publication stats