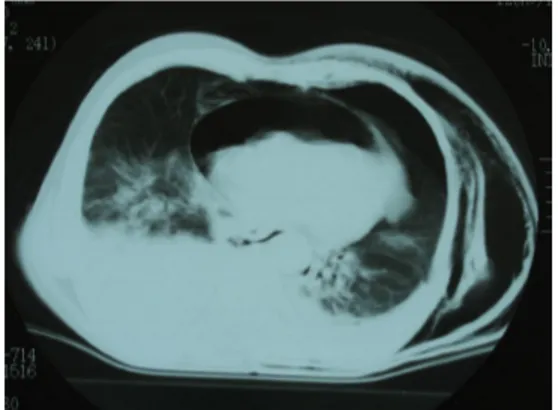
74 Year-old-man with pneumopericardium due to blunt chest trauma: Case report
Tam metin
Şekil
Benzer Belgeler
Although Hal- stead and coworkers 12 presented 3 valvular injury cases treated only with repair of the native aortic valve, we believe that valve replacement is usually necessary,
Amaç: Çal›flmam›zda transrektal ultrasonografi (TRUS) eflli¤inde prostat biyopsisi yap›lan hasta- larda prostat kanseri (PK) insidans›n› belirlemeyi ve prostat kanseri
臺北醫學大學衛生政策公報 第四十二期
ANLATIM BİÇİMLERİ VE DÜŞÜNCEYİ GELİŞTİRME YOLLARI Anlatım Biçimleri Açıklayıcı Anlatım (Açıklama) Öyküleyici Anlatım (Öyküleme) Betimleyici Anlatım
Dynamic perfusion and functional cardiac and thoracic MRI was performed to rule out any thoracic or cardiac anomaly and it demonstrated a cur- vilinear density in the right
Rupture of main bronchus due to blunt chest trauma in children: a report of two cases.. Çocuklarda ana bronşun künt göğüs travması kaynaklı rüptürü: İki olgu sunumu Ilan Bar, 1
It showed a large, traumatic, saccular false aneurysm of the right common carotid artery after truncal bifurcation (Fig.. There was no
ÖLÇME, DEĞERLENDİRME VE SINAV HİZMETLERİ GENEL MÜDÜRLÜĞÜ KİTAPÇIK TÜRÜ A.. Cevaplarınızı, cevap kağıdına
