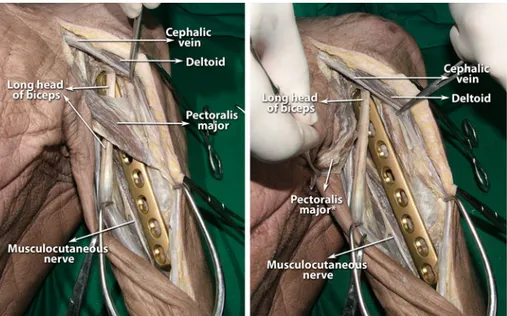
Clinical evaluation of an antero-medial approach for plate fixation of the proximal humeral shaft
Tam metin
Şekil

Benzer Belgeler
The explorers refer the monuments of cultural and historical heritage (historical territories, architectural buildings and complexes, archaeological areas, museums
Türk mitolojisinde ve destanlarında cet/ata, koruyucu/hami, bilge ve yol gösterici gibi pek çok fonksiyonu olan at, Türk masallarında baĢlı baĢına bir masal tipi
Makalede “Mektup-5” olarak adlandırılan ve 23 Mayıs 1918 tarihinde, Batum görüşmelerinin çıkmaza girdiği günlerde Enver Paşa’ya çekilen telgrafta, Mavera-yı
Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with
There are three services generally named as Infrastructure as a Service (SaaS) , Platform as a service (PaaS) and software as a service (SaaS) as provided by cloud
It yielded good results and higher performances of vehicle detection using vehicle dataset and it had overcome the problem of small, medium and large object detections,
Malware Materials Detection by Clustering the Sequence using Hidden Markov Model Muhammed Mofe N AL Rwajah a and Ravi Rastogi ba. Master Student, Faculty of Computing and
Also, Lakshmi (2011) have measured the overall work life imbalances among 120 women teachers in various educational institutions and noted that the negative attitude of
