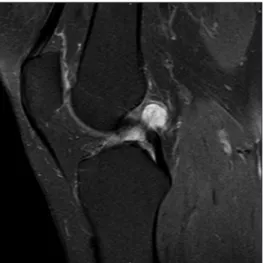
Simultaneous bilateral ganglion cysts of the anterior cruciate ligaments
Tam metin
Şekil
Benzer Belgeler
In this project we have developed an “Electronics Concealed Box” which consists of Arduino, RTC (Real Time Clock), RFID Reader, RFID tags(Main Examiner and Invigilator),
Pitchai, “Prognostic evaluation of multimodal biometric traits recognition based human face, finger print and iris images using ensembled SVM classifier” , Cluster Computing ,
According to the results of the data analysis, it is observed from the viewpoint of the company managers, among the methods of development and acquisition of information
Hamdi Paşanın Berutta huo çeten öldüğü o vakit çıkan *-a- rik gazetesinde görülmesi üze rine sarayca telâşı mucip o ou Baş kitabetten Sadrazam S a ıl
Macaristan’da iki Burley tütün çeşidinde üç yıl boyunca farklı azot dozlarının (0, 4, 8, 12, 16 ve 20 kg/da N) verim, kalite, olgunlaşma oranı, yeşil yaprak verimi,
對於希望接受手術的人而言,最重要的是風險利益的評估,特別是屈光手術這類
18 As recommended by the European Council Conclusions of 14 December 2012, the duties of the Adri- atic-Ionian Interregional Group were: drafting an action plan, that takes into
