Comparison of the effect of single lumbar transforaminal epidural steroid ınjections for the treatment of L4-5 and L5-S1 paramedian disc herniation
Tam metin
Şekil

Benzer Belgeler
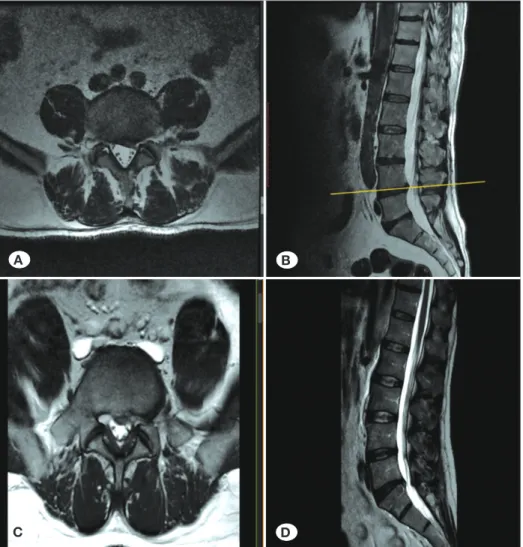
According to the terminology developed by the ‘’International Society for the Study of the Lumbar Spine’’ the radiological staging of the lumbar disc herniation is defined
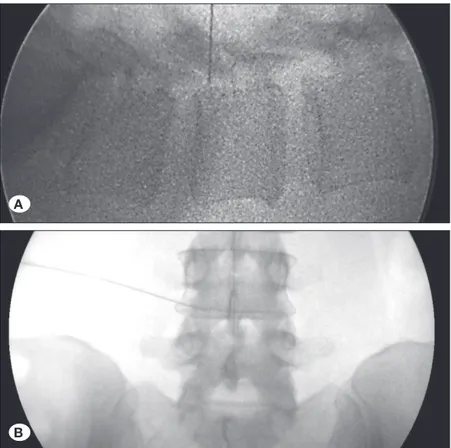
Bu çalışmada, konservatif tedavi yöntemleri ya da cerrahi tedaviyle iyileşmeyen bel ağrısı şikayeti olan hastalara uyguladığımız lomber TFESE tedavisinin
We aimed to emphasize that lumbar disc pathologies may cause new onset pain in the patients with amputated limb and should importantly take a place in the differential diagnosis
Introduction: Our aim was to evaluate the relationship between lumbar multifidus (LM) muscle atrophy and lumbar disc herniation by magnetic resonance imaging (MRI) findings
Aim: The aim of this study is to examine the safety and efficacy of the Percutaneous Laser Disc Decompression which is applied to patients with lower back pain and radiculopathy
In this study which aimed two different applications of traction as a physical therapy method in patients with subacute lumbar disc hernia on the effect of pain, clinical
Conclusion: Although risk of recurrence in lumbar disc hernia depends on many factors, possibility to develop recurrent disc hernia of the patients who have larger annular
5000’den fazla insanın ölümüne sebep olduğu için Dünya Sağlık Örgütü tarafından 11 Mart 2020 tarihinde pandemik hastalık olarak ilan edilmiştir.. Bu ilanın ardından
