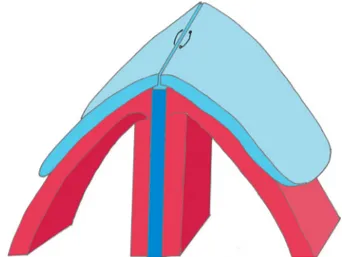
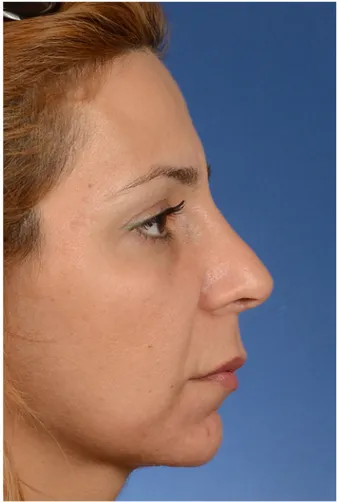
Evaluation of postoperative patient satisfaction after covering the nasal dorsum with upper lateral cartilage: "upper lateral closing"
Tam metin
Şekil

Benzer Belgeler
Results: Nasal obstruction frequency and severity scores in patients treated with both radiofrequency and lateral displacement on post-operative days 3, 5 and 7 were found to
As the goal is finding H(n, p, o), the homing sequences that can be found for the possible FSMs generated by adding output to an automaton which has shorter synchronizing sequence
Bu çalışmada hastaların ultraso- nografi hakkındaki bilgi düzeyleri ölçülerek hekim- hasta arasındaki iletişimin şekli ve ultrasonografi kalitesine etki- sinin
Systemic, neurological, or psychogenic itching should be considered in the absence of lesions on the skin or in the presence of secondary lesions such as excoriations,
Herein we report a case presenting with massive upper eyelid swelling and tension causing severe pain, epiphora, upper eyelid/eyelash ptosis and corneal epithelial erosion.. The
In addition to providing drivers and passengers with a wide range of information, this method of communication allows safety applications to enhance road safety
The axial view of chest computed tomography (CT) scan revealed continuity of the line of the right lateral process of the second thoracic vertebra to the mass no other
Keywords: Trimethoprim/sulfamethoxazole, cerebral toxoplasmosis, Kaposi’s sarcoma, magnetic resonance imaging, Toxoplasma gondii Anahtar Kelimeler: Trimetoprim/sülfametoksazol,
