Association between obstructive sleep apnea syndrome and waist-to-height ratio
Tam metin
Şekil

Benzer Belgeler
Methods: After applying the exclusion criteria, the retrospective study population consisted of 330 patients, including 110 patients with isolated CAE, 110 with obstructive
White blood cell (WBC) count and subtypes are well known measurements as inflammatory markers (3-5) in cardiovascular disease and its index as the ratio between neutrophils and
Accordingly, when patients with cellulitis were divided into two groups as ≥65 years and <65 years, a statistically sig- nificant difference was noted among the WBC, NLR, and
Elevated C-re- active protein levels and increased cardiovascular risk in patients with obstructive sleep apnea syndrome. Szkandera J, Pichler M, Gerger A, et al (2013b)
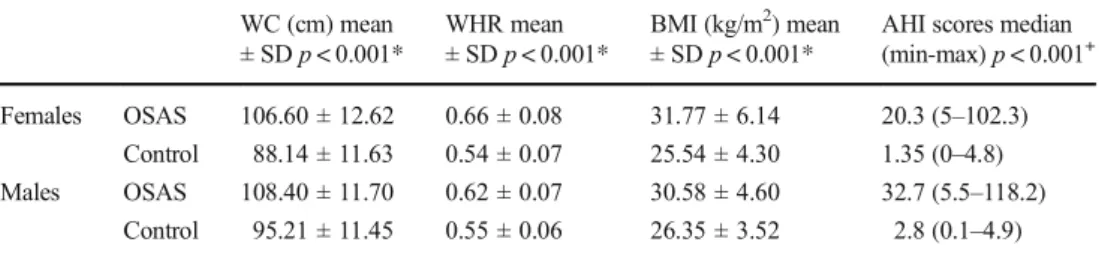
Neutrophil to lymphocyte ratio, TST: Total sleep time, AHI: Apnea Hypopnea index, SRO: Position related OSAS, RRO: Rem related OSAS, HSN: Simple (habitual) snorer... gradually
In our study, we aimed to compare inflammation marker levels between patients diagnosed with OSAS based on polysomnography and the control group, determine the
The aim of the present study was to investigate the usefulness of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) in patients diagnosed with Bell’s
The lymphocyte counts of group 4 (obese OSAS group) were the lowest among all groups; these values were lower than the lymphocyte counts of groups 1 (control group),
