https://doi.org/10.1007/s00403-018-1867-z ORIGINAL PAPER
Visfatin and insulin levels and cigarette smoking are independent risk
factors for hidradenitis suppurativa: a case–control study
Neslihan Akdogan1 · Nuran Alli1 · Pinar Incel Uysal1 · Canan Topcuoglu2 · Tuba Candar3 · Turan Turhan2 Received: 5 July 2018 / Revised: 4 September 2018 / Accepted: 1 October 2018 / Published online: 6 October 2018
© Springer-Verlag GmbH Germany, part of Springer Nature 2018
Abstract
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease. HS has been associated with obesity, adipokine imbalance, dyslipidemia, pro-inflammation, and metabolic syndrome (MS). The aim of this study was to determine the association between HS, and serum visfatin levels (SVLs), small-dense low-density lipoprotein cholesterol (sdLDL-C), and ischemia-modified albumin (IMA), as well as the association between HS, and smoking, alcohol consumption, anthropometric measurements, blood pressures (BPs), fasting blood glucose (FBG) and lipids, inflammatory markers, homocysteine, uric acid (UA), serum insulin levels (SILs), insulin resistance (IR) and MS, so as to identify relevant risk factors for HS. This case–control study included 40 patients (M/F: 23/17) and 40 age- and gender-matched controls (M/F: 23/17). Demographic data, smoking status and alcohol consumption, personal and family medical history, previous and current treatments were noted. Anthropometric data, BPs, FBG and lipids, homocysteine, UA, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and high-sensitivity CRP (hs-CRP), hemoglobin A1c (HbA1c), SILs, SVLs, IMA and sdLDL-C were meas-ured. Homeostasis model assessment for IR (HOMA-IR) was calculated. The associations were made by univariate and multivariate analyses. Univariate analysis showed that there was a significant association between HS and smoking, pack-years of smoking, weight, body mass index (BMI), waist circumference (WC), triglycerides (TGs), high-density lipoprotein cholesterol, very low-density lipoprotein cholesterol, SILs, CRP, hs-CRP, homocysteine, UA, ESR, HOMA-IR, SVLs, and MS. After adjusting for BMI and smoking status, the SVLs, SILs, and hs-CRP levels remained higher in the patients than in the controls (P = 0.02, P = 0.01, and P = 0.02, respectively). Multivariate analysis showed that there was a significant association between HS, and the SVLs and SILs, and smoking. Each unit increase in the SVL (P = 0.003, 95% CI 1.16–2.11) and SIL (P = 0.03, 95% CI 1.01–1.17) increased the risk of HS 1.56- and 1.09-fold, respectively. Furthermore, smoking was associated with a 14.87-fold increase in the risk of HS (P = 0.001, 95% CI 2.82–78.56). This study indicates that HS patients have higher SVLs, SILs, and hs-CRP levels than healthy controls—independent of BMI and smoking status. The SVL and SILs and smoking were independent risk factors for HS.
Keywords Hidradenitis suppurativa · Visfatin · Insulin · Smoking
Introduction
Hidradenitis suppurativa (HS) is a chronic inflamma-tory skin disease which can present as recurrent nodules, abscesses, and sinus tracts [33]. The etiopathogenesis of HS is not precisely known; however, follicle-associated factors, genetic factors, hormones, autoinflammation, and microbial factors are known to play a role [26]. HS is associated with several conditions, including obesity, cigarette smoking, and metabolic syndrome (MS) [22]. Accordingly, beyond its role in regulating energy, adipose tissue, which exhib-its changes in obesity, also functions as an endocrine organ via its production of adipocytokines [1]. Several adipokines
* Neslihan Akdogan [email protected]
1 Department of Dermatology and Venereology, Ankara
Numune Education and Research Hospital, Talatpaşa Street, No:44, Altındağ, 06100 Ankara, Turkey
2 Department of Medical Biochemistry, Ankara Numune
Training and Research Hospital, Ankara, Turkey
3 Department of Medical Biochemistry, Faculty of Medicine,
with proinflammatory effects, such as leptin, resistin, and visfatin, are secreted by adipose tissue [1]. In addition to proinflammatory effects, visfatin has insulin-like properties; it binds to the insulin receptor which is why some think there could be a relationship between visfatin and MS [7]. Vis-fatin is a biomarker or a factor posited to be associated with obesity, inflammation, and insulin resistance (IR) [6]. Adi-pokine expression is dysregulated in obesity; however, it is not clearly known if adipokine levels are altered in patients with HS. A recent study observed adipokine imbalance in HS patients, even though visfatin was not evaluated in this study [17]. In accordance with visfatin’s insulin-like fea-tures, and its association with IR and MS, it might be helpful to know if there is a difference in the serum visfatin level (SVL) between HS patients and healthy controls.
HS is now considered to be a systemic inflammatory dis-ease extending beyond the skin, with a substantial comor-bidity burden. The risk of atherosclerosis, cardiovascular disease (CVD), and major adverse cardiovascular events is increased in HS [3, 30, 31]. Although the role of lipid frag-ments in HS-associated atherosclerosis and dyslipidemia has been reported, the role of the atherogenic particles low-density lipoprotein cholesterol (LDL-C) and small dense low-density lipoprotein cholesterol (sdLDL-C) in HS is yet to be investigated. Furthermore, homocysteine—an amino acid produced from methionine—is associated with CVD, cerebrovascular disease, venous thromboembolism, and peripheral vascular disease via its role in the promotion of thrombosis, oxidant stress, apoptosis, and cellular prolif-eration [18]. As homocysteine is considered an independ-ent risk factor for CVD, idindepend-entification of any relationship between homocysteine and HS could be clinically relevant [28]. Moreover, ischemia-modified albumin (IMA), which results from modification of free albumin in the presence of atherosclerotic conditions, is considered a biomarker that could be important for the detection of ischemia and oxi-dative stress in several endocrine diseases such as diabe-tes mellitus (DM), polycystic ovary syndrome (PCOS) and hypothyroidism [23]. Contraction of vessels induced by atherosclerosis causes hypoxia or ischemia, which leads to formation of IMA [14]. Moreover, recent data showed that serum uric acid (UA) concentration might be predictive of the development of MS, DM, hypertension (HT), kidney disease, and CVD, as UA has a negative effect on adipocytes via promotion of inflammation and nitric oxide production, and induction of platelet aggregation [27].
In accordance with the findings outlined above, the pre-sent study aimed to determine the association between HS, and SVLs, sdLDL-C, and IMA, as well as the association between HS, and smoking, alcohol consumption, anthro-pometric measurements, blood pressure, plasma lipid and glucose levels, inflammatory markers, serum insulin levels (SILs), homocysteine, UA, IR, and MS, so as to identify relevant risk factors for HS.
Materials and methods
The study included 40 patients (M/F: 23/17) and 40 age- and gender-matched controls (M/F: 23/17) that met the inclusion criteria. The participants were recruited from the outpatient dermatology clinic of Ankara Numune Training and Research Hospital between December 2016 and Janu-ary 2018. Inclusion criteria were age ≥ 18 years, a negative history of cancer, and voluntarily agreeing to participate. The diagnosis of HS was confirmed by dermatologists, according to the Dessau definition [15]. Exclusion criteria were age ≤ 18 years, pregnancy, lactation, active or chronic infection, and current use of antihyperlipidemic treatment. Patients and controls were matched for age, gender, DM, HT, coronary artery disease (CAD), inflammatory arthri-tis (rheumatoid arthriarthri-tis or ankylosing spondyliarthri-tis), and hypothyroidism.
Demographic data, including age, gender, personal and family medical history, cigarette smoking status, alco-hol consumption, engagement in regular physical activ-ity (defined as exercise for ≥ 45 min per day 3 times per week), and family history of premature (age ≤ 49 years) CVD were recorded for all participants. Duration of dis-ease, previous and current treatment agents, and lesion localization (defined as axillae, inguinal, groin, ano-genital, submammary, and intermammary) were noted. Disease severity was based on Hurley staging (Table 1) and HS Physician’s Global Assessment (PGA) (Table 2) [33]. Waist circumference (WC) (cm), height (m), weight (kg), and BMI (kg m−2) were recorded. BMI was
meas-ured using the Quetelet Index [4], and cut-off points for BMI and WC are shown in Table 3 [32]. MS was defined according to the 2006 International Diabetes Federation Report(1)(Table 4) [13]. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in each participant using a blood pressure monitor (ERKA, The Original, VARIO, blood pressure monitor, Germany) Table 1 A severity classification
of hidradenitis suppurativa, Hurley staging
Stage I Abscess formation, single or multiple, without sinus tracts and cicatrization Stage II Recurrent abscesses with tract formation and cicatrization, single or
multi-ple, widely separated lesions
Stage III Diffuse or near-diffuse involvement, or multiple interconnected tracts and abscesses across the entire area
following at least 10 min of rest. Laboratory measurements included the serum lipid profile (SLP)—total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), very low-den-sity lipoprotein cholesterol (VLDL-C), and triglycerides (TG), fasting blood glucose (FBG), C-reactive protein (CRP), high-sensitivity CRP (hs-CRP), UA, the erythro-cyte sedimentation rate (ESR), homocysteine, hemoglobin A1c (HbA1c), SILs, SVLs, and sdLDL-C and IMA. The homeostasis model of assessment-IR (HOMA-IR) (mass units) was calculated using the following formula: fasting insulin (mIU L−1) × fasting glucose (mg dL−1)/405.
Assays
After 8 h of fasting 10 mL of peripheral venous blood was collected from each participant. FBG, TC, TG, HDL-C, and UA levels were measured via the enzymatic method, whereas the LDL-C level was calculated using the Friede-wald formula (LDL-C = TC–HDL-C − TG/5.0). CRP (Roche Diagnostics, Mannheim, Germany) and the hs-CRP (Beck-man Coulter AU5800, Beck(Beck-man Coulter Inc., USA) level were calculated via the immunoturbidimetric method. The SIL was measured via electrochemiluminescence immu-noassay using a Cobas e601 analyzer (Roche Diagnostics, Mannheim, Germany) and homocysteine was measured via Table 2 Six stage Physician’s Global Assessment for hidradenitis suppurativa
Clear (score = 0) No inflammatory nodules, no noninflammatory nodules, no abscesses, no draining fistulas
Minimal (score = 1) Only the presence of noninflammatory nodules in the absence of abscesses, draining fistulae or inflammatory nodules Mild (score = 2) < 5 inflammatory nodules or 1 abscess or draining fistula and no inflammatory nodules
Moderate (score = 3) No abscesses, no draining fistulas, and ≥ 5 inflammatory nodules; or 1 abscess or draining fistula and ≥ 1 inflamma-tory nodule; or 2–5 abscesses or draining fistulas and < 10 inflammainflamma-tory nodules
Severe (score = 4) 2–5 abscesses or draining fistulas and ≥ 10 inflammatory nodules Very severe (score = 5) > 5 abscesses or draining fistulas
Table 3 Cut-off points for body mass index and waist circumference according to World Health Organization Adapted from ‘Waist Circumfer-ence and Waist-Hip Ratio, Report of a World Health Organization Expert Consultation, December 2008 [32]
BMI body mass index WC Waist circumference
BMI (kg m−2) Obesity class
Underweight < 18.5
Normal 18.5–24.9
Overweight 25.0–29.9
Obesity 30.0–34.9 I
35.0–39.9 II
Extreme obesity > 40.0 III
WC (cm) Risk of
meta-bolic complica-tions
Men ≥ 94 Increased
Women ≥ 80 Increased
Table 4 Metabolic syndrome definition according to 2006 report of International Diabetes Federation [13]
WC Waist circumference, HDL-C High density lipoprotein cholesterol
a WC does not need to be calculated and central obesity can be supposed when BMI is > 30 kg m−2
1. Central obesity (WCa for men ≥ 94 cm and for women ≥ 80 cm) plus any two of the following four factors
1. Fasting plasma glucose ≥ 100 mg/dL (or receiving drug therapy for hyperglycemia)
2. Systolic blood pressure ≥ 130 or diastolic blood pressure ≥ 85 mmHg (or receiving drug therapy for hypertension) 3. Triglycerides ≥ 150 mg/dL (or receiving drug therapy for hypertriglyceridemia)
chemiluminescent immunoassay using an Immulite 2000 XPi (Siemens Healthcare Diagnostics, UK). HbA1c was measured via ion-exchange high-pressure liquid chromatog-raphy using an ADAMS A1c HA-8180V automated glyco-hemoglobin analyzer (Arkray Global Business, Inc., Kyoto, Japan). ESR was calculated using an ALI FAX® TEST1 THL analyzer (ALIFAX Srl, Polverara, Italy) via measure-ment of the kinetics of red cell aggregation.
Sera obtained after centrifugation of blood samples at 1200g (g = relative centrifugal force) for 10 min were used to measure visfatin, sdLDL-C, and IMA. Serum samples were stored at − 80 °C until analysis. The SVL was calculated via the Sandwich ELISA method using the commercially available ElabScience Kit (Elabsci-ence Biotechnology Co. Ltd., WuHan, P.R.C., Catalog no. E-EL-H1763, LOT: AK0017NOV20092), according to the manufacturer’s instructions. The kit has a detection range of 0.31–20 ng mL−1 and a sensitivity of 0.19 ng mL−1.
The IMA level was calculated by measuring the complex composed of dithiothreitol and cobalt (Sigma-Aldrich VR, St Louis, MO) (unbound to albumin) via the colorimetric method using a spectrophotometer. Absorbance of speci-mens was spectrophotometrically assayed at 470 nm using a spectrophotometer (HumaLyzer Photometers, Humalyzer 2000, Human Diagnostics, Wiesbaden, Germany) and the results were given as absorbance units (ABSU). The sdLDL-C level was measured via a 2-step automated colorimetric method using an Abbott c8000 analyzer. The first step was to precipitate the lipoprotein with a density < 1.044 g mL−1
using heparin-magnesium and the second step was direct LDL-C determination based on the supernatant fraction.
Statistical analysis and ethics
Statistical analysis was performed using IBM SPSS Statis-tics for Windows v.21.0. (IBM Corp., Armonk, NY). Data are shown as mean ± SD or median (range), as appropriate. The Shapiro–Wilk test was used to determine the normality of the distribution of numeric variables. When parametric assumptions were met, the independent sample t test was used to compare numeric variables between patients and controls, and the Mann–Whitney U test was used to com-pare numeric variables when parametric assumptions were not met. The Chi-square test was used to compare between-group differences in categorical variables. Relationships between the numeric variables were determined using Spearman’s correlation coefficient. Non-parametric Quade ANCOVA was used to verify the effect of variables on HS with adjustments for BMI and smoking. Multivariate logistic regression analysis was used to determine the association between HS and the study parameters after elimination of confounding factors. The strength of the association between the study parameters and HS risk was assessed via the odds
ratio (OR) and the corresponding 95% confidence interval (CI). The level of statistical significance was set at P < 0.05.
The study protocol was approved by the Ankara Numune Training and Research Hospital Ethics Committee (code E-16-1089, 14 December 2016). All study procedures were performed in accordance with the ethical principles of the 1964 Declaration of Helsinki, and all the participants pro-vided written informed consent.
Results
The clinical data and demographic features of the partici-pants are listed in Tables 5 and 6. The study included 40 patients with HS (M/F: 23/17) and 40 healthy controls (M/F: 23/17). Patients and controls were similar in terms of age, gender, and systemic diseases mentioned above. Median disease duration was 74 months (range 1–300). In all, 19 patients were currently using medication for HS, includ-ing primarily oral retinoids and oral antibiotics, whereas 21 patients were not.
Univariate analysis showed that there was not any sig-nificant association between HS and the investigated param-eters, including alcohol consumption, regular physical activ-ity, family history of premature CVD, height, SBP, DBP, FBG, TC, LDL-C, HbA1c, sdLDL-C, and IMA. Addition-ally, there was a significant association between HS, and cigarette smoking, pack-years of cigarette smoking, MS, weight, BMI, WC, TG, HDL-C, VLDL-C, SILs, CRP, hs-CRP, homocysteine, UA, ESR, HOMA-IR, and SVLs. The patient group had significantly higher levels of these param-eters that were significantly associated with HS, except HDL-C, than the control group (Table 5). After adjusting for BMI and smoking status, the SVLs, SILs, and hs-CRP levels remained higher in the patients than in the controls (P = 0.02, P = 0.01, and P = 0.02, respectively). Addition-ally, after correction for BMI and smoking, there was an association between HS, and LDL-C, CRP, and HOMA-IR based on univariate analysis; however, these associations only approached borderline significance (P = 0.05, P = 0.05, and P = 0.05, respectively) (Table 7).
There was a weak negative correlation between the SVL, and the CRP or hs-CRP level across the patient group (rs:
− 0.386, P = 0.01 and rs:−0.352, P = 0.03, respectively), although there was not a significant correlation between the SVL, and Hurley stage, PGA, or disease duration. There was no difference in the SVL between the patients that were currently receiving treatment for HS and those that were not (P = 0.60). In addition, there was a weak positive cor-relation between the SVL and UA in the control group (rs:
0.389, P = 0.01).
Multivariate logistic regression analysis showed that there was a significant association between HS, and the
Table 5 Comparisons of parameters in patients with hidradenitis suppurativa and controls by univariate analysis
Parameter Patients (n = 40) (%) Controls (n = 40) (%) Normal range P value
Ageb (years) 35.43 ± 11.23 35.40 ± 11.43
Gender (male/female) 23/17 23/17
Cigarette smoking status < 0.001
Current smoker 33 (82.5%) 15 (37.5%)
Ex-smoker 1 (2.5%) 5 (12.5%)
Never smoked 6 (15%) 20 (50%)
Pack-years of cigarette smokinga 10 (0–40) 0.5 (0–30) 0.001
Engagement in regular physical activity 0.06
Yes 3 (7.5%) 9 (22.5%)
No 37 (92.5%) 31 (77.5%)
Family history of premature CVD 0.45
Yes 12 (30%) 9 (22.5%)
No 28 (70%) 31 (77.5%)
Alcohol consumption 0.25
Once a month, two beers 2 (5%) 0 (0%)
Twice a week, two beers 2 (5%) 1 (2.5%)
Once a week, six glasses of Turkish raki 1 (2.5%) 0 (0%) Thrice a week, three glasses of Turkish raki 0 (0%) 2 (5%)
None 35 (87.5%) 37 (92.5%) Metabolic syndrome 0.002 Yes 20 (50%) 7 (17.5%) No 20 (50%) 33 (82.5%) Heightb (cm) 0.24 Men 176.2 ± 7.5 174.1 ± 7.6 Women 164.3 ± 8.5 163.0 ± 6.8 Weighta (kg) < 0.001 Men 88.5 (55–193) 78.0 (53–99) Women 80.0 (58–130) 58.0 (50–82) BMIa, c (kg m− 2) < 0.001 Men 28.7 (17.8–56.4) 24.9 (18.6–33.9) Women 29.3 (22.6–46.1) 20.8 (17.7–34.1) WCa, c(cm) 0.001 Men 99 (67–160) 93 (70–133) Women 104 (76–127) 75 (64–110) Blood pressurea (mmHg) SBP 120 (90–150) 116.5 (90–135) 90–120 0.37 DBP 75 (50–90) 70 (40–90) 60–80 0.67 FBGa (mg/dL) 93.5 (79–248) 90.0 (73–412) 74–109 0.48 TGsa (mg/dL) 145.5 (52–335) 97.5 (38–385) 0–200 0.004 TCa (mg/dL) 178 (104–267) 177 (12–308) 0–200 0.32 LDL-Ca (mg/dL) 104 (54–187) 105.5 (60–184) 0–100 0.98 HDL-Ca (mg/dL) 42.98 (22–73) 51.1 (16–89) 40–60 0.009 VLDL-Ca (mg/dL) 29.0 (10–67) 20 (8.2–77) 0–40 0.009 Insulina (µU/mL) 15.67 (3.75–42.81) 9.57 (1.33–59.52) 2.6–24.9 < 0.001 CRPa (mg/dL) 6.5 (0.3–79) 2.0 (0.2–27) 0–5 < 0.001 hs-CRPa(mg/L) 6.26 (0.29–82.24) 1.18 (0.18–28.42) 0–3 < 0.001 Homocysteinea(umol/L) 12.8 (7.89–72.7) 11.85 (4.77–22.3) 0–12 0.049 UAb (mg/dL) 5.67 ± 1.20 4.72 ± 1.48 3.4–7 0.001 ESRa (mm/h) 15.5 (2–84) 6.5 (2–35) 0–20 0.001 HbA1ca (%) 5.7 (4.7–12.9) 5.35 (4.8–15) 4–6.2 0.06
SVLs and SILs, and smoking. Each unit increase in the SVL (P = 0.003, 95% CI 1.16–2.11) and SIL (P = 0.03, 95% CI 1.01–1.17) increased the risk of HS 1.56-fold and 1.09-fold, respectively. Furthermore, smoking was associated with a 14.87-fold increase in the risk of HS (P = 0.001, 95% CI 2.82–78.56); therefore, the SVLs and SILs, and smoking were considered independent risk factors for HS (Table 8).
Based on univariate analysis there was an association between HS and MS (P = 0.002). According to multivariate logistic regression analysis, there was a significant associa-tion between MS, and study group (patient/control), age, UA, and IMA (Table 9). Additionally, univariate analysis revealed that there was no significant difference between patients receiving active therapy for HS and those not receiving active therapy in terms of the parameters studied except HDL-C and gender. Median serum HDL-C levels were higher in patients who were not receiving active ther-apy for HS compared with patients receiving active therther-apy (P = 0.02). There was an association between gender and the status of receiving active therapy for HS (P = 0.049).
Discussion
Visfatin is an adipokine that is secreted from visceral adi-pose tissue. It exhibits insulin-like properties which may be why some think there is an association between visfatin and MS [7]. Additionally, visfatin plays a role in pro-inflamma-tion and atherosclerotic plaque destabilizapro-inflamma-tion [2]. Elevated SVLs is associated with endothelial inflammation, and an increase in oxidative stress and proinflammatory cytokine levels [19]. The SVL was reported to be high in patients with such inflammatory conditions as colonic tissue of Crohn’s and ulcerative colitis [21], macrophages of human unstable
carotid and coronary atherosclerosis [2], acute myocardial infarction [12], rheumatoid arthritis [16], cancer [11], and psoriasis [9], and diseases associated with IR, including DM [24], MS [5], and PCOS [29]. Esteghamati et al. [5] posited that visfatin might be an indicator predictive of MS. Although there is no study evaluating the role of visfatin in HS, Malara et al. showed an adipokine imbalance regardless of SVLs in HS. As such, the present study is the first study to determine the role of SVLs in HS [17]. The present study observed that patients with HS had a significantly higher SVL—independent of BMI and smoking status—than con-trols. The high SVL in HS patients regardless of BMI could be considered to support the idea that this adipokine con-stitutes a relevant parameter for HS subgroups with a low and high BMI phenotype. Moreover, the SVL might be an independent risk factor for HS and an elevated SVL may predispose individuals to the development of HS. Additional research is needed to further clarify visfatin’s functions, pre-cise role, and clinical and therapeutic significance, so as to discern if this adipokine can improve our attitude in HS and be used as a biomarker in clinical practice.
Indications for elevated SIL and IR in HS can be men-tioned. Although the association between HS, and elevated SILs and IR is dependent upon a high BMI in HS patients, this association remained significant even after adjusting for BMI in some studies [31]. The present study’s findings also show that patients with HS had a significantly higher SIL— independent of BMI and smoking status—than the controls, and increase in the SIL increased the risk of HS. The level of significance of the relationship between HS and HOMA-IR might have been higher had the present study included a larger study population, as the relationship was only bor-derline significant after adjustments for BMI and smoking. These findings suggest that insulin might be an independent n number, CVD cardiovascular disease, BMI body mass index, WC waist circumference, SBP systolic blood pressure, DBP diastolic blood
pres-sure, FBG fasting blood glucose, LDL-C low-density lipoprotein cholesterol, HDL-C high-density lipoprotein cholesterol, VLDL-C very low density lipoprotein cholesterol, HOMA-IR homeostasis model of assessment-insulin resistance, CRP C-reactive protein, hs-CRP high-sensitivity C-reactive protein, UA uric acid, HbA1c hemoglobin A1c; ESR erythrocyte sedimentation rate, sdLDL-C small-dense low density lipoprotein cholesterol, IMA Ischemia-modified albumin, ABSU absorbance unit
P < 0.05 is defined statistically significant and shown in bold
a Median (range) values
b Shows mean ± standard deviation results
c Normal ranges for BMI and WC are shown at Table 3
Table 5 (continued)
Parameter Patients (n = 40) (%) Controls (n = 40) (%) Normal range P value
HOMA-IRa (mass units) 4.31 ± 3.69 2.17 ± 1.46 normal IR:<3
Moderate IR:3–5 severe IR:>5 0.001 Visfatina (ng/mL) 3.38 (0.03–11.57) 1.86 (0.19–8.54) 0.02 SdLDL-Ca (mg/dL) 46 (27–104) 47.5 (26–104) 0.72 IMAa (ABSU) 0.72 (0.26–1.72) 0.71 (0.19–1.77) 0.86
risk factor for the development of HS. Accordingly, we think that all HS patients should be screened for the SIL. In terms of the insulin-mimetic effects of visfatin, it is possible that visfatin and insulin have synergistic effects on HS, as both visfatin and insulin were significantly associated with HS in the present study. The effects of various therapeutic agents on the SIL, the precise role of insulin in the pathogenesis of HS, the effect of weight loss on the SVLs and SILs, and
the consequent effects on the risk of HS, disease severity, and treatment response should be investigated in prospec-tive studies.
Smoking might also be considered a potential risk factor for HS. A meta-analysis published in 2015 by Tzellos et al. [30] observed that there is a close association between HS and smoking. A retrospective cohort analysis of 3,924,310 smokers showed that the overall likelihood of a new diag-nosis of HS among smokers is 1.90-fold higher than among nonsmokers [8]. Active cigarette smoking increased the risk of HS and there was a significant association between HS, and smoking or pack-years of cigarette smoking in the Table 6 Disease characteristics, previous and current treatment
agents, classification of patients according to Hurley staging and Phy-sician’s Global Assessment
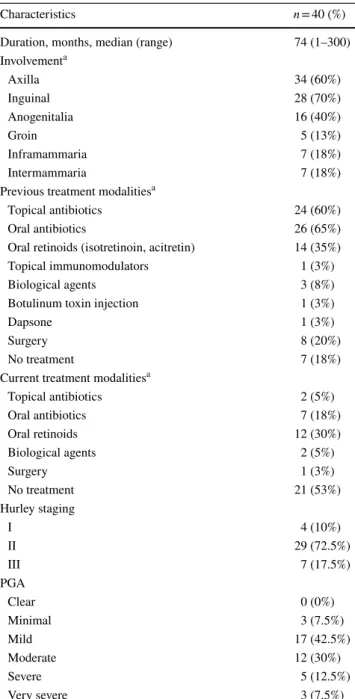
n number, PGA Physician’s Global Assessment
a Patients may experience more than one area of involvement as well
as more than one type of previous and current treatments
Characteristics n = 40 (%)
Duration, months, median (range) 74 (1–300) Involvementa Axilla 34 (60%) Inguinal 28 (70%) Anogenitalia 16 (40%) Groin 5 (13%) Inframammaria 7 (18%) Intermammaria 7 (18%)
Previous treatment modalitiesa
Topical antibiotics 24 (60%)
Oral antibiotics 26 (65%)
Oral retinoids (isotretinoin, acitretin) 14 (35%)
Topical immunomodulators 1 (3%)
Biological agents 3 (8%)
Botulinum toxin injection 1 (3%)
Dapsone 1 (3%)
Surgery 8 (20%)
No treatment 7 (18%)
Current treatment modalitiesa
Topical antibiotics 2 (5%) Oral antibiotics 7 (18%) Oral retinoids 12 (30%) Biological agents 2 (5%) Surgery 1 (3%) No treatment 21 (53%) Hurley staging I 4 (10%) II 29 (72.5%) III 7 (17.5%) PGA Clear 0 (0%) Minimal 3 (7.5%) Mild 17 (42.5%) Moderate 12 (30%) Severe 5 (12.5%) Very severe 3 (7.5%)
Table 7 Comparisons of parameters in patients with hidradenitis sup-purativa and in controls after adjustments for body mass index and active smoking
hs-CRP high-sensitivity C-reactive protein, CRP C-reactive protein, LDL low-density lipoprotein cholesterol, HOMA-IR homeostasis
model of assessment-insulin resistance
P < 0.05 is defined statistically significant and shown in bold
* Borderline significant differences
Variable P value
Serum visfatin (ng/mL) 0.02
Serum insulin (µU/mL) 0.01
Serum hs-CRP (mg/L) 0.02
Serum CRP (mg/L) 0.05*
Serum LDL-C (mg/dL) 0.05*
HOMA-IR (mass units) 0.05*
Table 8 Multivariate logistic regression analysis for variables in patients with hidradenitis suppurativa and controls
OR odds ratio, CI confidence interval
P < 0.05 is defined statistically significant and shown in bold
Variable OR (95% CI) P value
Serum visfatin levels (ng/mL) 1.56 (1.16–2.11) 0.003 Serum insulin levels (µU/mL) 1.09 (1.01–1.17) 0.03
Active smoking 14.87 (2.82–78.56) 0.001
Table 9 Multivariate logistic regression analysis for variables in par-ticipants with metabolic syndrome and in parpar-ticipants without meta-bolic syndrome
OR odds ratio, CI confidence interval, UA uric acid, IMA
ischemia-modified albumin
P < 0.05 is defined statistically significant and shown in bold
Variable OR (95% CI) P value
Group (patient/control) 6.54 (1.80–23.75) 0.004
Age 1.06 (1.01–1.12) 0.03
UA (mg/dL) 2.13 (1.27–3.56) 0.004
present study; therefore, we think HS patients should be strongly encouraged to quit smoking. Larger scale studies that include prospectively paired individuals are needed to further clarify the effects of smoking on the pathogenesis of HS, and the therapeutic response and long-term follow-up of HS.
The role of increased pro-inflammation in the pathogene-sis of HS remains the subject of investigation. An increase in the serum TNF-α concentration, and upregulation of IL-1β, IL-23, and IL-17 in HS lesions indicate that inflammatory response and cytokines play a role in the pathogenesis of HS [22]. In the present study, there was a marked increase in the serum hs-CRP level—independent of BMI and smok-ing status—in the HS patients, as compared to the controls, which suggests an increased trend toward pro-inflammation. Moreover, the utility of hs-CRP measurement in the estima-tion of prognosis, disease severity, and or treatment response in patients with HS and potential targets for reducing the hs-CRP level should be determined via additional larger scale prospective studies.
The present findings suggest there is an association between HS and MS. Although the present study matched the HS patients and control in terms of age, gender, DM, and HT, the discrepancy in frequency of MS might have been due to differences in obesity and WC rates, and lipid levels between the patients and controls. Earlier studies reported a significant association between HS and MS [20, 25]. Gold et al. [10] observed that the prevalence of MS in HS patients was 50.6%, versus 30.2% in controls. The researchers attrib-uted this difference to differences in the rate of obesity, the TG level, and glucose abnormalities between the two groups, even though blood pressure and the HDL-C level did not dif-fer. We think that dermatologists should be made aware of the relationship between HS and MS, and screen HS patients accordingly.
The present study has some limitations, including a small study sample, gender imbalance (more males than females), and a case–control design. As the study was conducted at a single research center, generalization of the findings is not warranted. In addition, causality could not be evaluated due to the study’s case–control design. Furthermore, the serum IMA concentration measurements were not corrected by albumin concentrations. Moreover, it was not determined if any of the participants were using such medications as folic acid and B vitamins that affect the plasma homocysteine level. Despite these limitations, we think the study’s findings offer new insights into the association between HS, and the SVLs, SILs, and hs-CRP levels, and smoking status which might pave the way to novel approaches to the treatment of HS patients.
In conclusion, the present findings indicate that HS patients have higher SVLs, SILs, and hs-CRP levels than healthy controls—independent of BMI and smoking status.
The SVL and SILs, and smoking were observed to be inde-pendent risk factors for HS. Additional larger scale research is needed to further delineate the function, pathogenetic role, potential prognostic value, and clinical and therapeu-tic significance of the SVL and SILs, and smoking in HS patients. Clinicians should be made aware of the impor-tance of screening, detecting, and controlling these three factors in patients with HS, so as to minimize the incidence of comorbidity.
Funding This study was supported by Scientific Research Support Fund of Ankara Numune Training and Research Hospital on December 14, 2016 (Grant number: 2016/1089).
Compliance with ethical standards
Conflict of interest Author Neslihan Akdogan, Nuran Alli, Pinar Incel Uysal, Canan Topcuoglu, Tuba Candar and Turan Turhan declare that they have no conflict of interest.
Ethical approval The study protocol was approved by the Ankara Numune Training and Research Hospital Ethics Committee (code E-16-1089, 14 December 2016). All study procedures were performed in accordance with the ethical principles of the 1964 Declaration of Helsinki, and all the participants provided written informed consent.
References
1. Campanati A, Ganzetti G, Giuliodori K, Marra M, Bonfigli A, Testa R, Offidani A (2015) Serum levels of adipocytokines in psoriasis patients receiving tumor necrosis factor-alpha inhibitors: results of a retrospective analysis. Int J Dermatol 54(7):839–845 2. Dahl TB, Yndestad A, Skjelland M, Oie E, Dahl A, Michelsen A,
Damås JK, Tunheim SH, Ueland T, Smith C, Bendz B, Tonstad S, Gullestad L, Frøland SS, Krohg-Sørensen K, Russell D, Aukrust P, Halvorsen B (2007) Increased expression of visfatin in mac-rophages of human unstable carotid and coronary atherosclerosis: possible role in inflammation and plaque destabilization. Circula-tion 115(8):972–980
3. Egeberg A, Gislason GH, Hansen PR (2016) Risk of major adverse cardiovascular events and all-cause mortality in patients with hidradenitis suppurativa. JAMA Dermatol 152(4):429–434 4. Eknoyan G (2008) Adolphe Quetelet (1796–1874)—the average
man and indices of obesity. Nephrol Dial Transplant 23(1):47–51 5. Esteghamati A, Morteza A, Zandieh A, Jafari S, Rezaee M, Nakh-javani M, Jamali A, Esteghamati AR, Khalilzadeh O (2012) The value of visfatin in the prediction of metabolic syndrome: a multi-factorial analysis. J Cardiovasc Transl Res 5(4):541–546 6. Friebe D, Neef M, Kratzsch J, Erbs S, Dittrich K, Garten A,
Pet-zold-Quinque S, Blüher S, Reinehr T, Stumvoll M, Blüher M, Kiess W, Körner A (2011) Leucocytes are a major source of cir-culating nicotinamide phosphoribosyltransferase (NAMPT)/pre-B cell colony (PBEF)/visfatin linking obesity and inflammation in humans. Diabetologia 54(5):1200–1211
7. Fukuhara A, Matsuda M, Nishizawa M, Segawa K, Tanaka M, Kishimoto K, Matsuki Y, Murakami M, Ichisaka T, Murakami H, Watanabe E, Takagi T, Akiyoshi M, Ohtsubo T, Kihara S, Yamashita S, Makishima M, Funahashi T, Yamanaka S, Hira-matsu R, Matsuzawa Y, Shimomura I (2005) Visfatin: a protein
secreted by visceral fat that mimics the effects of insulin. Science 307(5708):426–430
8. Garg A, Papagermanos V, Midura M, Strunk A (2018) Incidence of hidradenitis suppurativa among tobacco smokers: a popu-lation-based retrospective analysis in the USA. Br J Dermatol 178(3):709–714
9. Gerdes S, Osadtschy S, Rostami-Yazdi M, Buhles N, Weichenthal M, Mrowietz U (2012) Leptin, adiponectin, visfatin and retinol-binding protein-4— mediators of comorbidities in patients with psoriasis? Exp Dermatol 21(1):43–47
10. Gold DA, Reeder VJ, Mahan MG, Hamzavi IH (2014) The preva-lence of metabolic syndrome in patients with hidradenitis sup-purativa. J Am Acad Dermatol 70(4):699–703
11. Grolla AA, Travelli C, Genazzani AA, Sethi JK (2016) Extra-cellular nicotinamide phosphoribosyltransferase, a new cancer metabokine. Br J Pharmacol 173(14):2182–2194
12. Grzywocz P, Mizia-Stec K, Wybraniec M, Chudek J (2015) Adi-pokines and endothelial dysfunction in acute myocardial infarc-tion and the risk of recurrent cardiovascular events. J Cardiovasc Med (Hagerstown) 16(1):37–44
13. International Diabetes Federation (2006) The IDF consensus worldwide definition of the metabolic syndrome. Brussels, Bel-gium: International Diabetes Federation. 2006. https ://www.pitt. edu/~super 1/Metab olic/IDF1.pdf
14. Kucuk A, Uslu AU, Arslan S, Balta S, Ozturk C, Uysal S, Yılmaz R, Sakız D, Kayrak M (2016) Ischemia-modified albumin and atherosclerosis in patients with familial Mediterranean fever. Angiology 67(5):456–460
15. Kurzen H, Kurokawa I, Jemec GB, Emtestam L, Sellheyer K, Giamarellos-Bourboulis E, Nagy I, Bechara FG, Sartorius K, Lap-ins J, Krahl D, Altmeyer P, Revuz J, Zouboulis CC (2008) What causes hidradenitis suppurativa? Exp Dermatol 17(5):455–456 16. Lee YH, Bae SC (2018) Circulating adiponectin and visfatin levels
in rheumatoid arthritis and their correlation with disease activity: a meta-analysis. Int J Rheum Dis 21(3):664–672
17. Malara A, Hughes R, Jennings L, Sweeney CM, Lynch M, Awdeh F, Timoney I, Tobin AM, Lynam-Loane K, Tobin L, Hogan A, O’Shea D, Kirby B (2018) Adipokines are dysregulated in patients with hidradenitis suppurativa. Br J Dermatol 178(3):792–793 18. Maron BA, Loscalzo J (2009) The treatment of
hyperhomocyst-einemia. Ann Rev Med 60:39–54
19. Mattu HS, Randeva HS (2013) Role of adipokines in cardiovas-cular disease. J Endocrinol 216(1):T17–T36
20. Miller IM, Ellervik C, Vinding GR, Zarchi K, Ibler KS, Knudsen KM, Jemec GB (2014) Association of metabolic syndrome and hidradenitis suppurativa. JAMA Dermatol 150(12):1273–1280 21. Moschen AR, Kaser A, Enrich B, Mosheimer B, Theurl M,
Niederegger H, Tilg H (2007) Visfatin, an adipocytokine with proinflammatory and immunomodulating properties. J Immunol 178(3):1748–1758
22. Prens E, Deckers I (2015) Pathophysiology of hidradenitis sup-purativa: an update. J Am Acad Dermatol 73(5 Suppl 1):S8–S11 23. Seshadri Reddy V, Bukke S, Munikumar M (2018) Elevated lev-els of the circulatory ischemia-modified albumin in patients with polycystic ovary syndrome: a meta-analysis. Gynecol Endocrinol 14:1–7
24. Shaker O, El-Shehaby A, Zakaria A, Mostafa N, Talaat S, Kat-siki N, Mikhailidis DP (2011) Plasma visfatin and retinol bind-ing protein-4 levels in patients with type 2 diabetes mellitus and their relationship to adiposity and fatty liver. Clin Biochem 44(17–18):1457–1463
25. Shalom G, Freud T, Harman-Boehm I, Polishchuk I, Cohen AD (2015) Hidradenitis suppurativa and metabolic syndrome: a com-parative cross-sectional study of 3207 patients. Br J Dermatol 173(2):464–470
26. Smith MK, Nicholson CL, Parks-Miller A, Hamzavi IH (2017) Hidradenitis suppurativa: an update on connecting the tracts. F1000Res 6:1272
27. Soltani Z, Rasheed K, Kapusta DR, Reisin E (2013) Potential role of uric acid in metabolic syndrome, hypertension, kidney injury, and cardiovascular diseases: is it time for reappraisal? Curr Hypertens Rep 15(3):175–181
28. Sun K, Song J, Liu K, Fang K, Wang L, Wang X, Li J, Tang X, Wu Y, Qin X, Wu T, Gao P, Chen D, Hu Y (2017) Asso-ciations between homocysteine metabolism related SNPs and carotid intima-media thickness: a Chinese sib pair study. J Thromb Thrombolysis 43(3):401–410
29. Sun Y, Wu Z, Wei L, Liu C, Zhu S, Tang S (2015) High-visfatin levels in women with polycystic ovary syndrome: evidence from a meta-analysis. Gynecol Endocrinol 31(10):808–814
30. Tzellos T, Zouboulis CC, Gulliver W, Cohen AD, Wolkenstein P, Jemec GB (2015) Cardiovascular disease risk factors in patients with hidradenitis suppurativa: a systematic review and meta-anal-ysis of observational studies. Br J Dermatol 173(5):1142–1155 31. Vilanova I, Hernandez JL, Mata C, Duran C, Garcia-Unzueta
MT, Portilla V, Fuentevilla P, Corrales A, González-Vela MC, González-Gay MA, Blanco R, González-López MA (2018) Insu-lin resistance in hidradenitis suppurativa: a case–control study. J Eur Acad Dermatol Venereol 32(5):820–824
32. World Health Organization (2008) Waist circumference and waist-hip ratio: report of a WHO expert consultation, Geneva, 8–11 December 2008. World Health Organization, Geneva. http://www. who.int/iris/handl e/10665 /44583
33. Zouboulis CC, Del Marmol V, Mrowietz U, Prens EP, Tzellos T, Jemec GB (2015) Hidradenitis suppurativa/acne inversa: crite-ria for diagnosis, severity assessment, classification and disease evaluation. Dermatology 231(2):184–190
![Table 3 Cut-off points for body mass index and waist circumference according to World Health Organization Adapted from ‘Waist Circumfer- Circumfer-ence and Waist-Hip Ratio, Report of a World Health Organization Expert Consultation, December 2008 [32]](https://thumb-eu.123doks.com/thumbv2/9libnet/5589044.109796/3.892.83.818.306.555/circumference-according-organization-circumfer-circumfer-organization-consultation-december.webp)