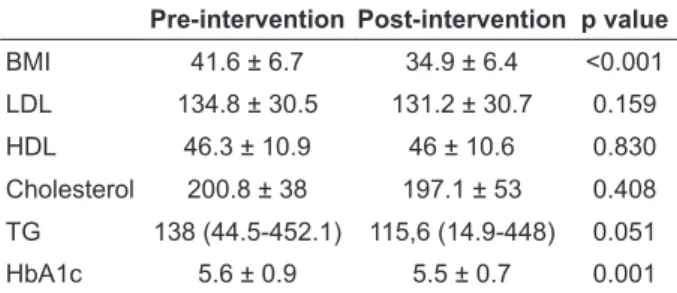
Effects of Intragastric Balloon on Body Mass Index, Lipid Profile and Blood Glucose Regulation: A Prospective Study
Tam metin
Şekil
Benzer Belgeler
Eseri yaşatmak, her yıl daha iyisini yapmak için çaba sarf etmekle, okuyucularımızın teveccühünü kazanmaya ça lışıyor ve ancak bu takdirde O’na lâyık
香港中文大學學生蒞校參訪見習 香港中文大學那打素護理學院 12 名國際生,於 2014 年 11 月 11 日至 25
為以香港大學臨床試驗中心為標竿學習的對象,本校特別邀請香港大學醫學院臨床 試驗中心主任 Johan Karlberg 教授、副主任 Henry
CONCLUSIONS: This study shows that under well-designed conditions, Tai Chi exercise training could decrease blood pressure and results in favorable lipid profile changes and
CONCLUSIONS: This study shows that under well-designed conditions, Tai Chi exercise training could decrease blood pressure and results in favorable lipid profile changes and
Ethanolic extract of adlay bran and residue from ethanolic extraction of adlay bran significantly suppressed the formation of ACF in the distal colons but did not aff ect the
Deniz Hastahanesinin köşesindeki çeşme tek parça bir mermer üzerine işlenmiş Barok kabart malı bir ayna taşı ve üst kısmında bir buçuk kıt'alık
