Acil hekimlerinin ve radyoloji uzmanlarının abdomen BT yorumlama düzeylerinin karşılaştırılması
Tam metin
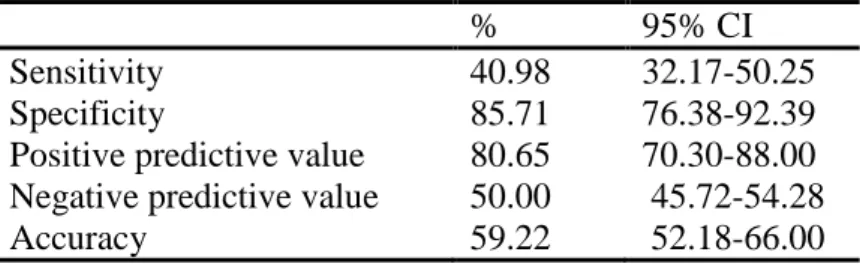
Şekil


Benzer Belgeler
The T-test results show significant differences between successful and unsuccessful students in the frequency of using the six categories of strategies except
He went to Cayirova Primary School as Primary School, Türk Maarif Koleji as middle school and high school.He graduated from the Computer Engineering Department in 2001at
The adsorbent in the glass tube is called the stationary phase, while the solution containing mixture of the compounds poured into the column for separation is called
In this chapter, abolition of cizye (tax paid by non-Muslim subjects of the Empire) and establishment of bedel-i askeri (payment for Muslims non-Muslims who did not go to
Overall, the results on political factors support the hypothesis that political constraints (parliamentary democracies and systems with a large number of veto players) in
In this story, Joyce writes about the main character Eveline, whose desire to fit into the role of loyal Catholic daughter prevents her from fleeing with her sweetheart Frank to
Systematic review of associations between the presence of acute ischemic lesions on diffusion-weighted imaging and clinical predictors of early stroke risk after
METHODS: The study was conducted retrospectively and included 26 acute ischemic stroke patients who only received intravenous thrombolytic therapy in Cankiri State Hospital
