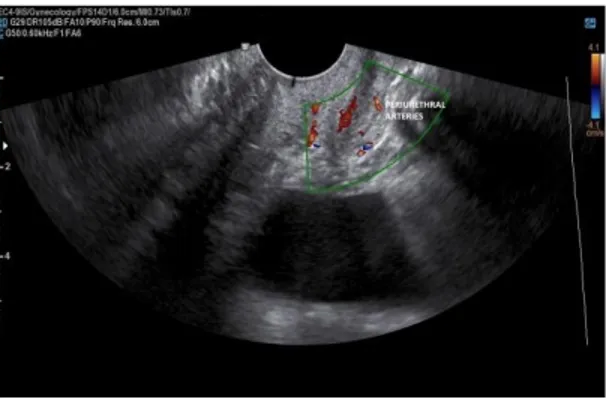
Postmenopozal Dönemdeki Kadınlarda Stres Üriner İnkontinans Tanısında Periüretral Doppler Ultrasonografi’nin Yeri
Tam metin
Şekil
Benzer Belgeler
Çalışmaya, 2010-2017 yılları arasında Ankara Numune Eğitim ve Araştırma Hastanesi Genel Cerrahi Kliniğinde hemoroidektomi sonrası spesmenlerin histopatolojik incelemesi
[72] Buna karşın çalışmamızın sonuçlarına göre postmenopozal dönemde olan kadınların fiziksel aktivite seviyesi, emosyonel reaksiyonları ile birlikte yaşam
Keywords: Stress urinary incontinence, vaginal cone therapy, transobturator tape, conservative treatment.. 1 University of Health Siences, Etlik Zübeyde Hanım Maternity and
We retrospectively examined the patients’ urodynamics, ultrasonography, demographic characteristics, incontinency surveys, life quality scores [incontinence impact
Genç üstün bilgili Zeki Kuneralp’in aldı ğı neticeyi Cumhurbaşkanı İnönü’ye arzeden ve kalet mensuplarına büyük devlet adamı; “Bu de ğerli gencin
Ezetimibe(本院商品名:Ezetrol 10mg) 干擾膽固醇穿過腸道障壁以抑制膽固醇吸收。 僅可降低約 17% 的低密度脂蛋白,通常與
İki tane triazol halkası ve iki tane metil bağlı kumarin grubu taşıyan 5e bileşiğinin metal iyonlarının varlığında monomer emisyon şiddeti azalırken,
Sexually active respondents completed the short form of the Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ-12).. MAIN OUTCOME MEASURE: PISQ-12 and
