www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Comparison
of
anxiety
and
child-care
education
characteristics
of
mothers
who
have
children
with
or
without
speech
delays
夽
Talih
Özdas
¸
a,∗,
Ays
¸e
Sanem
¸ahlı
S
b,
Behiye
Sarıkaya
Özdemir
c,
Erol
Belgin
daAdanaNumuneEducationandResearchHospital,OtolaryngologyClinic,Adana,Turkey
bHacettepeUniversity,VocationalSchoolofHealthServices,HearingandSpeechTrainingCenter,Ankara,Turkey
cAnkaraChildHealthandDiseaseHematology,OncologyEducationalResearchHospital,DepartmentofPediatric,Ankara,Turkey dIstanbulMedipolUniversity,FacultyofHealthSciences,AudiologyDepartment,Istanbul,Turkey
Received21August2017;accepted11December2017 Availableonline5January2018
KEYWORDS
Mother; Anxietylevel; Speechdelay; Beckanxietyscale; PARI
Abstract
Introduction:Speechdelayinachildcouldbethecauseand/orresultoftheemotionaldisorder. Thechildrearingattitudethattheparentshaveacceptedcouldhavebothpositiveandnegative effectsonthepersonalityofthechild.
Objective: The current study aimed to investigate the sociodemographic features andthe mothers’anxietyofchildrenwithspeechdelay.
Methods:One hundredfivemotherswith childrenaged between3and6yearswithspeech delayswereincludedinthepatientgroup,and105motherswhohavechildrenagedbetween3 and6yearswithnormalspeechandlanguagedevelopmentwereincludedinthecontrolgroup. Aninformationformquestionnaireincludingdemographiccharacteristics,theFamilyLifeand Childrearing AttitudeScale(PARI---ParentalAttitudeResearchInstrument)andBeckanxiety scalewererequestedfromallmothersinthepatientandthecontrolgroups.
Results:Inthecurrentstudy,therewasasignificantdifferencebetweenthegroupsintermsof gender(p=0.001).AccordingtoParentalAttitudeResearchInstrument,themeanofmothers ofthechildren withspeechdelayswashigherthanthemeanofmothersofnormalchildren
夽 Pleasecitethisarticleas:Özdas¸T,S¸ahliAS,ÖzdemirBS,BelginE.Comparisonofanxietyandchild-careeducationcharacteristicsof
motherswhohavechildrenwithorwithoutspeechdelays.BrazJOtorhinolaryngol.2019;85:199---205.
∗Correspondingauthor.
E-mail:[email protected](T.Özdas¸).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial. https://doi.org/10.1016/j.bjorl.2017.12.004
1808-8694/©2017Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
intermsoftheanswerstooverprotectivemotheraspect(p<0.01).Themothersofchildren withspeechdelayshadmoreoverprotectivemotherhoodattitudes;however,thedifferencein termsoftheanswerstotheaspectsofdemocraticattitudeandprovisionofequality,refusal tobeahousewife,husband-wifeconflict,andsuppressionanddisciplinewerenotstatistically significant.The Beckanxiety scale, asignificantdifference was detectedbetween the two groups(p<0.01).Itwasfoundthatthemothersofchildrenwithspeechdelayshadmoresevere levelsofanxiety.
Conclusion:Thesocialstructureofthefamily,theattitudesandthebehaviorsofthemother, andtheanxietylevelsofthemothershaveimportanteffectsonchilddevelopment.Thus,it isnecessarytoperformfurtherstudiesrelatedtospeechdelays,inwhichmanyfactorsplaya roleintheetiology.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/). PALAVRAS-CHAVE Mãe; Níveldeansiedade; Atrasonafala; Escaladeansiedade deBeck; PARI
Comparac¸ãodaansiedadeecaracterísticasdaeducac¸ãoinfantilemmãescomfilhos comousematrasosnafala
Resumo
Introduc¸ão:Oatrasodafalaemumacrianc¸apodeseracausae/ouoresultadodedistúrbio emocional.Asatitudestomadaspelospaisnaeducac¸ãodacrianc¸apodemterefeitospositivos enegativossobreapersonalidadeinfantil.
Objetivo:Investigarascaracterísticassócio-demográficaseaansiedadedasmãesdecrianc¸as comatrasonafala.
Método: Foramincluídasnogrupodepacientes105mãescomcrianc¸asentre3e6anosde idadeeatrasosnafala,enogrupocontrole105mãescomcrianc¸asnamesmafaixaetáriae desenvolvimentonormaldafalaedalinguagem.Foisolicitadoàsmãesdeambos osgrupos opreenchimentodeinformac¸õesemumformulário,incluindocaracterísticasdemográficas,o instrumentoFamilyLifeandChildRearingAttitudeScale(PARI---ParentalAttitudeResearch Instrument)eoinventáriodeansiedadeBeck.
Resultados: Noestudoatual,houvediferenc¸asignificativaentreosgruposemrelac¸ãoaogênero (p=0,001).DeacordocomoinstrumentoParentalAttitudeResearchInstrument,amédiadas mãesdascrianc¸ascomatrasosnafalafoimaiordoqueamédiadasmãesdecrianc¸asnormaisem relac¸ãoàsrespostassobresuperprotec¸ãomaterna(p<0,01).Asmãesdecrianc¸ascomatrasos nafalaapresentarammaisatitudesdeprotec¸ãomaternaexcessiva;noentanto,adiferenc¸a dasrespostassobreatitudesdemocráticaseigualitarismo,recusadopapeldedonadecasa, conflitomaritaledisciplinarígidanãoforamestatisticamentesignificantes.Noinventáriode ansiedadedeBeckfoiencontradaumadiferenc¸asignificativaentreosdoisgrupos(p<0,01). Verificou-sequeasmãesdecrianc¸ascomatrasosnafalaapresentavamníveismaisgravesde ansiedade.
Conclusão:Aestruturasocialdafamília,asatitudes,ocomportamentoeosníveisdeansiedade das mães têm efeitos importantes nodesenvolvimento da crianc¸a. Conclui-se, portanto, a necessidadederealizarestudosadicionaisrelacionadosaosatrasosnafala,nosquaisdiversos fatoresdesempenhamumpapeletiológico.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Speechdelayisdefinedasinabilitytodemonstrate speech-languageskills thatis expectedaccording tothe age.The prevalenceofspeechdelayinchildrenbetweenaged2and 7 varies at the range of 2.3---19%. Speech delay through-out school period and continuing even at adulthood is observed in 5---8% of the children who had speech delay duringpreschoolperiod.1
There are many factors that could cause speech delays. The most frequently reported risk factors for speech delays are positive family history, male gen-der, a history of prematurity, and low birth weight. Other risk factors that are thought to be less associ-ated are low education level of the parents, history of childhood disease, late birth sequence, older parents, low socioeconomic status, and the presence of a large family.2,3
Anxiety disorders and depression are the most com-monpsychologicaldisordersinthegeneralpopulation.The prevalenceofanxietydisordersintheurbanpopulationwas 9.1%inmalesandas18.1%infemales.Speechdelayin chil-dren affects the emotional status of themother, and the emotionaldisorderordepressionofmothercouldalso nega-tivelyaffectspeechdevelopmentinchildren.Speechdelay inachildcouldbethecauseand/orresultoftheemotional disorder.4 Thechildrearingattitudethattheparentshave
acceptedcouldhaveboth positiveandnegativeeffectson thepersonalityofthechild.
The current study aimed toinvestigate the etiological factorsofspeechdelay inchildrenintermsof sociodemo-graphic features and tocompare the mothers of children withspeech delay and the mothers of normalchildren in termsofchildrearingattitudesandanxietylevels.
Materials
and
methods
Subjectrecruitment
Theparticipantswereinformedabout thestudy,andtheir verbalandwritteninformedconsentswereobtained.Local ethics committee approvedthe study protocol, andstudy was conducted in accordance withthe human rights and experimentalethics(ProjectNumber:KA15/168).
Atotalof105childrenwhowereadmittedtothe audi-ologysoundandspeechdisordersunitandear-throat-nose policlinicwith complaintsof speechdelay, andwho were diagnosed with speech delays as a result of speech and language assessment (the results of evaluation as normal receptive language anddelayed expressivelanguage) and their mothers; and 105 children with normal speech and theirmotherswereincludedinthestudy.
Psychosocialfactorsarethoughttobetheleadingcause ofetiologicalfactorsinchildrenwithspeechdelaywhoare includedinthestudy.Thesefactorsincludelackofspeech stimuli,inadequatesocialcommunicationinthefamily,and long-termuseoftelevisionandcomputers.thecontrolgroup wasrandomly selectedfromchildren aged3---6 yearswho wereattendingapreschoolinstitutioninaregionwiththe samesocioeconomiccharacteristics.Theresearchers inter-viewedtheirparentsandtheirteachersandlearnedabout theirlanguageandspeechdevelopment.Childrensuspected ofhavinglanguageand/orspeechdelayarenotincludedin thestudy.
Forboth groups, our inclusioncriteriais children aged 3---6yearswhowerenotathighriskofdevelopmentaldelay orsuspectedofhavingdevelopmentaldelayandour exclu-sion criterias are children born preterm (gestational age <37),withlowbirthweight(<2500g)andchildrenwithother knowdisordersthatmaybeassociatedwithoraffect devel-opment.Aftertheparentsoftheparticipantchildrenhave beeninformedabouttheprocess,participantpermissionto thestudyhasreceivedbysigningvoluntaryconsentform.
Physicalexaminations
Physical examinationsof the ear---throat---nose system and hearingassessmentswereperformedinallchildren,andthe children whohadhearinglevels between(−10)and (+15)
dB(decibel)wereacceptedasnormalandincluded inthe study.The children withmentalretardation, hearingloss, historyoftrauma,complicationsrelatedtoprevious child-hooddisease,andneurologicaldiseasewerenotincludedto thestudy.
Thespeechandlanguageassessment
Thespeechandlanguageassessmentwereperformedwith the Preschool Language Scale-Fifth Edition (PLS-5). PLS-5, which is widely used around the world, is a language assessmenttest thathasbeen preparedandimplemented by Zimmerman, Steiner, and Pond in 2011. The test was broughttoTurkey in 2013 and the Turkish translation, its adaptationforTurkishchildrenanditsvalidityand reliabil-ityis done with 1320 children between 0---7 yearsand 11 monthsbySahli,A.SandBelgin,E.Itisusedtodetermine whetherthereisdelayinlanguagedevelopment,toevaluate receptiveandexpressivelanguagedevelopment.5
Thedemographicinformation
Demographic information form consists of questions that interrogate not only demographic characteristics of the mother (age, occupation, educational status, number of children, economic status, etc.), but also information relatedto the child (age, which child, etc.), andvarious developmentalstatusesincludinglanguageandspeech.
ParentalAttitudeResearchInstrument,(PARI) [FamilyLifeandChildrearingAttitudeScale (FLCAS)]
PARI, developed by Schaefer and Bell in the United States in 1958,6 was adapted in 1978 by Guney le
Com-plete, Ayhan le Complete, and Serap Ozer.7 The scale
consists of 60 items and five subitems, including exces-sive motherhood/overprotection, refusal of the role of beingahousewife,offeringdemocraticapproach/equality, marriage conflict/disagreement, and strict discipline.6,7
Reliabilitycoefficientswerereportedtobe58and88,and thealphareliabilitycoefficientwas64.Thesecond adapta-tionhasbeenperformedbyKucuk(1990).8
Beckanxietyscale(BAS)
TheBASwasdeveloped byBecketal.in 1988,duetothe needforascalethatdifferentiatesanxietyanddepression.9
Itmeasurestheseverityofanxietysymptomsthatthe indi-vidualexperiences.TheBASisascalethatcontains21items, fourofwhichareself-assessmentitemsandgraded accord-ingtoaLikertscale(0---3)andiscompletedbythepatient. Thescoreintervalis0---63.Thehightotalscoreinthescale demonstratestheseverityoftheanxietythattheindividual experiences.Ascoreof0---8indicatestheabsenceofanxiety, ascoreof8---15indicatesamilddegreeofanxiety,ascoreof 16---25indicatesamoderatedegreeofanxiety,andascore of 26---63 indicates severe anxiety. The validity-reliability studieswereperformedbyUlusoy,Sahin,andErkmen.10
Dataanalysis
The SPSS 17.0 program was used for statistical analysis. Descriptivestatisticswereusedforthemean,standard devi-ation, median, and minimum and maximum values. The Chi-squaretestwasusedtoanalyzetheclassifieddata.The Student’st-testwasusedtocomparethemeanofthetwo groups,andtheone-wayANOVAtestwasusedtocompare themeanofmorethantwogroups.p<0.05wasaccepted asstatisticallysignificant.
Results
Recruitment
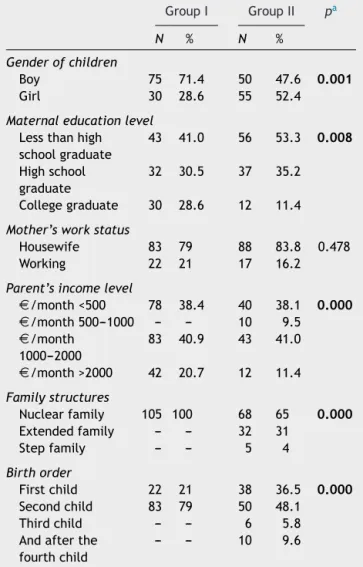
In the current study, the mothers of 105 children with speechdelaysandthemothersof105normalchildrenwere compared in terms of childrearing attitudes and anxiety levels of mothers, and the causes of speech delay were examined interms ofsociodemographic characteristics; a controlled comparison was performed. The demographic characteristicsofthemothersandchildreninboth groups aresummarizedinTable1.
Atotal of105 mothersof childrenwithspeechdelays, including75males(71.4%)and30females(28.6%), consti-tutedthepatientgroup.Atotalof105mothersofnormal children,including50males(47.6%)and55females(52.4%), constitutedthecontrolgroup.Thedifferencebetweenthe groupsintermsofgenderwasstatisticallysignificantusing theChi-squaretest(p=0.001)(p<0.01).
The age of the children in the patient group ranged between 36 and 72 months and the mean age was 55.18±17.29 months. The age of children in the control grouprangedbetween36and63monthsandthemeanage was45.42±8.51months.
TheresponsestotheBASbetweenstudyand
controlgroups
According to the responses to the BAS, anxiety was not detectedin46mothers(43.8%),mildanxietywasdetected in45mothers(42.9%),moderateanxietywasdetectedin7 mothers(6.7%),andsevereanxietywasdetectedin7 moth-ers(6.7%)amongthe105mothersofchildrenwithspeech delaysinthepatientgroup.
Accordingtotheresponses totheBAS,anxietywasnot detectedin57mothers(54.3%),mildanxietywasdetected in32mothers(30.5%),andmoderateanxietywasdetected in16mothers(15.2%)in the105mothersofchildren with normalspeechdevelopment.
When the mothers of children with speechdelays and those withnormal speechdevelopment were statistically comparedaccordingtotheresponsestotheBAS,a statisti-callysignificantdifferencewasdetected betweenthetwo groupsintheChi-squaretest(p<0.01)(Table2).
TheresponsestothePARIbetweenstudyand controlgroups
When the statistical results of the responses to the subitemsofPARIscalewascomparedinmothersofchildren
Table 1 Demographic characteristics of mothers in the studyandcontrolgroups.
GroupI GroupII pa
N % N %
Genderofchildren
Boy 75 71.4 50 47.6 0.001
Girl 30 28.6 55 52.4
Maternaleducationlevel
Lessthanhigh schoolgraduate 43 41.0 56 53.3 0.008 Highschool graduate 32 30.5 37 35.2 Collegegraduate 30 28.6 12 11.4
Mother’sworkstatus
Housewife 83 79 88 83.8 0.478 Working 22 21 17 16.2
Parent’sincomelevel
D/month<500 78 38.4 40 38.1 0.000 D/month500---1000 --- --- 10 9.5 D/month 1000---2000 83 40.9 43 41.0 D/month>2000 42 20.7 12 11.4 Familystructures Nuclearfamily 105 100 68 65 0.000 Extendedfamily --- --- 32 31 Stepfamily --- --- 5 4 Birthorder Firstchild 22 21 38 36.5 0.000 Secondchild 83 79 50 48.1 Thirdchild --- --- 6 5.8 Andafterthe
fourthchild
--- --- 10 9.6
N,numberofindividuals;%,percentage;Group I,mothersof childrenwithspeechdelays(n=105);GroupII,mothersof chil-drenwithnormalspeech(n=105).
a p-Value=0.05,consideredsignificant.Boldsarestatistically significant.
Table2 Distributionofanxietylevels ofmothers inthe controlandpatientgroupsaccordingtoscoresintheBAS.
GroupI GroupII N % N % Insignificant 46 43.8 57 54.3 Mild 45 42.9 32 30.5 Moderate 7 6.7 16 15.2 Severe 7 6.7 ---
---N,numberofindividuals;%,percentage;Group I,mothersof childrenwithspeechdelays(n=105);GroupII,mothersof chil-drenwithnormalspeech(n=105).
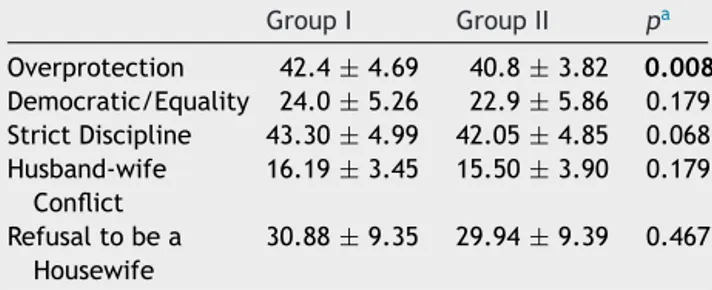
with speechdelays and with normal speechdevelopment (Table3).
Themeanscoreofmothersinthepatientgroup accord-ing to the answers to Overprotective Motherhood was 42.4±4.69. The mean score in the control group was
Table3 Distributionofmothersaccordingtoscoresinthe subdimensionsofPARIinthepatientandthecontrolgroups.
GroupI GroupII pa Overprotection 42.4±4.69 40.8±3.82 0.008 Democratic/Equality 24.0±5.26 22.9±5.86 0.179 StrictDiscipline 43.30±4.99 42.05±4.85 0.068 Husband-wife Conflict 16.19±3.45 15.50±3.90 0.179 Refusaltobea Housewife 30.88±9.35 29.94±9.39 0.467
SD,standarddeviation;GroupI,mothersofchildrenwithspeech delays (n=105); Group II, mothers of children with normal speechdevelopment(n=105).Resultsweregivenasmean±SD. a p-Value0.05 considered significant. Bolds are statistically significant.
40.8±3.82.Therewasastatisticallysignificantdifference between thetwogroups according totheStudent’s t-test
(p<0.01).Themeanscoreofthemothersofchildrenwith speechdelayswashigherthanthemeanscoreofthe moth-ersofchildrenwithnormalspeech.Themothersofchildren withspeechdelayshadamoreprotectivemotherhood atti-tude.
Themeanscoreofthemothersaccordingtotheanswers toOfferingDemocraticAttitudesandEqualitydimensionwas 24.0±5.26 in thepatient groupand it was22.9±5.86in thecontrolgroup.Therewasnostatisticallysignificant dif-ference between thetwogroups in terms of mean score, accordingtotheStudent’st-test(p>0.05).
The mean score of the mothers according to the responsestotheRefusaltobeaHousewifedimensionwas 30.88±9.35inthepatientgroupanditwas29.94±9.39in thecontrolgroup.Therewasnostatisticallysignificant dif-ferencebetweenthetwogroupsaccordingtotheStudent’s
t-test(p>0.05).
The mean score of the mothers according to the responses to the Husband-wife Conflict dimension was 16.19±3.45inthepatientgroupanditwas15.50±3.90in thecontrolgroup.Thedifferencebetweentwogroupswas notstatisticallysignificantaccordingtotheStudent’st-test
(p>0.05).
The mean score of the mothers according to the responsestotheSuppressionandDisciplinewas43.30±4.99 inthepatientgroupand42.05±4.85inthecontrolgroup. Similarly,thedifferencebetweentwogroupswasnot statis-ticallysignificantaccordingtotheStudent’st-test(p>0.05).
Discussion
Althoughtheetiologyofspeechdelayiscurrentlyunknown, many variableshave been described aspotentialrisk fac-tors. The most important risk factors for speech delay aremalesex,factorsassociatedwithsocioeconomic disad-vantage,familyhistoryof developmentalspeech-language disorder,andpersistentotitismedia.11 U.S.Preventive
Ser-vicesTask Force(USPSTF) wasunabletodevelop alistof specificriskfactorstoguideprimarycareprovidersin selec-tivescreening.Themostconsistentlyreportedriskfactors included a family history of speech and language delays, malesex,andperinatalfactors,suchasprematurityandlow
birthweight.12ThestudyofHorwitzetal.,13whichincluded
1189 children with speechdelays, in 2003, reported that 51% of the children were maleand 49% was female. The studyofZubricketal.,14conductedin2007andincludinga
totalof1766children,reported1528childrenwithnormal speechdevelopmentand238childrenwithspeechdelays.It reportedthat47.6%ofthechildrenthathadnormalspeech and70.8%ofthechildrenthathadspeechdelaysweremale andthedifferencewasstatisticallysignificant.
In the current study, among the children with speech delays, 75 (71.4%) were male, 30 (28.6%) were female, whereasamongthechildren withnormal speech develop-ment,50(47.6%) weremaleand55 (52.4%)werefemale. The difference between the groups in terms of gender wasstatisticallysignificant(p=0.001).Incomparisontothe literature,speechdelaysweremorecommoninmales com-paredtofemalesinthecurrentstudy.
InthestudyofSahli,15 whichwasconductedin20
chil-drenwithhearinglossandtheirfathersin2011,whenthe meanscoreofthefathersaccordingtothePARI subdimen-sions were examined, the scores of the dimension of the overprotectiveapproachweresignificantlyhigherinfathers ofchildrenwithhearingloss(42.76±5.59)comparedwith thefathersofchildren without hearingloss(40.16±6.55) (p<0.01).Itwasemphasizedthatthisresultwasan indica-torofmoreprotective behaviorbythefathersofchildren withhearingloss.Furthermore,thefathersofchildrenwith hearing loss had lower scores in the democratic/equality and strict discipline dimensions, and these values were statistically significant (p<0.01). Thus, this was empha-sizedasanindicator thatfathersofchildren withhearing loss demonstrate less democratic behavior and lesser discipline.
When the mothers of children with speechdelays and those with normal speech development were compared accordingtotheresponsestothesubdimensionsofthePARI. The mean score of the mothers of children with speech delays was higher than the mean score of the mothers ofchildrenwithnormalspeechdevelopment,accordingto theresponsestotheOverprotectivemotherhooddimension; the difference was statistically significant (p<0.01). The mothersofchildrenwithspeechdelaysdemonstratedmore protectivemotherhoodattitudes.
The difference in the mean score according to the responsestotheDemocraticAttitudesandEquality,Refusing tobeaHousewife,Husband-WifeConflict,andSuppression andDisciplinedimensionswere notstatisticallysignificant inmothers of childrenwithspeech delaysandthose with normalspeechdevelopment.
Itisknownthattheattitudeofthefamilyhasboth posi-tiveandnegativeeffectsonalldevelopmentalfieldsofthe children.The current study revealed that the mothers of childrenwithspeechdelaysdemonstratedmoreprotective attitudesandbehaviors.Motherswiththistypeofattitude couldnotunderstandthattheirchildrenareindividuals dif-ferent from themselves and these children need to gain theirindependence.Theseparentsalwaysbehaveasiftheir childrenweresmaller thanthey.They feedthe childthat eventuallyfeedshimself; theyclothethechildthat even-tuallyclothesbyhimself.Thus,asallneedsofthechildren aremetbytheirparents,itis thoughtthatthesechildren havenoneedtospeak.
The DepressionAnxietyStressScale (DASS)wasusedin thestudyofZubricketal.,andnormal,mild,and moderate-severe degrees of anxiety were detected in 94.5%, 1.9%, and3.7% of the mothers of children withnormal speech, respectively.Thedegree ofanxietywasnormal,mild,and moderate-severein 93.3%, 2.1%,and4.6% of themothers ofchildrenwithspeechdelays,respectively.Nostatistically significantdifferencewasdetectedbetweenthegroups.14
ThestudyofCırparetal.,16conductedin2010,included
themothersof18childrenwithspeechdelaysand20healthy children. The level of anxiety was evaluated with State-TraitAnxietyInventory(STAI). The mothers inthe patient group hadSTAI-S scores of 44±13.5 andSTAI-C scores of 45.2±9.4,andthemothersinthecontrolgrouphadSTAI-S scoresof36.9±9.9andSTAI-Cscores of41.0±5.3.A sta-tistically significant differencewas detected in the mean STAI-Sscoresofthemothersofchildrenwithspeechdelays andthemothersofhealthychildren(p=0.046).
In the current study, among 105 mothers of children withspeechdelays,anxietywasnotdetectedin46mothers (43.8%),mild anxietywasdetectedin45mothers(42.9%), moderate anxiety was detected in 7 mothers (6.7%), and severe anxiety was detected in 7 mothers (6.7%) accord-ingtotheBAS.Among105mothersofchildrenwithnormal speech,anxiety wasdetected in57mothers (54.3%),mild anxiety was detected in 32 mothers (30.5%), and moder-ateanxietywasdetectedin16mothers(15.2%).Whenthe answerstotheBASwerestatisticallycompared,asignificant differencewasdetected betweenthemothers ofchildren withspeechdelaysandthemothersofchildrenwithnormal speech(p<0.01).Furthermore,thecurrentstudyrevealed that the severity of anxiety in mothers of children with speechdelays wasgreater. Speechdelaysinchildren neg-ativelyaffectthelevelofanxietyinmothersandthehigh level of anxiety in mothers might also negatively affect speechdevelopmentin children.Itis thoughtthat speech delaysinchildrencouldbeboththecauseand/ortheresult oftheanxietydisorderinthemother.Thesmallsamplesize isthelimitationtothisstudythatshouldbeaddressed.
Conclusions
Whenthemeanscoresofmothersofchildrenwithspeech delaysandthemothersofhealthychildrenwerestatistically compared according to the responses to the subdimen-sionsof PARI, the mothersof children withspeechdelays demonstratedmoreprotectiveattitudesandbehaviors.The mothers who had such attitudes and behaviors met the requirementsoftheirchildren withouttheneed tospeak; therefore,speechmighthavebeendelayedinchildrenwho hadmotherswithsuchbehavior.
When the BAS of the mothers of children with speech delayswerecomparedtothemothersofnormalchildren,a significantdifferencewasdetectedbetweenthetwogroups, andthemothersof childrenwithspeechdelayshadmore severe anxiety. The anxiety might be a result of speech delaysinthechildrenandthe highlevelof anxietyinthe mothers might be the reason for the speech delay. Fur-therstudiesarerequiredtoinvestigatespeechdelaysand itsrelationship tothe family andsociety structure inour country.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgment
The currentstudywasapprovedbytheBaskentUniversity MedicalandHealthSciences ResearchCommittee(Project Number:KA15/168).Therewasnoinvolvementinthedesign or conduct of the study; collection, management, analy-sis,or interpretation ofthe data; or preparation,review, orapprovalofthemanuscript.
References
1.Wake M, Tobin S, Girolametto L, Ukoumunne OC, Gold L, Levickis P, et al. Outcomes of population based language promotion for slow to talk toddlers at ages 2 and 3 years: Let’sLearnLanguageclusterrandomisedcontrolledtrial.BMJ. 2011;343:460---503.
2.McLaughlinMR.Speechandlanguagedelayinchildren.AmFam Physician.2011;83:1183---8.
3.Nelson HD, Nygren P, Walker M, Panoscha R, Rockville MD. Screeningforspeechandlanguagedelayinpreschoolchildren: systematicevidencereviewfortheUSpreventiveservicestask force.Pediatrics.2006;117:298---319.
4.RudolphM,RosanowskiF,EysholdtU,KummerP.Anxietyand depressioninmothersofspeechimpairedchildren.IntJPediatr Otorhinolaryngol.2003;67:1337---41.
5.SahliAS,BelginE.Adaptation,validity,andreliabilityofthe PreschoolLanguage Scale-FifthEdition(PLS-5)intheTurkish context:theTurkishPreschoolLanguageScale-5(TPLS---5).IntJ PediatrOtorhinolaryngol.2017;98:143---9.
6.SchafferES,BellR.Developmentofaparentalattituderesearch instrument(PARI).ChildDev.1958;29:339---61.
7.LeCompteG,LeCompteA,SözenS.Childrearingattitudesof themothersfromthreesocio-economiclevelsinAnkara:ascale adaptation.JPsychology.1978;1:5---8.
8.KucukS.Thevaliditystudyofthe2nd,3rdand4thsubscales oftheTurkishadaptationofthePARIscale.In:V.National Psy-chologyCongressPsychologySeminarJournal,vol.8.1990.p. 451---9.
9.BeckAT,EpsteinN,BrownG,SteerRA.Aninventoryfor mea-suringclinicalanxiety:psychometricproperties.JConsultClin Psychol.1988;56:893---7.
10.Ulusoy M,Sahin NH, Erkmen H. Turkish version of the Beck AnxietyInventory:psychometricproperties.JCognPsychother. 1998;12:163---72.
11.ShribergLD,KwiatkowskiJ.Developmentalphonological disor-dersI:aclinicalprofile.JSpeechHearRes.1994;37:1100---26. 12.BerkmanND,WallaceI,WatsonL,Coyne-BeasleyT,CullenK,
WoodC,etal.Screeningforspeechandlanguagedelaysand disordersinchildrenage5yearsoryounger:asystematicreview fortheU.S.preventiveservicestaskforce,evidencesyntheses No.120.US:AgencyforHealthcareResearchandQuality;2015. 13.Horwitz SM, Irwin JR, Briggs-Gowan MJ, BossonHeenan JM, MendozaJ,CarterAS.Languagedelayinacommunitycohort of young children. J Am Acad Child Adolesc Psychiatry. 2003;42:932---8.
14.Zubrick SR, Taylor CL, Rice ML, Slegers DW. Late language emergenceat24months: anepidemiologicalstudyof preva-lence, predictors, and covariates. J Speech Lang Hear Res. 2007;50:1562---92.
15.SahliAS.Investigatingchildraisingattitudesoffathershaving ornothavingachildwithhearingloss.IntJPediatr Otorhino-laryngol.2011;75:681---5.
16.CirparOC,MulukNB,Yalc¸ınkayaF,ArikanOK,O˘guztürkO,Aslan F.State-TraitAnxietyInventory (STAI)assessmentofmothers withlanguagedelayedchildren.ClinInvestMed.2010;33:30---5.